The U.S. recorded 184,514 new COVID-19 infections Nov. 13, a 20 percent increase from the new case count one day prior, according to data compiled by Johns Hopkins University.
The country also hit a 10-day high in daily deaths, with 1,431 reported Nov. 13.
The COVID Tracking Project reported more 68,516 hospitalizations for Nov. 13, with 19 percent of those patients in intensive care units and 6 percent on ventilators.
Here are several other noteworthy developments related to COVID-19 in the U.S. over the past 24 hours:
1. Several governors rolled out measures Nov. 13 to mitigate the virus’s spread, according to the Wall Street Journal.
New Mexico Gov. Michelle Lujan Grisham issued a two-week shutdown of all nonessential activities effective Nov. 16. COVID-19 hospitalizations in the state tripled in the past four weeks.
Oregon Gov. Kate Brown tightened capacity restrictions for restaurants, gyms, retail stores and places of worship, effective Nov. 18.
Virginia Gov. Ralph Northam expanded a mask mandate and restricted public and private gatherings in the state to 25 people, effective Nov. 15. Masks are now required for everyone age 5 and older, rather than age 10 and older.
New York‘s court system issued plans to indefinitely halt most in-person proceedings, including jury duty.
North Dakota Gov. Doug Burgum issued a mask mandate effective Nov. 14 through Dec. 13, as well as capacity limitations for bars, restaurants and event venues.
Vermont Gov. Phil Scott issued an executive order to close bars and clubs and ban multihousehold gatherings of any size, according to The Boston Globe.
2. Massachusetts Gov. Charlie Baker is reopening the state’s field hospital after it went inactive roughly five months ago, according to The Boston Globe. The 240-bed facility at the DCU Center in Worcester should be primed to accept patients the first week of December.
3. The recent widespread surge of COVID-19 cases across most of the U.S. is prompting several states to adjust plans for schooling. Detroit, Boston and Baltimore have shut down or scaled back in-person learning because of increases in coronavirus cases, the Wall Street Journalreports. New York City’s mayor warned parents Nov. 13 that the schools could be closed as soon as Monday if COVID-19 cases continued their climb.
4. Wisconsin’s field hospital, which opened Oct. 14 on the state fairgrounds in West Allis, currently has 15 patientsunder its roof, Wisconsin Public Radio reports. The site could accommodate 50 patients upon opening; as operations ramped up it could take up to 530. WPR reports that the facility is too far for some patients from central and Northern Wisconsin, while others have refused to go to the field hospital even after education about how the alternate care site could free up hospital beds for those who are critically ill.
5. Fewer systems and clinician communities have the option to send help. The geographic distribution of COVID-19 activity means it is less likely that hospitals could deploy a similar strategy to the first and second surges earlier this year, in which medical professionals traveled to reinforce care teams in cities and areas that were in the height of crisis. “We haven’t extended the request, but I’m confident that there’s no one that could come to help,” Jeff Jensen, MD, a critical care physician who splits his time between Mayo Clinic Rochester and Mayo Clinic Health System in La Crosse, Wis., told Bloomberg. “They would be busy taking care of the local issues in their community.”
More people in the US are hospitalized with the coronavirus than at any other time.
More Americans are currently hospitalized with Covid-19 than at any other point in the pandemic, a grim indicator that the third big wave of cases in the US may be the worst wave to date.
On November 11, 65,368 people across the United States were in the hospital after testing positive for the novel coronavirus, according to data reported by the Covid Tracking Project. That’s significantly higher than the last peak of 59,940 recorded on April 15, when the New York City area was the epicenter of the US outbreak. (As the Covid Tracking Project notes, the national and state hospital data have been erratic and incomplete, and reported totals may continue to shift.)
What’s clear from the data is that Covid-19 migrated across the country to new hot spot regions this fall. In the spring, hospitalizations were overwhelmingly concentrated in the Northeast. In the summer, more than half of hospitalized Covid-19 patients were in the South and West: states like Arizona, California, Florida, Georgia, and Texas.
Now the Midwest, Great Plains, and Mountain West are the new hot spots, but some former hot spots are warming back up as well, with cases and hospitalizations surging again. “There’s so many places, with so many people, that the numbers are just drastically higher,” said Daniel McQuillen, an assistant professor of medicine at Tufts and a senior physician in the division of infectious diseases at Beth Israel Lahey Health, at a Wednesday Infectious Diseases Society of America briefing.
As of November 11, Texas had the highest number of hospitalizations of any state (6,779), and Illinois was in second place with 5,042 people in the hospital; other Midwestern states like Michigan, Indiana, and Wisconsin have seen record spikes in cases in recent weeks and now have more than 2,000 people hospitalized each.
