A wave of coordinated lawsuits is transforming the No Surprises Act’s arbitration system into a battlefield where insurers seek to intimidate physicians, rewrite the law and consolidate control.
As I have written, Congress passed the No Surprises Act (NSA) to safeguard patients from unforeseen medical expenses and establish a neutral, independent dispute resolution (IDR) process for payment conflicts between insurers and out-of-network providers. That design was meant to replace brinkmanship with an independent referee. What Congress designed as a neutral arbitration system is now being challenged by Big Insurance through coordinated litigation designed to narrow, intimidate, and ultimately reshape the law.
Major insurance conglomerates — including UnitedHealthcare entities, Elevance/Anthem affiliates and Blue Cross Blue Shield plans — have launched a coordinated series of federal lawsuits against providers, hospitals, and revenue-cycle vendors who have used IDR at scale. Employing nearly identical language, legal arguments, and allegations, these lawsuits are not isolated ordinary litigation. It is lawfare.
Narratively, these suits recast lawful engagement in the NSA’s IDR process as “abuse,” but functionally they are designed to intimidate physicians from seeking NSA protection. A Pennsylvania suit from UnitedHealthcare against NorthStar Anesthesia presents the most urgent and perilous threat to independent physicians. If Unitedhealthcare prevails, insurers will be able to obtain judgments of fraud against physicians who incorrectly file NSA disputes. The effects of this will be catastrophic for independent physician practices, who cannot afford to litigate against billion dollar behemoths that have armies of lawyers on staff and retainer.
If successful in these efforts, the insurers will further weaken physician practices and make them ripe for acquisitions, continuing the dangerous path of vertically integrated insurance corporations – and the further decimation of independent physician practices.
The “Flooding” Myth
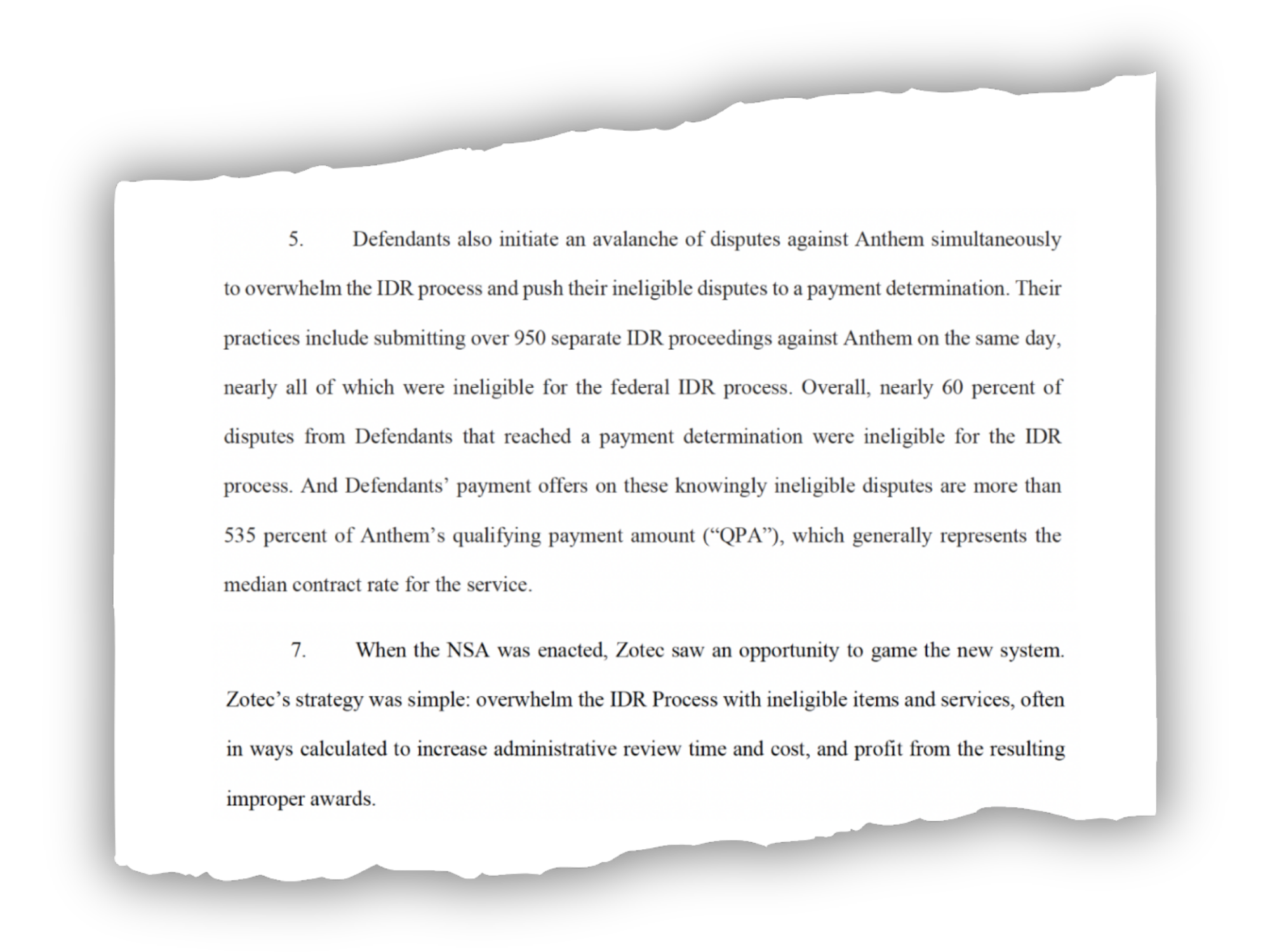
The lawsuits all start in a similar fashion. Each one claims that the defendant “abused” federal legislation “designed to protect patients from unexpected medical bills” and asserts that “the IDR process has not functioned as intended.” This wording appears verbatim in cases filed months apart, across different jurisdictions, against completely different defendants. Insurers adopt the same basic allegation: providers or billing companies “flooded,” “overwhelmed,” or unleashed an “avalanche” of IDR disputes that insurers assert were ineligible.
