

A UC Berkeley study suggests that provider and insurer consolidation is increasing, reducing competition in regional markets, and leading to higher healthcare prices across California.
In the midst of a nationwide consolidation trend, California is witnessing a swell of mergers among health providers and insurers, resulting in higher prices for consumers and large-scale employers across the state.
A recent study found most counties in California, especially those in the rural northern portion of the state, have highly concentrated hospital markets, noting provider consolidation rose as average insurer consolidation decreased statewide.
The report, released last month by the Nicholas C. Petris Center on Health Care Markets and Consumer Welfare School of Public Health at the University of California, Berkeley, concluded that Californians pay for healthcare services that are “considerably above what a more competitive market would produce.”
Of the 54 counties surveyed, 44 were highly concentrated hospital markets and six were moderately concentrated. According to the study, seven of these counties warrant “concern and scrutiny” by the Department of Justice and the Federal Trade Commission.
The report found from 2010 to 2016, there was a 15% increase in physicians working for a foundation owned by a hospital or health system rather than physician practices, due in part to health system mergers, as well as a 13% increase for primary care physicians, and a 29% increase for specialist physicians.
Additionally, the study found 42 counties surveyed for commercial health plans were highly concentrated while 16 were moderately concentrated. The study also recommended federal agencies review the concentration levels of the insurer market in seven counties.
Breeding anticompetitive behavior
Bill Kramer, MBA, executive director for national health policy at the Pacific Business Group on Health, told HealthLeaders Media the consolidation trend in California is a “serious problem” that employers have been dealing with for years.
Kramer said large health systems, physician groups, and health plans recognize that consolidation leads to increased market power, which in turn provides the opportunity to raise healthcare service prices above what is allowed in a competitive marketplace.
Two weeks ago, California Attorney General Xavier Becerra sued northern California’s Sutter Health, for anticompetitive practices. Sutter, a health system with $12.4 billion in operating revenue in 2017, is charged with foreclosing price competition on its competitors, imposing prices for healthcare services exceeding a competitive market value, and restricting negotiations with insurers to an “all-or-nothing” basis.
Since 2014, Sutter has also been the focus of a class-action lawsuit filed by a grocery worker’s health plan alleging violation of antitrust and unfair competition laws.
“When a provider or any other healthcare entity gains significant market share, it can use that power to negotiate higher prices,” Kramer said. “But they also can put in place mechanisms that strengthen their market power further. That’s what [Becerra] and complainants in this other lawsuit have alleged, that anticompetitive behavior further strengthens their market power and their ability to raise prices. It’s all part of the same picture.”
State and federal blocks on insurers, not providers
Becerra’s lawsuit against Sutter is not the first time state or federal officials have stepped in to address concerns in California’s healthcare industry.
In June 2016, California Insurance Commissioner Dave Jones requested the federal government block the proposed Aetna-Humana merger, citing concerns about an “already heavily concentrated commercial insurance” market. A federal judge agreed with his request and blocked the move in January 2017.
Despite recent and growing recognition among state and federal officials that action must be taken, Kramer says provider consolidation remains an issue without a simple solution. Efforts to enact antitrust statutes against health system mergers in recent years have not always been successful, and are often looked at as the “nuclear option” by industry watchers.
A potential path to offsetting provider consolidation is greenlighting insurer consolidation, though Kramer says there is mixed evidence about whether that would be effective. He said some argue that two large industries competing against each other can result in lower prices, while others claim there is no guarantee that consumers will see lower prices if savings are secured by insurers.
The Berkeley report recommends legislative and regulatory action to address “significant variation” in prices and Affordable Care Act (ACA) premiums across the state, specifically suggesting the implementation of reference pricing by public marketplaces and private employers.
Kramer says the consolidation dilemma is not unique to California, which offers state officials a chance to adopt proactive measures taken by other states to address rising healthcare costs associated with consolidation.
In 2011, Massachusetts Attorney General Martha Coakley authored a report similar to the Berkeley study that analyzed the rise in high prices due to health system mergers. The study ultimately led to the creation of the Health Policy Commission in 2012, with the purpose of monitoring healthcare prices in the state.
NoCal versus SoCal
Another important aspect of the consolidation trend in California is the divide between the rural northern counties and the more populous southern metropolitan area.
Northern California is a sparsely populated region dominated by large health systems, giving insurers less leverage to negotiate prices. A 2017 study from the Bay Area Council Economic Institute (BACEI), the Center for Health Policy at Brookings, and The Nelson A. Rockefeller Institute of Government found that the hospital concentration in northern counties, where only two insurers cover the entire region, is five times higher than the Inland Empire.
Micah Weinberg, PhD, president of BACEI, told HealthLeaders Media the consolidation trend is not tied to one particular factor such as geography.
BACEI’s report cited the consolidation of a few health systems in northern California as a “perennial concern” and driver of rate variation between regions. However, Weinberg said that when low-price, for-profit systems in southern California are removed from the equation, there is a fair amount of parity between prices charged there compared to those charged in northern California.
