Likely Republican Campaign Plan: Replace the ACA with Devolution and Deregulation
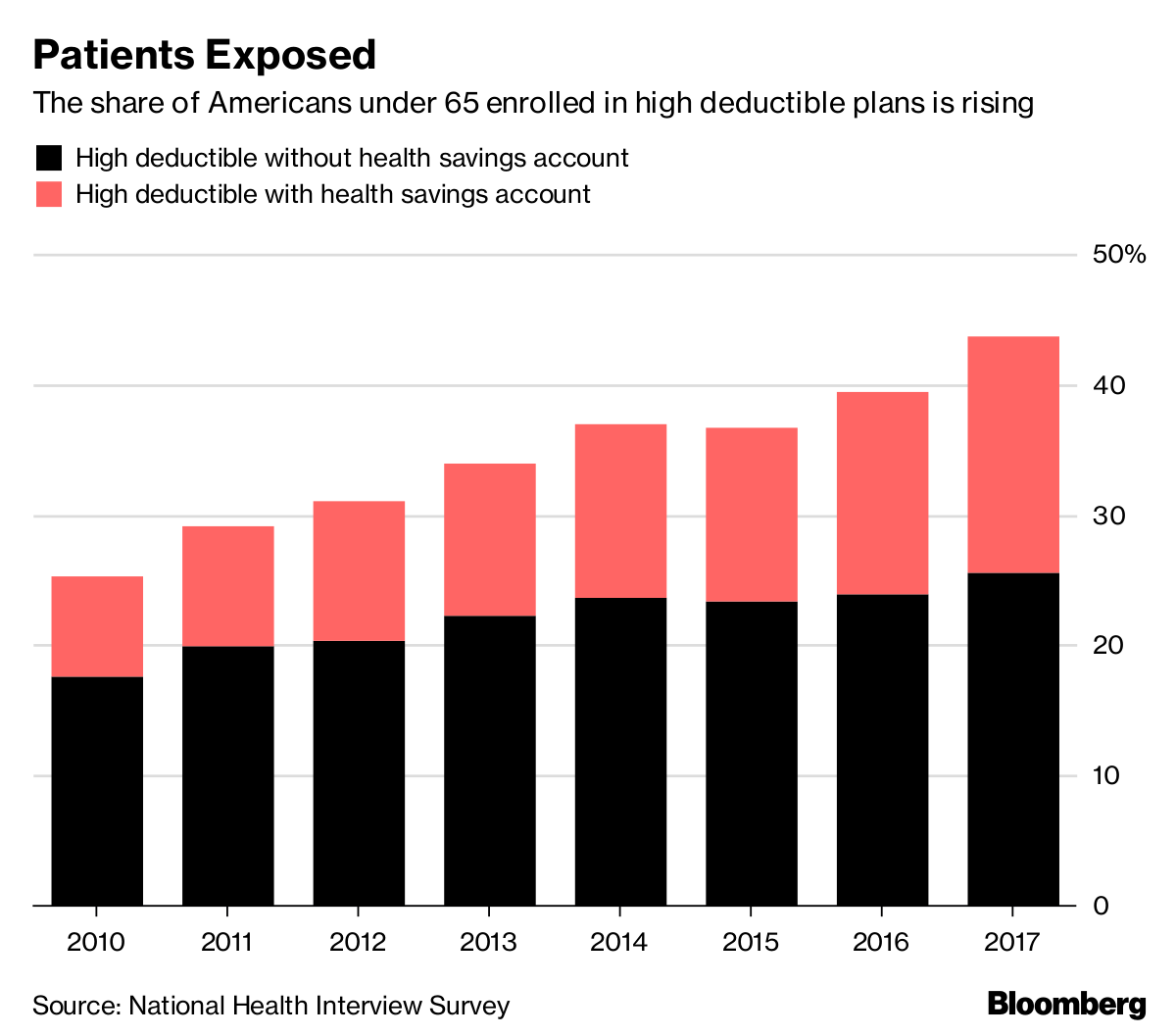
President Trump has indicated he will run for reelection in 2020.51 His fiscal year 2019 budget included a proposal “modeled closely after the Graham-Cassidy-Heller-Johnson (GCHJ) bill.” It would repeal federal financing for the ACA’s Medicaid expansion and health insurance marketplaces, using most of the savings for a state block grant for health care services. It would also impose a federal per-enrollee spending cap on the traditional Medicaid program. States could waive the ACA’s insurance reforms.52 The congressional bill also would repeal the employer shared responsibility provision (i.e., the employer mandate) and significantly expand tax breaks for health savings accounts, among other policies.53 The framework for this proposal — repealing parts of the ACA, replacing them with state block grants, reducing regulation, and expanding tax breaks — is similar to the 2016 Republican platform.