Those characterizations are based on bad data. Before the NSA went into effect, the Departments of Health and Human Services, Labor, and Treasury projected that the independent dispute resolution (IDR) process would see roughly 17,000 disputes annually. In reality, the system received nearly hundreds of thousands of disputes in its first year. That mismatch didn’t happen by accident. The departments based their projections on New York’s experience with a state arbitration system, scaling the state’s dispute numbers nationally. But New York’s law relied on an independent benchmark called FAIR Health that sharply reduced disputes. This is a structural feature the federal law does not have.
A more realistic comparison was available at the time: Texas. Unlike New York, Texas operated an arbitration system without an external benchmark making it a better comparison for the federal No Surprises Act. In its first year, the Texas system received nearly 49,000 arbitration requests for a population of just under six million people. That experience should have been a clear signal that arbitration volume would be far higher than federal projections suggested. Insurers have used this modeling error to their rhetorical advantage in their litigation.
Last week, the war in Iran intensified and Kristi Noem’s tenure as DHS Secretary came to an unceremonious close. Perhaps lost in the noise was the February jobs report issued Friday by the U.S. Bureau of Labor Statistics. It showed a surprising decline in job growth prompting speculation the economy might have taken a downward turn. Some headlines….
Payrolls unexpectedly fell by 92,000 in February; unemployment rate rises to 4.4% (CNBC)
Employers Cut Jobs in Sign of a Shakier Economy (New York Times)
Paychecks keep rising for American workers, providing boost to household budgets (Fox Business):
The U.S. economy lost 92,000 jobs in February, stoking labor market worries (NBC News)
The US economy lost 92,000 jobs in February and the unemployment rate rose to 4.4% (CNN)
Anticipation that the jobs report portends bad news for the economy followed the news cycle all day and through the weekend. And a few, like Axios, went further: “The surprise to many was where the biggest since job growth especially in healthcare and social assistance had buoyed the labor market for 3 years.” Others attributed the decline to hangovers from recent nursing strikes (USC Keck, Kaiser Permanente, MarinHealth) and layoffs by many health systems.
To industry insiders, the BLS jobs report’s capture of declines in healthcare hiring was no surprise. Operating cost reduction has been a strategic imperative in every hospital, long-term care, ancillary and medical group since the pandemic (2020). In tandem, investments in workforce productivity enhancements via technology-enabled workforce redesign and performance-based compensation have elevated human resource management to C-suite status in most organizations. It’s understandable:
Healthcare is capital intense: it needs appropriations from government and in-flows from employers and individual taxpayers to pay its bills. Most of that pays for its labor costs. Today, most Board agenda include updates on labor relations, human resource management issues and workforce adequacy—it’s standard fare. And all weigh options to outsource and devour progress reports from HR management on AI-enabled investments anticipated to reduce labor costs.
Healthcare is highly regulated, especially in workforce activities, and labor-management relationships impact organizational performance and reputation. Every sector in healthcare is regulated by combinations of federal, state and local rules, laws and agency directives that define roles, responsibilities, decision-rights and constraints of its workforce. It’s complicated by the politics of healthcare which avoids policy changes that threaten protections sought by each labor cohort in healthcare. Protecting funding and restricting infringement on scope of responsibility by unwanted outsiders is the primary rationale for professional society’ advocacy efforts. In hospital and long-term care settings, the healthcare workforce is a cast-system that keeps doctors at the top of the pyramid, licensed mid-levels in the middle and everyone else below. In other healthcare settings, executive-level designations dominate hierarchies, and in some Boards play roles in workforce structure and compensation schemes. Workforce modernization in most healthcare settings is acknowledged as a critical need but most default to layoffs and fail to enact a comprehensive strategy.
Looking ahead, technology will alter the status quo for workforce modernization efforts in healthcare:
1-Less dependence on physician recommendations. Might patients access customized clinical decision support tools more widely in the future and make more choices themselves (especially if incentives support self-care)? Might other sources of clinical counsel be more accurate, more accessible and less costly in the future, prompting acceptance (trust and confidence) by patients? Physicians and other caregivers will play key roles, but in concert with tools and processes that enable consumer engagement.
2-More access to verifiable cost, price and value information. The underlying costs and prices for healthcare services are unknown to their caregivers at the points of care so the majority of transactions require pre-authorization by a third-party adjudicator with payments that follow. Physicians bear no responsibility for advising patients about costs and prices: theirs is exclusively the domain of clinical counsel. Thus, labor costs in healthcare presume third party payments, middlemen, incapable self-care and work rules that reinforce old ways and torpedo better ways of work. Might the role and scope of insurer activity be integrated with delivery so that “costs and quality” are directly accountable to providers? Might primary and preventive health hubs (physical + behavioral + nutrition + prophylactic dentistry + self-care enablement + insurance) become the centerpieces of community health replacing traditional insurers and hospitals? Where will the workforce choose to work?
Per the Healthcare Workforce Coalition (www.healthcareworkforce.org), healthcare workforce shortages are a near and present danger to the U.S. health system: shortages of physicians, nurses and allied health professionals are significant, especially in rural areas. The 18-million who constitute the healthcare workforce today are being told to work harder with less. It’s no secret.
In the Affordable Care Act (2010), Title 5 (Section 5101), healthcare workforce modernization was authorized: “The purpose of this title is to improve access to and the delivery of health care services for all individuals…” Subtitle B authorized creation of a 15-member National Health Care Workforce Commission to recommend modernization policies. It would have coordinated workforce initiatives across federal agencies (HRSA, CMS, MedPAC, MACPAC, GAO, et al) along with states and private sector operators to address long-term issues and short-term execution challenges. The Commission never met because its funding was not authorized by Congress.
If the overall economy is dependent on healthcare to produce an appropriate share of job growth while reducing overall costs, modernizing its workforce is key. It must include unpaid caregivers, licensed and unlicensed providers and technology-enabled solution providers—not just traditional licensed professional groups and their academic partners. That’s not going to happen in the current political environment where each sector’s primary focus is protecting reimbursement and guarding against scope of practice threats.
The health system needs transformation. Workforce modernization is where to start.
Paul
P.S. My journey as a heart patient continues to teach me just how far we have to go as a “system.” Understanding what I have been billed for, by whom, when and why is like reading Russian. As best I can see, $267,490.30 has been charged by the hospital and 13 different doctors who’ve treated me in some way. How much I end up spending after rehab et al remains a mystery but it’s not remotely close to the hospital’s “price estimator” tool. Little wonder consumers are frustrated about healthcare costs pushing its affordability to the top of their Campaign 2026 concerns.
