https://www.healthcaredive.com/news/hospitals-prepare-for-uncompensated-care-payment-change/530719/

Hospitals will soon get paid for uncompensated care differently, and though supporters of the change say it will create a fairer measurement, hospitals are leery about how the move will affect their bottom lines.
Starting Oct. 1, CMS will begin a three-year phase-in for how it pays hospitals for uncompensated care. No longer will they get paid based solely on a Medicaid, dual-eligible and disabled patient headcount. Instead, hospitals will need to provide patient-level detail of the services performed, as well as total uncompensated care totals.
Rita Numerof, co-founder and president of Numerof & Associates, told Healthcare Dive that counting heads is easier for hospitals, but it’s not always accurate. That distortion can result in institutions having an “unfair advantage” in terms of payments under the Disproportionate Share Hospital program. Instead, CMS will now gauge the actual care experience.
Numerof said the move looks to target flaws in the current payment model and improve transparency and accountability. “I think that looking at the services that are provided rather than just looking at the number of people and making an assumption about what their utilization is is a lot more accurate,” she said.
Chuck Alsdurf, director of healthcare finance policy and operational initiatives at Healthcare Financial Management Association, told Healthcare Dive the change “levels the playing field” for hospitals. However, several issues and concerns remain.
Worksheet S-10 and uncompensated care
CMS recently released its hospital inpatient prospective payment system final rule for fiscal year 2019, which included a provision that will require hospitals to use Worksheet S-10 to provide patient-level compensated care information that can be used to make payments to disproportionate share hospitals.
That patient-level data includes forms in which hospitals must attest to a patient’s eligibility, such as whether the person meets the criteria through disability, dual eligibility or Medicaid.
At the same time, CMS will audit Worksheet S-10 data in the fall and says it will continue provider education efforts and look to improve Worksheet S-10 instructions.
CMS made the change to improve the accuracy in the way that DSH payments are made. “Historically, the approach has been a head-count approach, essentially taking a look and totaling up the number of Medicaid patients, dual patients and those that are disabled,” Numerof said.
The new method isn’t as easy as a headcount, but it improves accuracy and is closer to what a hospital is actually owed.
According to the agency, about half of hospitals that receive uncompensated care payments felt the need to modify their S-10 data. Alsdurf said that’s not a large enough number to assume the data is accurate or reliable. “HFMA members view this as half of the hospitals possibly submitted imprecise data based on vague instructions that impact their hospital payments. So, at the current time, we do not feel this model is clear or accurate enough to utilize for such a significant distribution of funds,” he said.
Critics charge that the change might hurt Medicaid expansion states and help hospitals in states that didn’t expand the program. Now, hospitals calculate Medicaid Patient Days and send that information along to CMS. However, supporters of the change say that non-expansion states with fewer Medicaid recipients now lose out on uncompensated care payments compared to expansion states.
In a letter to CMS about the change, Dallas-based Parkland Memorial Hospital CEO Frederick Cerise said his facility is one of the largest providers of uncompensated care in Texas, which has not expanded Medicaid.
He said Parkland supports the change and called using S-10 data a “more exact measure.” The system provided $2.37 billion in uncompensated care in FY 2015. More than three-fourths of the system’s payer mix is unfunded (nearly half) or Medicaid (almost one-third).
The American Hospital Association agrees that Worksheet S-10 has the potential to provide a more accurate measure of uncompensated care costs. However, Erika Rogan, senior associate director of policy at AHA, told Healthcare Dive in a statement the group has concerns about the “accuracy and consistency of the S-10.”
Meanwhile, America’s Essential Hospitals, which represents more than 325 member hospitals with much of the country’s uncompensated care, sent a 44-page letter to CMS in June listing a series of concerns and recommendations to resolve the issues.
“The high cost of providing complex care to struggling Americans leaves our hospitals with limited resources, driving them to find increasingly innovative strategies for high-quality care,” AEH CEO Bruce Siegel said. “But improving care coordination and quality while staying true to a mission of helping those in need can be a delicate balance. This balance is threatened by payment cuts to hospitals.”
What does the change mean for hospitals?
Uncompensated care costs in community hospitals are on the rise after years of decreases following the Affordable Care Act.
Uncompensated care is bad debt charges plus financial assistance charges. This includes caring for uninsured patients unable to pay their bills. Uncompensated care doesn’t include underpayments from Medicare or Medicaid.