Trump may continue to express interest in lowering prescription drug costs. In 2016 and early 2017, he supported letting Medicare negotiate drug prices54 — a policy excluded from the 2016 Republican platform and his proposals as president. His 2019 budget seeks legislation primarily targeting insurers and other intermediaries that often keep a share of negotiated discounts for themselves.55 On May 11, 2018, he released a “blueprint” to tackle drug costs, including additional executive actions and ideas for consideration. Polls suggest that prescription drug costs rank high among health care concerns.56
One policy initiative in the recent Republican platforms but not embraced by the president is Medicare reform. The idea of converting Medicare’s defined benefit into a defined contribution program and raising the eligibility age to 67 was supported by Vice President Mike Pence when he was a member of Congress and by Speaker of the House Paul Ryan.57 Major Medicare changes were excluded from the 2017 ACA repeal and replace proposals. In contrast, versions of Medicaid block grant proposals appeared in various bills, including the GCHJ amendment, as well as numerous Republican presidential platforms.
Historically, presidents running for reelection have limited competition in primaries. Those challengers, by definition, emphasize their differences with the incumbent, which may include policy. It may be that John Kasich will run on maintaining the ACA Medicaid expansion but otherwise reforming the program (his position as governor of Ohio throughout 2017). Or, Rand Paul could campaign on his plan to repeal even more of the ACA than the Republicans’ 2017 bills attempted to do. Incumbents tend to have slimmer campaign platforms than their opponents in general and primary elections, since their budget proposals, other legislative proposals, and executive actions fill the policy space (see Reagan, Clinton, George W. Bush, Obama). Exceptions include George H. W. Bush, who in 1992 developed a plan given voters’ concerns about health; and Nixon, who offered a proposal for health reform at the end of his first term.
Likely Democratic Campaign Plan: Improve the ACA and Add a Public Plan
It is possible and maybe probable that the ultimate Democratic Party platform in 2020 will resemble that of 2016: build on the ACA and include some sort of public plan option. Legislation has been introduced during this congressional session that builds on the law by extending premium tax credits to higher-income marketplace enrollees (e.g., Feinstein, S. 1307), lowering deductibles and copayments for middle-income marketplace enrollees (e.g., Shaheen, S. 1462), providing marketplace insurers with reinsurance (e.g., Carper, S. 1354), and strengthening regulation of private market insurance (e.g., Warren, S. 2582). Some proposals aim to increase enrollment following the effective repeal of the individual mandate, by, for example, raising federal funding for education and outreach, and testing automatic enrollment of potentially eligible uninsured people (e.g., Pallone, H.R. 5155). These proposals would have different effects on health insurance coverage, premiums, and federal budget costs.58
The Democrats will inevitably discuss a public plan in their platform, although the primary contenders will most likely disagree on its scale (e.g., eligibility) and design (e.g., payment rates, benefits).59 In September 2017, Senator Bernie Sanders introduced the Medicare for All Act (S. 1804). It would largely replace private insurance and Medicaid with a Medicare-like program with generous benefits and taxpayer financing. “Medicare for more” proposals have also been introduced: Medicare Part E (Merkley, S. 2708), an option for individuals and small and large businesses; Medicare X (Bennet, S. 1970), which is available starting in areas with little insurance competition or provider shortages; and a Medicare buy-in option, for people ages 50 to 65 (Higgins, H.R. 3748). A Medicaid option (Schatz, S. 2001), similar to Medicare Part E, offers a public plan choice to all privately insured people, aiming to capitalize on the recent popularity of that program. Publicly sponsored insurance plans have long been included in Democratic presidents’ platforms, although the government’s role has ranged from regulating the private plans (Carter, Clinton) to sponsoring them (Truman, Obama). It may be that the candidate who prevails in the primaries will determine whether the Democratic platform becomes “Medicare for all” or “Medicare for more.”
This may be the extent of Medicare policies in the 2020 Democratic platform. Relatively high satisfaction and low cost growth in Medicare have limited Democratic interest in Medicare policy changes in recent years. Similarly, Democrats have not introduced or embraced major reforms of Medicaid. However, the public concern about prescription drug costs has fueled Democratic as well as Republican proposals, some of which target the drug companies (e.g., addressing “predatory pricing,” allowing Medicare rather than prescription drug plans to negotiate the prices for the highest-cost drugs).60
Discussion
Predictions about presidential campaigns have inherent limits, as many experts learned in the 2016 election. Events concerning national security (e.g., conflict), domestic policy (e.g., a recession), or the health system (e.g., a disease outbreak) could alter the policy choices of presidential candidates. New ideas could emerge, or candidates could take unconventional approaches to improving the health system. And, while campaign plans have relevance, the long history of attempts at health reform underscores that by no means are promises preordained.
That said, perennial policies and recent political party differences will likely figure in 2020. Republican presidential candidates, with few exceptions, have adopted a small government approach to health reform: shifting control to states, cutting regulation, preferring tax breaks and block grants over mandatory federal funding, and trusting markets to improve access, affordability, and quality. Democratic presidential candidates have supported a greater government role in the health system, arguing that market solutions are insufficient, and have defended existing programs like Medicare, Medicaid, and, now, the ACA. Some will probably support the government’s taking a primary role in providing coverage given criticism of the efficacy and efficiency of private health insurers. The direction and details of the campaign plans for 2020 will be developed in the coming months and year. Given such plans’ potential to shape the next president’s agenda, now is the time to scrutinize, modify, and generate proposals for health reform.