Last Tuesday, HCA, the largest investor-owned hospital system, released their Q4 2025 and year-end earnings and they’re impressive. The 190-hospital system reported:
Net income of $6.8 billion in 2025, a 17.8% increase year over year.
Revenue of $75.6 billion, a 7.1% increase year over year.
On a same facility basis, growth in revenue of 6.6%, equivalent admissions of 2.4% and net revenue per equivalent admission of 4.1% versus prior year.
For 2026, projected a net income between $6.5 billion and $7 billion and adjusted EBITDA between $15.6 and $16.5 billion on revenue between $76.5 billion and $80 billion.
CFO Mike Marks told the 16 analysts on the investor call “Consolidated adjusted EBITDA increased 12.1% over prior year, and we delivered a 90-basis point improvement in adjusted EBITDA margin. Cash flow from operations was $2.4 billion in the (4th) quarter and $12.6 billion for the year. This represents a 20% increase in operating cash flow in 2025 over full year 2024.”
And CEO Sam Hazen added “Let me add to just the whole resiliency agenda. This is not an episodic event for us. It just happens to be a maturation of what in my estimation is cultural within HCA, and that is being cost effective in finding ways to leverage scale, utilize best practices. Now we have tools… that are in front of us as opportunities to create even more consistency, efficiencies and transparency in the company’s overall cost. And that’s why the program is lining up in a well-timed manner with some of the enhanced premium tax credit challenges.
But we see this program continuing to mature. And as we get more capable at using these tools, it’s going to help us find even more opportunities. But this is not a onetime event. It’s a cultural dynamic in our company around being cost effective, being high quality and finding ways to improve from a process standpoint and a leverage standpoint with our overall scale.”
Shares of HCA closed at $488.27 last week, down from its peak at $527.55 (January27). Per MarketWatch, “shares of HCA Healthcare Inc rose $1.19% to $488.27 Friday on what proved to be an around grim trading session for the stock market, with the S&P Index falling 0.43% to 6939.03 and Dow (DJIA) falling 0.36% to 48,892.47. The stock demonstrated a mixed performance when compared to some of its competitors Friday, as Community Health Systems (CYH) rose 1.26% to $3.21 and Tenet (THC) fell 0.11% to $189.28.”
Hospital stock market analysts are keen to gauge how companies like these are navigating choppy waters for healthcare. It’s understandable: Healthcare is one of the 11 sectors that comprises the overall S&P 500 and is 9.6% of its weighting. Historically, the healthcare index had beaten the S&P (30-year average 9% vs. 8% overall) but in recent years, it has lagged largely because regulatory policy changes and healthcare budget volatility dampened investor confidence.
Investors are increasingly hedging their bets in healthcare services reasoning even market bell-weathers like HCA face headwinds. And that sentiment has profound impact on operators in not-for-profit health sectors like community and rural hospitals, nursing and home care and ancillary services like EMS, hospice care and others that see their credit-worthiness slipping and costs for debt capital increasing.
My take
HCA is not an exception. It is culturally geared to the business of running hospitals and amassing scale in its markets vis a vis outpatient services and physician relationships. It follows a playbook geared to earnings per share and strategic deployment of capital to optimize its ROC, and it rewards its leaders accordingly. These are not unique to HCA.
And, like other systems, HCA is a lightning rod for critics. Studies have shown for-profit hospitals lean on staffing, aggressive on procurement, concerning to physicians and increasingly problematic to private insurers. Those same studies have shown quality of care to be comparable and charity care to be at or above same-market competitors. But this discipline also enables a higher price to cost ratio, a better payer mix and pruning of clinical services where margins are thin. Again, leverage in payer contracts and high pricing are not unique to the HCA playbook. Some not-for-profit systems have done the same or better.
What’s unique for each system like HCA are 1-the markets in which they enjoy leverage by virtue of scale and 2-the aggressiveness whereby they use their leverage. Ownership status—not for profit vs. investor-owned—matters in some markets and organizations more than others. But market dominance by any system, and how it’s leveraged, is a differentiator.
Case in point: In Asheville NC, HCA’s Mission Health dominates. HCA paid $1.5 billion for the legacy Mission-St. Joseph’s system in 2019. Despite, difficult media coverage and 3 warnings from CMS about quality shortcomings, it’s profitable.
On December 10, 2025, I had quadruple by-pass surgery there. Over the course 2 ED visits in November, the 5-day inpatient stay and post-surgical interactions since, I had the opportunity to see its operations firsthand. The bottom line for me is this: HCA Healthcare is a successful business. It operates Mission aggressively and profitably. Every employee knows it. Staffing is lean. There are no frills. Coordination of care is a crap shoot: connectivity between offices, services, and physicians is limited; price transparency is a joke and care navigation for patients like me is haphazard. But all say patient care is not compromised as my surgical experience confirmed. Every hospital aspires for the same. All are trying to do more with less.
HCA’s financial success is not the exception in acute care, but it’s certain to draw attention to business practices that enable results like it enjoyed last year across the spectrum of hospital care. And it’s certain to intensify competition between hospitals to get the upper hand.
References in addition to citations in the sections that follow:
Bipartisan bill modeled on the 1933 Glass-Steagall Act would require health care conglomerates to divest vertically integrated subsidiaries.
Today, Senate ideological-opposites, Sen. Josh Hawley (R-Mo.) and Sen. Elizabeth Warren (D-Mass.), introduced the Break Up Big Medicine Act, a Glass Steagall Act for health care. From the right, Hawley has built a reputation as a populist critic of corporate exploiters. From the left, Warren has spent years hammering Wall Street and Big Tech for their grip on markets. Together, their new bill aims at the corporate, monopolistic conglomerates that now control much the U.S. health care system — particularly where Big Insurance and its subsidiaries blur the lines between health delivery and Wall Street calculations.
At its core, the legislation prevents common ownership of a medical provider organization and one or more of the following: an insurance company, pharmacy benefit manager (PBM), or a prescription drug or medical device wholesaler. The bill requires individuals who currently own, operate, or control both types of entities to divest from one category (either the provider organization or the insurer, PBM, or wholesaler) within one year of the bill’s enactment. Failure to do so would result in penalties and enforcement from the Federal Trade Commission.