Related: 3 Reasons Why Health Insurers and PBMs Are Merging
According to Weinberg, another aspect to California’s healthcare market that affects prices has been the implementation of a “very successful experiment” in managed competition through the state exchange. In 2010, California became the first state to create its own insurance marketplace under the ACA.
He argues that Covered California, the state’s insurance marketplace, has standardized healthcare products, instituted financial incentives for providers to embrace limited networks, and fostered competition.
“What that does is it emphasizes the importance of not only payers and providers, but of the structure of the marketplace, in which consumers are making choices across different provider groups linked to particular insurance plans,” Weinberg said.
The BACEI report did cite the ACA as an unintended driver of increased regional consolidation among providers, which has made achieving profitability in northern California a challenge for insurers such as UnitedHealth Group Inc., which exited the statewide ACA marketplace entirely in 2016.



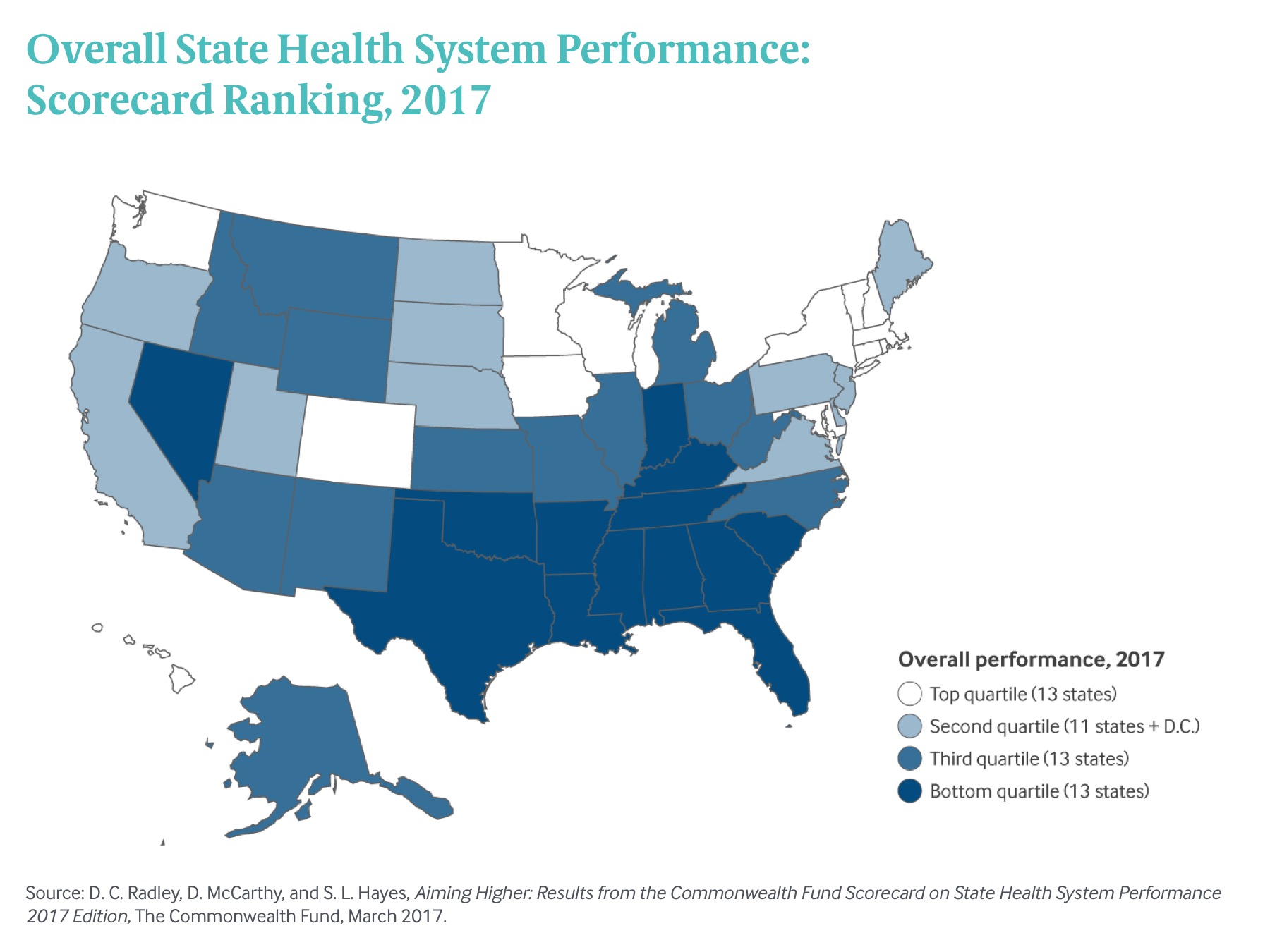
 Exhibit 1: Overall State Health System Performance: Scorecard Ranking, 2017
Exhibit 1: Overall State Health System Performance: Scorecard Ranking, 2017