“The hospitalization number is the best indicator of where we are,” Eric Topol, a professor of molecular medicine and director of the Scripps Research Translational Institute, told Vox this summer. That’s because it’s a better measurement of the severity of the pandemic than Covid-19 testing, which only finds a fraction of cases and includes more mild cases. “We’re going to go to new heights in the pandemic that we haven’t seen before. Not that what we saw before wasn’t horrifying enough.”
Some states like Utah and North Dakota have lower total hospitalizations but also fewer hospitals and hospital beds — and they’re now reaching a woeful tipping point of hospitals stretched to maximum capacity.
“Here in Salt Lake City, we provide a lot of [specialized infectious disease and ICU care] to people in four states as far away as Montana, Arizona, and Wyoming … and our hospitals and caregivers are extraordinarily stressed,” Andrew Pavia, the chief of pediatric infectious diseases at the University of Utah School of Medicine, said at the IDSA briefing. “Our ICUs are full, but that includes overflow ICUs that have been purpose-built, taking advantage of the time we’ve had to plan.”
This was, unfortunately, to be expected (although it wasn’t inevitable). As the weather has turned cooler and states failed to fully control their outbreaks, transmission picked up when people moved indoors. Nearly all the states currently experiencing an increase in new cases and hospitalizations also did not experience major outbreaks in the spring or summer, so residents were less fearful and took less action to prevent the spread of the virus.
“There was a political climate where there’s distrust of government and reluctance to take harsh measures,” in places like Utah, said Pavia. “Many of these states did not have mask mandates until very recently, and some don’t even have them today and have very limited restrictions on mass gatherings.”
Deaths are ticking up again too, reaching 1,592 on November 11, reversing a steady decline that had begun in early May after the first wave and in August after the second wave.
Cumulatively, 10.2 million Americans have tested positive for Covid-19 since the pandemic began, and more than 233,000 of them have died. With hospitalizations surging and several states reporting thousands of new cases a day, experts say we are in for a difficult late fall and winter.
The new hospitalizations, and the untenable pressure they’re putting on the health care system, are also a reminder of how critical it is for states to implement and enforce measures like mandatory face masks, restrictions on bars and restaurants, and for the federal government to fix testing and contact tracing problems. “It should be an all-points bulletin to really bear down on this, because otherwise there’s no limit on where this might go,” said Topol.
Hospitals are running out of staff and beds for Covid-19 patients
The good news is that infectious disease experts think many hospitals are better prepared to handle surges in Covid-19 patients than they were in the spring. For the most part, they have the equipment they need and they know how to deploy it. They also have more standardized protocol for treating the sickest patients.
Yet hospitals in hot spots across the country are maxing out their staff, equipment, and beds, with doctors and nurses warning that the worst-case scenario of hospital resources being overwhelmed is on the horizon if their states don’t get better control of the coronavirus.
“The surge of Covid-19 patients takes away from our ability to care for the sick patients that are already in Arkansas,” said a nurse at a major health system in Little Rock, who asked to go unnamed fearing retaliation from her employer. “We have so many nurses quarantined that we’re not able to staff our oncology unit appropriately, and our patients are being negatively affected. Covid-19 is right now overburdening our healthcare system in Arkansas.”
Hospitals in several states are also straining to find enough specialists to treat the very sick Covid-19 patients. “ICU beds don’t take care of people — you need staff,” said Pavia of the University of Utah School of Medicine. “And one of the things that many of the Western states have in common is a relative shortage of the people we need to take care of very sick people during a pandemic like this: ICU doctors, probably most importantly ICU nurses, and infectious disease physicians, respiratory therapists. These folks have been working flat out for eight or nine months, and three months into the surge, they’re exhausted, they’re stressed.”
Staffing is a universal problem in hot spots. Gov. Gary Herbert of Utah said the state will have to bring in out-of-state nurses to help with the surge, and officials and health care providers in South Dakota, Tennessee, Arizona, and Wisconsin are requesting them too:v
In Texas, officials are setting up medical tents in El Paso and Lubbock in response to the rapid rise in hospitalized Covid-19 patients and a dwindling number of hospital beds. “El Paso, Texas, is almost completely out of ICU beds; Lubbock, the same thing,” said McQuillen.
“We are the 11th-largest city in the state of Texas and we have two field hospitals on their way to town,” Jarrett Atkinson, Lubbock’s city manager, told KCBD on Tuesday. “I can absolutely assure you that never in my career did I think we would be deploying field hospitals to Lubbock, Texas.”
According to McQuillen, both El Paso and Lubbock have been “much less stringent with their populations [mandating] simple things like wearing masks, and socially distancing.” He compared that to Massachusetts and other Northeast states where he says strict measures during the spring surge made a big difference in reversing the steep climb in cases and hospitalizations. Yet too many states ignored that critical lesson, and now are paying the price.