Why “Glass-Steagall for Health”?
The original Glass-Steagall Act was enacted in June 1933 during the Franklin Roosevelt administration. Congress and Roosevelt believed it was imperative to break up the risky entanglement of commercial and investment banking, which contributed to the 1929 stock market crash that led to the Great Depression. Millions of Americans lost their life savings when thousands of banks failed and confidence in the country’s financial system collapsed. The Glass-Steagall Act helped separate banks from speculative securities operations, established the Federal Deposit Insurance Corporation (FDIC) to protect depositors and for decades served as a regulatory firewall that protected Americans’ savings.
In recent years, health insurers have morphed into Wall Street-controlled bank-like institutions that bear little resemblance to the nonprofit organizations most of them were just a few years ago. In fact, many of the country’s biggest health insurers are essentially financial institutions that also own a health insurance company.
Today’s major players are not just covering (and not covering) our health care costs — they are amassing profits across a sprawling set of subsidiaries that have mutated these health insurers into monopolistic corporations similar to the “trusts” Franklin Roosevelt’s cousin Teddy ordered broken up and to the vertically integrated banking titans of the 1920s.
For example:
UnitedHealth Group, owner of UnitedHealthcare (a health insurer), also owns Optum Bank (which has more HSA assets under management than any other financial institution), Optum Ventures, Change Healthcare, PBMs, speciality pharmacies, and over 2,000 medical provider organizations;
CVS Health operates both insurance products (through Aetna) and PBMs (through Caremark) and owns a major pharmacy retail chain that shapes prescription pricing and competition;
Cigna has been bringing in far more revenue from the pharmacy supply chain since it bought Express Scripts in 2018 than from its many health plans; and
Elevance, which operates Blue Cross plans in 14 states, also owns a PBM, clinical operations and, like UnitedHealth, a financial institution with millions in HSA assets under management.
The joint ownership of insurance companies, PBMs, medical provider organizations, and pharmacies allows the parent companies to game a little known regulation called the medical loss ratio (MLR). The ACA requires that insurers have MLRs of at least 80-85%, meaning they must spend 80-85% of premium dollars on medical care. When insurance companies own a PBM, a provider group or pharmacy, they can count premium dollars they “spend” with to those entities as “medical care” for purposes of the MLR, when in reality they are self-dealing – and often inflating the amount they pay their affiliated providers to meet the MLR requirements and avoid sending rebates to their customers for noncompliance. As a consequence large health care conglomerates have little if any incentive to contain costs. The self-dealing actually drives costs higher while enabling them to convert more premium dollars to profits than Congress intended when it included the MLR provision in the Affordable Care Act.
Taken together, Big Insurance profits from vertical integration by pooling their subsidiaries’ reach and capital, investing in and paying themselves and influencing the cost of and access to care for millions of Americans throughout the health care ecosystem.
The fact that Hawley and Warren are uniting on this important legislation is reflective of the broader national conversation about the nation’s health care affordability issue, which has created a medical debt crisis that a broad-swath of Americans now blame on Big Insurance.
Warren and Hawley recognize the critical importance of structurally separating companies within our health care system to protect patients and make prices more affordable.
The original Glass-Steagall Act was passed after many banks had already become insolvent. The Break Up Big Medicine Act could prevent a similar catastrophe.
A new report from the Republican-led Senate Judiciary Committee describes how UnitedHealth Group has turned a safeguard for sick patients in the Medicare Advantage program into a profit-making strategy.
The report, How UnitedHealth Group Puts the Risk in Medicare Advantage Risk Adjustment, details how Medicare Advantage (MA) payments (seemingly designed to compensate health insurers more for enrolling patients with greater health needs) have increasingly rewarded insurers with the resources, data and scale to capture and maximize diagnosis codes. According to the committee, UnitedHealth Group has leveraged its size, vertical integration and advanced data and AI capabilities to consistently stay ahead of efforts by the Centers for Medicare & Medicaid Services to curb excess payments tied to coding intensity.
Read the U.S. Senate Judiciary Committee’s How UnitedHealth Group Puts the Risk in Medicare Advantage Risk Adjustment here.
After reviewing more than 50,000 pages of internal UnitedHealth documents, Judiciary Committee investigators found that the company built a vast diagnosis-capture infrastructure that includes in-home health risk assessments, secondary chart reviews, “pay-for-coding” arrangements with providers, and tightly controlled clinical workflows within UnitedHealth-aligned medical practices. These efforts, the report states, go well beyond neutral documentation and instead amount to an aggressive strategy to maximize risk scores and, by extension, federal payments.
The committee, chaired by Sen. Chuck Grassley, (R-Iowa), warns that even when CMS attempts to rein in abuse (such as excluding more than 2,000 diagnosis codes from the risk-adjustment model) UnitedHealth appears uniquely positioned to identify new, untapped diagnoses among the thousands that remain. Because UnitedHealth also sells its diagnostic criteria, coding tools and workforce to rival insurers, its strategies can quickly spread across the entire Medicare Advantage market.
The report concludes with this:
While Senator Grassley’s staff will continue to evaluate the information produced by UHG, this initial review has revealed how UHG has been able to profit from the way that CMS risk adjusts payments to MAOs. The investigation has also shown that risk adjustment in MA has become a business in itself—by no means should this be the case. MAOs should receive payments that are commensurate to the complexity and acuity of the Medicare beneficiaries that they insure, not their knowledge of coding rules and their ability to find new ways to expand inclusion criteria for diagnoses. Taxpayers and patients deserve accurate and clear-cut risk adjustment policies and processes.
But what makes these findings especially notable is who commissioned the investigation in the first place. Grassley was one of the original architects and longtime champions of Medicare Advantage when it was enacted back in 2003. In recent years, he now warns that the program’s “promise of efficiency and choice” has been undermined by vertical consolidation, blinded oversight and systemic risk-code gaming.
In past inquiries — spurred by reporting from outlets like The Wall Street Journaland findings from the Health & Human Services’ Office of Inspector General — he has demanded answers from UnitedHealth over the use of in-home assessments and chart reviews that allegedly drove billions of dollars in additional payments to the company.