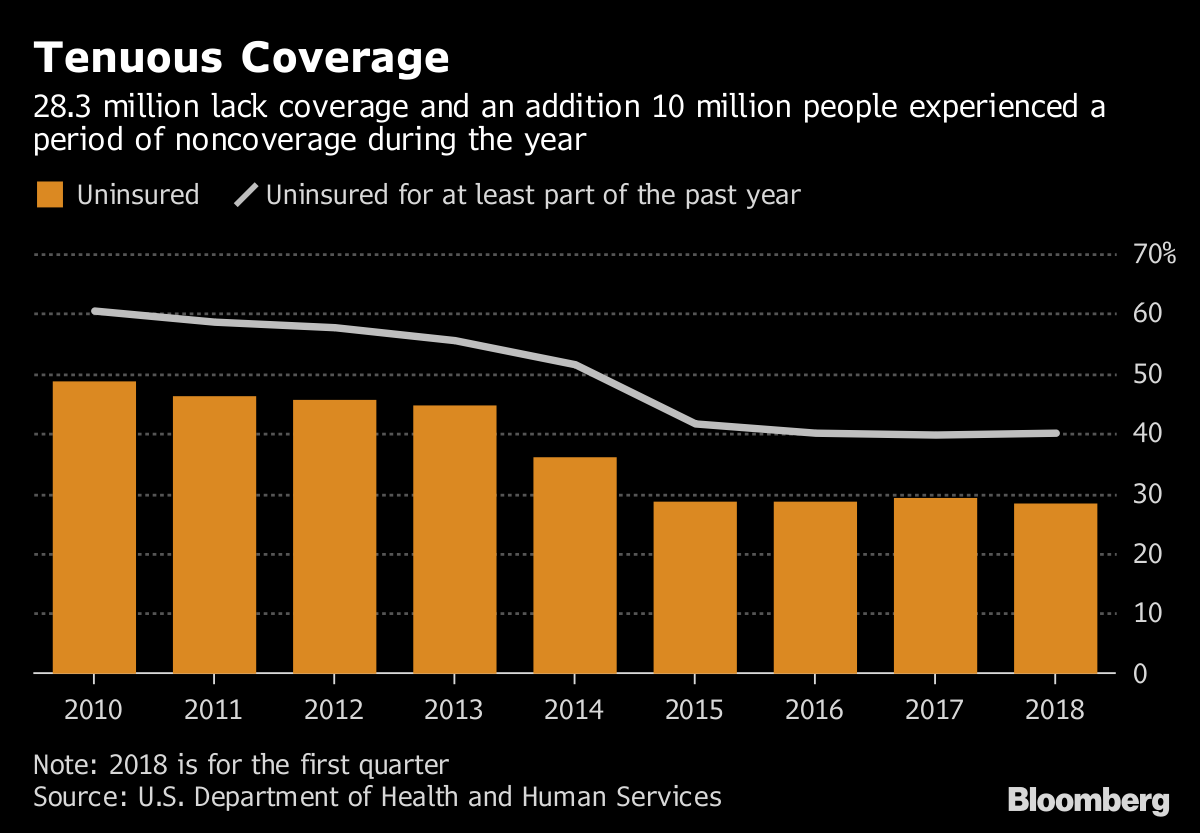
The AHA earlier this year said 4,840 community hospitals provided a total of $38.3 billion in uncompensated care in 2016, up from $35.7 billion at 4,862 community hospitals in 2015. And uninsured numbers have increased in the years since 2016, so those numbers are likely higher now.
Hospitals are concerned about any change that might result in them losing out on uncompensated care funding. However, what the change will mean for hospitals depends on multiple factors, including patient mix, location and how much the facility already relies on uncompensated care payments.
The AHA had hoped CMS would put into place protections to shield hospitals hurt by the change. In its comments to CMS, the hospital group requested a stop-loss policy that would kick in if hospitals lost more than 10% of DSH payments in a year after using the S-10 worksheet. AHA estimated that nearly one-fifth of hospitals might face that problem in FY 2019. AEH also requested a stop-loss policy.
Ultimately, CMS didn’t put in that provision. Numerof said she understands the agency’s choice. Hospitals need to understand where the market is headed and build infrastructure and systems to meet those demands accordingly. She added that no other business would request stop-loss protection based on changes like the S-10.
Concerning community relations, Alsdurf doesn’t expect the change will have an impact. “Hospitals will continue to provide care to those who cannot afford it, so I don’t think this change will have any impact on the community, positive or negative,” he said.
How should hospitals prepare?
There are still questions about the S-10, but hospitals can’t wait for CMS to provide all answers and clarifications. The change is here and hospitals need to move forward with the information available to them.
This process means maximizing uncompensated care payments in the new system. One step is for hospitals to make sure their charity care and bad debt policies are updated and that those policies are followed, so they receive the level of payments they’re owed.
Alsdurf said hospitals are already collecting Medicaid days data. Now they’ll have to add another piece. He expects the change will be minor for reporting and data gathering practices.
“Until they receive feedback from CMS on their data, it’s hard to do much other than make sure they feel good about the data … I’d suggest they begin running reports from their billing systems and reconciling the data (if they haven’t already) to the S-10 worksheet for FY 2014 to present,” Alsdurf said.
He added that hospitals should also continue to review their data as CMS provides more explicit instructions about S-10 in the coming months.