Daily deaths are creeping up again but are still far below the earlier peak
While daily Covid-19 hospitalizations are surging, another key metric, daily deaths, reached 1,562 on November 11, the highest it has been since May during the first surge, according to the Covid Tracking Project. It’s an ominous sign that deaths could reach unprecedented levels in the coming weeks and months, given that cases and hospitalizations are now at new highs.
It’s possible, experts say, that fewer people who are hospitalized will end up dying in this winter stage of the pandemic as compared to the spring. As Vox’s Julia Belluz reported, there have been significant improvements in mortality in the US and Europe in the past several months, as doctors’ understanding of Covid-19 and how to treat it has improved:
Though there’s still a lot of progress to be made, the treatment approach has become more standardized over time, said Jen Manne-Goehler, an infectious disease doctor at Brigham and Women’s and Massachusetts General hospitals. When she started treating Covid-19 patients in the spring, it felt like practice was changing every few days. Now it’s more streamlined — and that’s undoubtedly helping with survival, too.
That said, if hospitals in the hard-hit states run out of beds and staff to treat the incoming flow of patients, more people who could have been saved may die. When ICU staff were stretched in the spring, “ICU patients just didn’t get the same attention,” intensive care doctor Lakshman Swamy, who works with the Cambridge Health Alliance, told Belluz.
Official Covid-19 cases and hospitalizations in the United States are piling up at record rates — and daily deaths, experts fear, may soon follow.The following charts show how the fall coronavirus wave has put the US on unprecedented ground by some metrics, and with numbers trending up, point to how the situation could get worse while the country awaits a vaccine and distribution of new treatments.
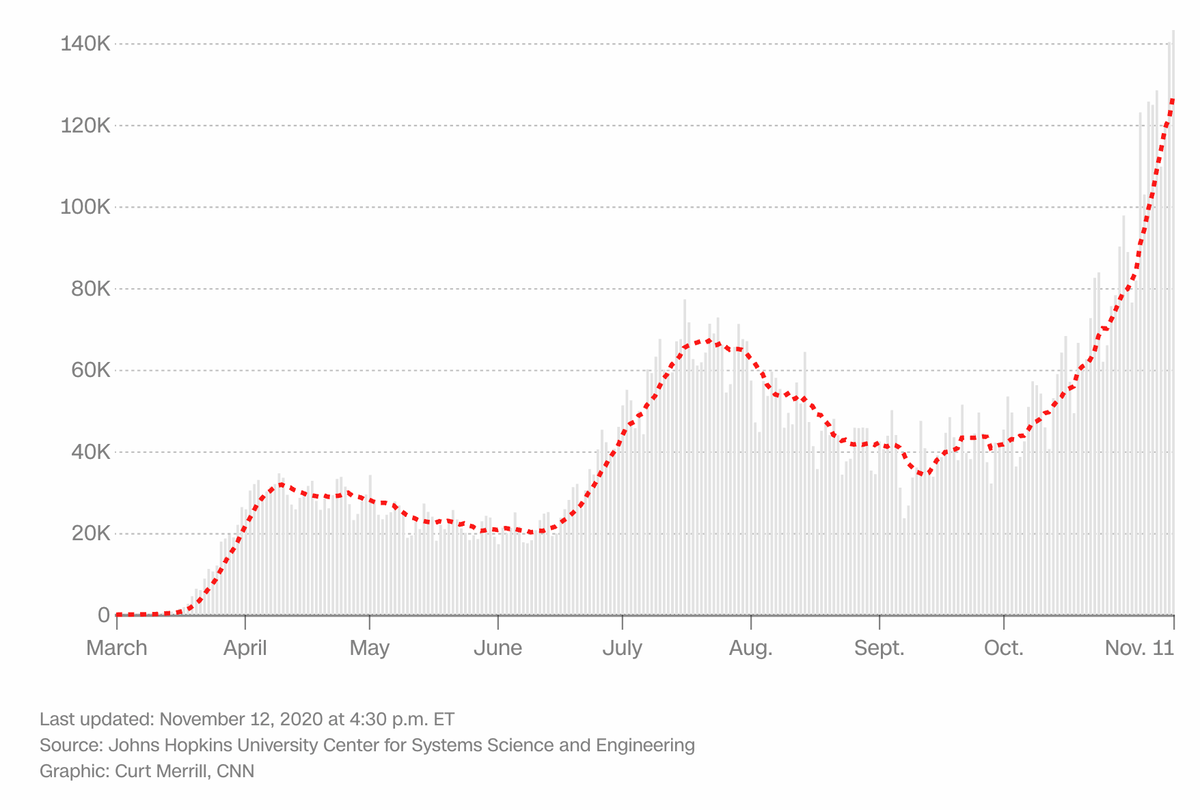
Daily case counts are reaching new highs
Daily cases were dipping as recently as September, as the nation was bouncing back from a summer surge.But infections roared back in a way not recorded before.Thursday brought the United States’ highest one-day infection total (above 153,000) and seven-day average for new daily infections (more than 131,000) on record, according to Johns Hopkins University data.