Continuing the bipartisan scrutiny of MA insurers, CMS recently released its proposed payment rates for MA plans in 2027. Notably, CMS is proposing to exclude diagnosis codes added to a patient’s chart during chart reviews by AI or insurers from their risk score; something many reform advocates and I have long supported. These changes and this investigation are important steps in reining in the abuses by MA insurers and reason for hope we are on the right track.
Last week, J.P. Morgan hosted its 44th annual healthcare conference, with over 500 companies and 8,000 people in attendance to discuss health system performance, pharmaceutical trends, and new AI offerings.
Health systems outline current performance, future plans
According to STAT, many health systems took a measured tone at this year’s conference, focusing largely on stability and consistency, especially in the face of significant Medicaid funding cuts from the One Big Beautiful Bill Act.
“For me, it’s been about stabilizing,” said Kevin Smith, CFO of SSM Health. “Taking a look at the operations, doing a lot of blocking and tackling. Getting back to the basics.”
Separately, Paul Rathbun, outgoing CFO at AdventHealth, said that “[i]t all begins and ends with consistent financial performance.” He also emphasized sustainability and the importance of a solid foundation to handle future uncertainty.
As hospitals and health systems face financial challenges, many are focusing on boosting efficiency and reducing expenses. For example, Intermountain Health is focusing on optimizing its supply chain and simplifying healthcare with value-based arrangements.
Some health systems, like CommonSpirit Health, are planning to sell some facilities to help boost finances and expand ambulatory networks. Providence is also considering selling some of its assets, potentially including some hospitals.
“We have 51 hospitals, most of which have No. 1 market share in their communities, but we do have a handful that we may have to find a different purpose or different sponsors for,” said Providence CFO Greg Hoffman.
Other health systems, like Mass General Brigham and Hackensack Meridian, are aiming to expand their partnerships with other providers or outside organizations. Currently, Mass General Brigham has a new ambulatory care venture with Tampa General Hospital, and Hackensack Meridian is planning to add 20 new primary care clinics in New Jersey with Amazon One Medical.
Top CMS officials meet with hospital, insurance leaders
At the conference, CMS Administrator Mehmet Oz, along with four top members of his staff, hosted an event with hundreds of top hospital and health insurance leaders to discuss the Trump administration’s healthcare policies.
During the event, Oz downplayed the potential impact of upcoming Medicaid cuts, saying that they won’t be felt for at least a year and a half. “The catastrophizing over the idea that it’s going to rip the guts out of the system, I don’t think that’s fair,” he said.
CMS leaders also discussed efforts to combat fraud, the Trump administration’s focus on deregulation, recent vaccine changes, and more.
“The catastrophizing over the idea that it’s going to rip the guts out of the system, I don’t think that’s fair.”
According to David Joyner, CEO of Hill Physicians Medical Group, the general mood among attendees was skeptical and pessimistic, particularly about cuts to Medicaid and the impact of declining Affordable Care Act membership. At the same time, people were curious and optimistic about CMS’ potential to promote new innovation and technology that could address some of the healthcare industry’s most persistent challenges.
AI offerings continue to expand
AI was a large focus of the conference, with many organizations announcing new tools or collaborations.
At the conference, Anthropic announced Claude for Healthcare, a new AI model that includes HIPAA-ready infrastructure for enterprise customers, native integration to commonly used medical and scientific databases, and a model specifically trained for healthcare and life sciences tasks.
The new model follows Claude for Life Sciences, which was launched last October. Anthropic also announced new capabilities for life sciences, which ranged from preclinical research and development and regulatory affairs.
According to Eric Kauderer-Abrams, head of biology and life sciences at Anthropic, healthcare and life sciences are one of the company’s largest bets.
“Anthropic is a very natural fit for the healthcare and life sciences world because our identity as an AI company is built around safety and responsibility and rigor and reproducibility, and these are all the central tenants of the healthcare and life sciences industries,” Kauderer-Abrams said.
Currently, several healthcare organizations already use Anthropic’s Claude model, including Banner Health, Novo Nordisk, and AbbVie. At the conference, Elation Health announced that it integrated Claude into its EHR to create chart summaries and clinical insights.
Other AI companies at the conference also announced new expansion efforts. For example, Hippocratic AI, which develops patient-facing generative AI healthcare agent, said it acquired Grove AI, a startup that provides agentic AI for pharma research and development and clinical trial operations. According to Hippocratic, the acquisition will help it build its life sciences division and accelerate the use of generative and agentic AI in the biopharma and med tech sectors.
Separately, Open Evidence said it plans to move toward “medical super-intelligence” by building its AI platform on top of a group of specialist medical AI models (oncology, neurology, radiology, etc.) instead of a single centralized model.
Pharma companies discuss new products, drug pricing deals
According to Johnson & Johnson (J&J) CEO Joaquin Duato, 2026 should be a better financial year for the company as it focuses on three high-growth areas for its med tech business: cardiovascular, surgery, and vision. Currently, J&J has around a dozen upcoming product launches across its med tech and innovative medicine businesses, including its new Ottava Robotic Surgical System.
Separately, BioNTech, which is most known for developing a COVID-19 vaccine with Pfizer, is turning its attention to cancer treatment. The company has an $11 billion partnership with Bristol Myers Squibb for its bispecific PDL1-VEGF antibody.
Pharmaceutical leaders also discussed the “most favored nation” (MFN) deals they signed with the Trump administration to reduce the prices of certain prescription drugs.
Paul Hudson, CEO of Sanofi, said that while it may sound like everyone won with these deals, there were compromises from both sides.
“I would say the government got what it needed, and we worked very hard to make sure that we could still deliver what we think is an attractive investment thesis for the company without breaking stride,” Hudson said. “So it was a very difficult needle to thread. I don’t want to give the impression that there’s no impact from MFN, because the question for us is: Can we manage that and deliver an attractive long-range plan?”
Christopher Boerner, CEO of Bristol Myers Squibb, had a similar view. “I think what we did with the agreement we signed at the end of last year is find a way to balance the interest of the administration in ‘most-favored nation’ with, obviously, what’s best for the company, but importantly, how can we find ways to provide real value to patients?”
The digital health market ramps up
In 2025, digital health investments reached $14.2 billion in funding, a 35% increase from 2024 and the highest total since 2022. Last year, there were 26 megadeals, or those that raised over $100 million, and 15 new “unicorn” companies, or those valued at over $1 billion, up from just six in 2024.
Although the digital health market is still below its pandemic-era peak, there was significant growth in the market in 2025, largely driven by excitement around AI, according to analysts from Rock Health. The analysts also noted that there is a growing concentration of power in the digital health space, with certain companies having outsized influence.
“On one side, AI-native upstarts attracted huge rounds at unprecedented speed, a handful of companies broke the IPO drought, and private equity made major moves, signaling real bets on an emerging ‘winner’ class,” wrote Rock Health analysts Megan Zweig, Jacqueline Kimmell, and Maddie Knowles. However, on the other side, “… many companies are still grappling with valuation overhangs from prior cycles while operating in a more competitive market.”
The economic fortunes of mom-and-pop businesses are diverging from those of their larger counterparts — a pre-existing gap that now appears to be getting bigger, faster.
Why it matters:
The evidence is in the private-sector labor market, that in recent months, has been propped up by large companies as smaller firms — typically responsible for 40% of U.S. employment — shed workers.
The big picture:
Larger businesses have been able to adapt to a tough economic backdrop — historic tariffs, high interest rates and a more cautious consumer — in ways far more challenging for small companies with fewer resources.
“It’s evident that medium and large firms are better positioned to weather what’s going on,” said ADP chief economist Nela Richardson.
“They can set prices, they can change suppliers. They can hire contractors instead of permanent employees in a more sophisticated way. They can hire globally, not just in their local region. They have more tools in the toolbox,” Richardson said.
By the numbers:
The hiring gap between small and big businesses is getting worse, a fresh sign that small business firings are holding down jobs growth across the economy.
As we mentioned yesterday, the private sector shed 32,000 jobs in November, according to payroll processor ADP. Small firms — those with fewer than 50 employees — accounted for all of the losses.
Those businesses reported a net loss of 120,000 jobs, the most small businesses have cut since the pandemic’s onset. Larger businesses grew, but not enough to offset the cuts elsewhere.
“Small business hiring reallystarted to slow in April and I attribute some of this to tariffs and the higher cost of doing business that small companies are much less able to absorb,” Peter Boockvar, chief investment officer at One Point BFG Wealth Partners, wrote in a note.
“The natural reaction is to cut costs elsewhere and we know that labor is their biggest cost,” Boockvar added.
The intrigue:
Bloomberg recently reported that there are more small businesses filing for bankruptcy under a special federal program this year than at any point in the program’s six-year history.
Subchapter V filings, which allow firms to shed debt faster and cheaper, are up 8% from last year, according to data from Epiq Bankruptcy Analytics.
Chapter 11 filings — a process used by larger businesses — are up roughly 1% over the same time frame.
Threat level:
Main Street is bearing the brunt of an economic slowdown in ways that might make it even harder for small shops to compete with larger companies.
One bright spot: Despite that pain, applications to start new businesses — ones likely to employ other people — remain notably higher than in pre-pandemic times, according to the latest data available from the Census Bureau.
What to watch:
The Trump administration shrugged off the ADP data that indicated a hiring bust. Commerce Secretary Howard Lutnick told CNBC that the cuts were due to factors unrelated to tariffs, like immigration crackdowns.
That hints at a debate among monetary policymakers, who are trying to gauge how much weak jobs growth is a byproduct of fewer available workers.
But ADP had earlier told reporters that small businesses generally had less demand for workers — not that staff weren’t available for hire.
The software monopoly that powers American hospitals wasn’t built for the data, speed, or intelligence the future of medicine demands.
Epic Systems is an American privately held healthcare software company, founded by Judy Faulkner in 1979, and has grown into the largest electronic health record (EHR) vendor by market share, covering over half of all hospital patients in the U.S.
Epic dominates American healthcare today. But so did Kodak in photography and GE in industry. Its software runs the country’s hospitals, determines the workflows clinicians, nurses and clinical support staff use, and shapes what data gets captured (or more often, what gets lost). It also serves as the front door for healthcare data for the patients it serves. Dominance has never guaranteed a future. Epic’s position reflects the architecture of the past, not the one emerging now.
More importantly, the sheer volume of activity occurring in these hospitals means they are collectively running thousands of experiments, mini clinical trials, and critical observations daily. The stakes are enormous: billions of dollars in drug discovery, the efficiency of clinical trials (currently plagued by poor recruitment and high costs), and the potential for better, personalized care. The data generated in these environments is the single most valuable, untapped resource in all of medicine.
However, this monumental source of value is being throttled by outdated infrastructure, and it shows. It’s hard to imagine a world where AI is used to its full potential in healthcare while Epic is still running the show. The ideas are oppositional at their core.
The Massive Data Problem
Technology is accelerating faster than any legacy system can keep up with. AI is reshaping every major industry, and healthcare will be forced to catch up. However, this essential transformation is structurally incompatible with the dominant system of record.
To put it bluntly: Epic has a data problem. A massive data problem. Not just imperfect data — structurally flawed data. What Epic captures is fragmented, delayed, and riddled with inconsistencies. Diagnoses become billing codes that distort reality. Interventions like intubations, pressor starts, and ventilator changes appear hours late, if at all. Outcomes are incomplete or missing. What remains isn’t a clinical record in any meaningful sense but a billing ledger dressed up as documentation. No model can learn reliably from that.
But the deeper problem is the data Epic never sees. Some of the most valuable information in modern medicine: continuous monitoring streams, ventilator logs, infusion pump data… never enters the EHR in a structured or analyzable form. In many cases, it isn’t captured at all.
I recently brought Roon (a well-known engineer at OpenAI) and Richard Hanania(a public intellectual/cultural critic)—both advisors in my new venture, in full disclosure—to one of the largest academic medical centers in the country. Both watched torrents of millisecond-scale data spill off monitors. Streams that could reveal what’s happening in the brain, heart, and vasculature. Valuable data… all vanished instantly. None of it logged. None of it stored. None of it correlated with outcomes. Roon captured this shock in a viral post on X/Twitter, essentially describing how hospitals are filled with catastrophic events like sudden cardiac death, yet we save none of the time-series data that could teach us how to prevent the next one. His shock distilled what people in technology grasp immediately and what healthcare has normalized: industries where human life isn’t exactly top of mind record everything; hospitals, where the stakes are life and death, learn almost nothing from themselves.
In Silicon Valley, losing data like this is unthinkable. In healthcare, it barely registers.
Epic was never built to ingest or learn from this scale of data. It was built to satisfy billing requirements, regulatory checklists, and documentation workflows. That is the beginning and end of its architecture. It is not a learning system, much less an AI system. It is not even a modern data system. And that is the root of Epic’s downfall.
The Cultural and Financial Moat
Epic is famous for its internal commandments — principles Judy Faulkner wrote decades ago:
Do not acquire.
Do not be acquired.
Do not raise outside capital.
(If you haven’t heard it, the latest Acquired podcast episode on Epic is essential listening)
But the same rules that built its empire now limit what it can become. What was once a strategic strength is now its ceiling.
The next era of healthcare software demands investments that were unnecessary when the EHR was the center of gravity. Building AI-native infrastructure: real-time data pipelines, device integrations, large-scale compute, continuous model training, semantic normalization — requires not millions but tens of billions of dollars. Most companies facing that kind of leap can raise capital, acquire talent, or merge with partners. Epic has ruled all of those options out.
Epic’s formidable market share is anchored by a massive customer sunk cost. With implementation fees often exceeding a billion dollars for large systems, the financial and political inertia makes replacing the EHR functionally unthinkable. However, this commitment only forces customers to defend an obsolete data architecture. By preventing them from adopting novel solutions, this inertia doesn’t protect Epic’s long-term viability, it simply guarantees a widening technical gap between the EHR and the transformative potential of AI.
A company optimized for slow, controlled expansion cannot transform itself into an AI-scale enterprise without violating the principles that define it. The culture that kept Epic dominant is the culture that prevents it from catching the next wave. Epic will continue to excel at documentation, billing, and compliance — but those strengths are anchored in the past. The future belongs to systems that learn, and Epic was never designed to learn.
The Shift to Middleware
Meanwhile, the broader economy is being held up by AI. The world’s largest tech companies are pouring staggering sums into compute, data centers, and model training. And all that compute needs rich, complex, high-value data to train on.
Healthcare is the only remaining frontier of that scale.
No other industry generates so much information while analyzing so little of it. No other sector represents nearly 20% of U.S. GDP yet still runs on fragmented workflows and manual processes. And the incentives here are unmatched: improving patient outcomes, reducing costs, eliminating inefficiency, accelerating drug development, modeling disease trajectories, and eventually automating the more repetitive layers of care. There’s even an irony: the very infrastructure needed to enable learning health systems would also finally make billing more accurate.
I’m not writing this to showcase some utopian vision of AI curing all disease. It’s the practical use of technology we already possess. Our limitation isn’t the models; it’s the missing data.
A handful of companies have bet their trillion-dollar valuations on this: OpenAI, Google, Amazon, Nvidia, Apple, Oracle. They are spending hundreds of billions a year on AI infrastructure and need high-volume, high-quality datasets to justify that investment. Healthcare produces oceans of exactly that kind of data, and most of it evaporates. The companies that learn to capture and structure it will define the next layer of healthcare infrastructure. Whether they integrate with Epic, build around it, or replace it is almost secondary.
What matters is that none of them are waiting for Epic.
Clinicians won’t either. Once tools exist that unify the data hospitals already generate, reduce workload, eliminate administrative drag, and answer the questions clinicians actually ask — What happened? Why did it happen? What should we do now? — the center of gravity will shift. Clinicians will live inside those tools, not inside an interface built for billing.
Epic can still exist, but it doesn’t need to function as healthcare’s operating system. There’s precedent for this in every major industry: the core orchestration/data layer eventually recedes into the background while workflow and data intelligence move up the stack. At that point, the EHR becomes background infrastructure or middleware. The intelligence/workflow layer becomes the real operating system. Epic will undoubtedly resist this shift, yet its attempts to maintain total control of the clinician interface will ultimately collide with the utility and data gravity of AI-native systems.
Epic becomes the backend: essential, invisible, and no longer the place where the practice of medicine occurs.
Regulatory modernization around HIPAA, interoperability, and data liquidity will be essential, but that is a conversation for another essay.
Epic isn’t vanishing tomorrow. Large institutions rarely do. But its relevance is eroding in the only domain that will matter over the next decade: the ability to harness data at a scale and fidelity that makes AI transformative. It can keep its commandments, preserve its culture, and reject outside capital — it just can’t do all that and remain the central platform of hospital data in an AI-native future.
For an economy that’s rapidly expanding, the usual drivers of job creation sure aren’t carrying their weight.
Why it matters:
Anemic job growth in key sectors is a sign that there is more underlying weakness in worker demand than the low unemployment rate might suggest.
It makes for a weaker starting point, as companies see new opportunities around the corner to use AI to automate their work.
It’s not a new trend: These sectors showed weak job creation or outright job losses for the last couple of years of the Biden administration.
But it is striking that a GDP surge fueled by data center and AI investment hasn’t been enough to generate more robust hiring.
By the numbers:
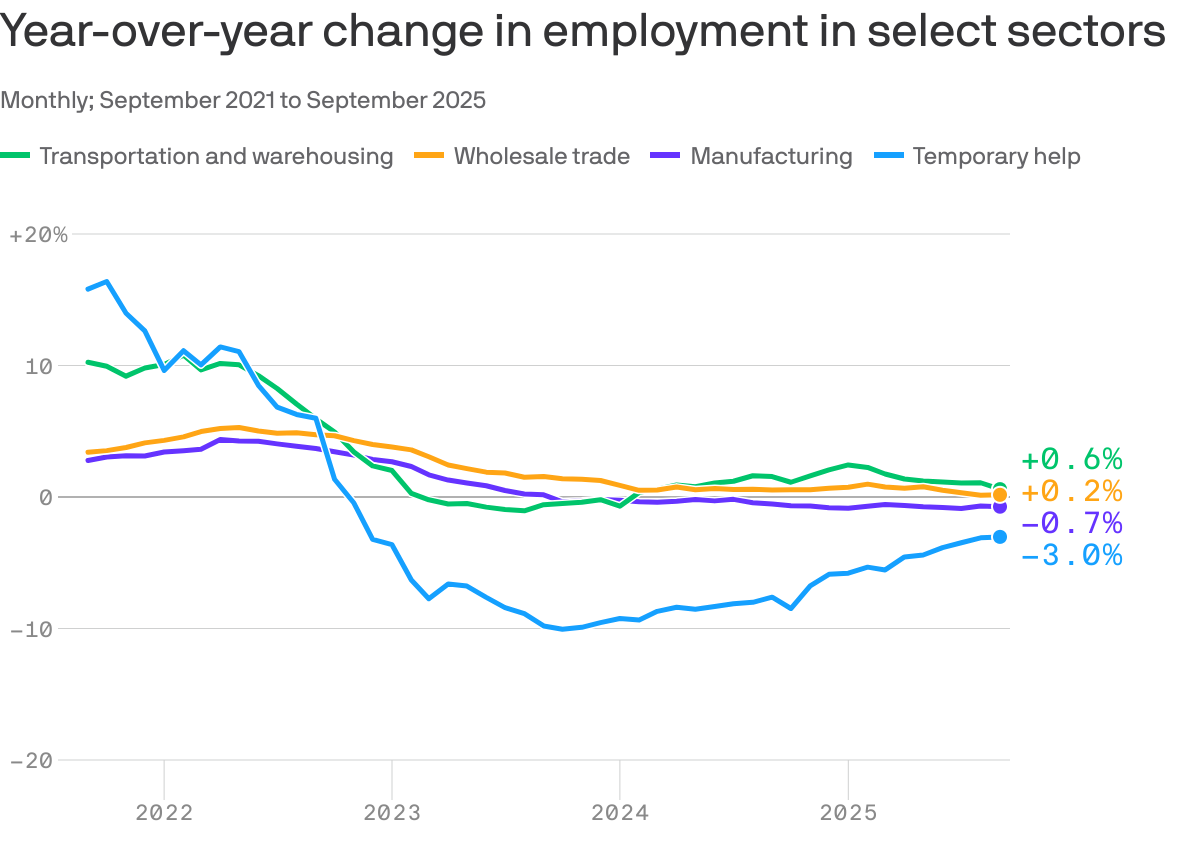
Overall employment is up 0.8% over the 12 months ended in September, but the hiring has been driven in significant part by health care, state and local government, and other less cyclical sectors.
Manufacturing employment is down 0.7% over the last 12 months. Tariffs are weighing on the sector, but its job losses long predate the Trump trade wars, with year-over-year job losses for more than two years.
Temporary help employment, which tends to be a volatile indicator underlying growth trends, is down 3%. It has been losing jobs for three consecutive years.
Two other sectors that tend to correlate with overall economic momentum, transportation and warehousing and wholesale trade, are also adding jobs at rates below that of overall job growth (0.6% and 0.2%, respectively).
Stunning stat:
As Bloomberg flagged, two sectors — health care and social assistance, and leisure and hospitality — accounted for more than 100% of net job gains so far in 2025.
Excluding those sectors, employment dropped by 6,000 jobs in the first nine months of the year.
Zoom out:
There’s not much reason to think these numbers are driven by AI-related opportunities for companies to increase productivity and rely on fewer human workers, particularly given that the phenomenon isn’t new.
But it is more plausible that seeing such opportunities on the horizon has made companies more reluctant to hire in the absence of overwhelming need.
BlackRock chief investment officer for global fixed income Rick Rieder wrote in a note after last week’s jobs report that “what we think we are seeing now is … essentially a hiring pause in anticipation of AI.”
Of note:
A report out this morning from the McKinsey Global Institute finds that AI and robotics technologies could, in theory, automate 57% of U.S. work hours.
“AI will not make most human skills obsolete, but it will change how they are used,” the authors find. “As AI takes on common tasks, people will apply their skills in new contexts,” they write, such as less time researching and preparing documents and more time framing questions and interpreting results.
The bottom line:
Beneath the headline numbers, there is some good reason that attitudes toward the job market are glum.
Layoff trends in 2025 indicate an increase in job cuts compared to 2024, with US employers announcing nearly 950,000 cuts through September, the highest number since 2020. Key drivers include cost-cutting measures, the strategic implementation of artificial intelligence (AI), and a cooling labor market.
Key Trends
Elevated Numbers: Total US job cuts through October 2025 were over one million, a 65% increase from the same period in 2024. October 2025 had the highest number of layoffs for that month in 22 years.
AI as a Primary Driver: AI adoption is a leading cause for job cuts as companies restructure for efficiency and reallocate resources. Companies like Amazon and Intel have cited AI as a reason for significant workforce reductions.
“Forever Layoffs”: A new trend involves smaller, more regular rounds of layoffs (fewer than 50 people) that create ongoing worker anxiety and impact company culture. These rolling cuts often stay out of headlines but contribute significantly to the overall job cuts.
Method of Notification: The process is becoming more impersonal, with many employees being notified of their termination via email or phone call rather than in-person meetings.
Hiring Slowdown: Alongside the layoffs, there has been a sharp drop in hiring plans, with planned hires for the year at their lowest level since 2011.
Affected Industries
While tech has been significantly impacted since late 2022, other industries are also facing substantial cuts in 2025:
Technology: Remains a leading sector for cuts as companies continue to restructure after pandemic-era overhiring and focus on AI.
Retail and Warehousing: Companies like Target and UPS are cutting thousands of jobs due to changing consumer demands, automation, and a push for efficiency.
Energy and Manufacturing: Oil giants such as Chevron and BP are making cuts as part of cost-reduction strategies and market consolidation.
Finance and Consulting: Firms like PwC and Morgan Stanley are trimming staff, citing factors like low attrition rates and the need to realign resources.
Media and Communications: Companies like CNN and the Washington Post have made cuts to pivot toward digital services and reduce costs.
Economic Context
The overall U.S. labor market remains relatively healthy despite the uptick in layoffs, though it is showing signs of cooling. The unemployment rate has inched up, and consumer sentiment has declined. The Federal Reserve is monitoring the situation and has implemented interest rate cuts to help stabilize the job market.