That average is more than 3.5 times higher than it was on September 12, when it was at a post-summer surge low of 34,198.And it’s well above the summer’s highest seven-day average, which was around 67,100 on July 22.
There has been good news recently: A vaccine candidate was reportedly found to be more than 90% effective, and the US Health and Human Services secretary said vaccines could be widely available in the second quarter of 2021. And the Food and Drug Administration this week approved a new antibody treatment that may lower the risk that patients with mild to moderate disease will be hospitalized.But with colder weather potentially driving risky gatherings indoors, and no vaccine available this minute, experts warn daily infections have room to grow.“It will not surprise me if in the next weeks we see over 200,000 new cases a day,” Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, told CNN on Monday.We should stress that the chart captures reported cases. Studies have estimated infections were vastly undercounted, especially early in the pandemic, partly because of limited test availability.Some health experts have said hospitalizations can be a truer measure of the pandemic’s severity — though rising cases are a warning sign, since a patient’s hospitalization can come well after diagnosis.
‘Most sensitive indicator’ of infections is up
US test positivity rates are rising
A test positivity rate is the percentage of people who get tested and turn out to be infected. And the US rate has been shooting up in recent weeks.The country’s test positivity rate averaged 8.7% over seven days as of early Thursday, according to the COVID Tracking Project.That’s above a summer’s highest seven-day average of about 7.9% in mid-July.The World Health Organization in May advised governments not to reopen until test positivity rates were 5% or lower for at least 14 days.And the director of the US Centers for Disease Control and Prevention, Dr. Robert Redfield, has suggested that communities’ positivity rates should be below 5% to comfortably have schools open.
White House coronavirus task force coordinator Dr. Deborah Birx has said test positivity rate is the statistic she watches the closest, because it is “the most sensitive indicator” of how the coronavirus situation is unfolding at any particular time and place.
Hospitals have more Covid patients than ever
More Covid-19 patients are reported to be in US hospitals now than at any previous point in the pandemic. About 65,300 coronavirus patients were in those facilities Wednesday, according to the COVID Tracking Project.That’s more than double the number from September 20, when the country was at post-summer-surge low of 28,608.And it’s beyond the summer peak of 59,718 on July 23, and the spring peak of 59,940 on April 15.”The new hospitalization record underscores that we’ve entered the worst period for the pandemic since the original outbreak in the Northeast,” two COVID Tracking Project co-founders wrote in an online post Wednesday.These hospitalization numbers prove that the current surge of Covid-19 cases is not merely the result of increased screening of asymptomatic people. Rather, the cases we’re detecting are a leading indicator that many people are seriously ill,” the post reads.Some hospital systems have said in recent days they are close to being overwhelmed.Seventeen states reported records for Covid-19 hospitalizations on Tuesday: Alaska, Arkansas, Colorado, Indiana, Iowa, Kentucky, Minnesota, Missouri, Montana, Nebraska, Ohio, Oklahoma, Oregon, South Dakota, Tennessee, Wisconsin and Wyoming, the tracking project said.The hospitalization numbers likely have become more accurate over time — Florida didn’t report its hospitalizations until July 10, the COVID Tracking Project notes.
The toll of lives lost is climbing, too
The country’s recent daily Covid-19 death tallies aren’t in record territory, but they are shooting upward.The average number of deaths per day, across a week, rose above 1,000 this week for the first time since the summer.That average was 1,034 on Wednesday — the highest since August 10, Johns Hopkins data shows. More than 1,380 deaths were reported on Wednesday alone.The University of Washington’s Institute for Health Metrics and Evaluation projects the US could average more than 1,650 deaths per day by December 1, and more than 2,200 daily by January 1, if government leaders kept current social distancing mandates and even added some.That would recall the tallies seen early in the pandemic, when 2,000+ deaths were reported daily for a time in April. The highest daily average across a week was 2,241, on April 24.Infections appear to be killing fewer people on average now than early in the pandemic, in part, experts say, because of changes in the way the disease is treated and a rise in the proportion of younger people becoming infected.But as hospitalizations break records, daily death rates could climb further.”The ratio of hospitalizations to deaths has fallen tremendously since the spring,” the COVID Tracking Project’s post from Wednesday reads. “But it is also true that wherever we see hospitalizations go up, deaths rise two to three weeks later.”
Hospitalized COVID-19 patients receiving SNG001, inhaled nebulized interferon beta-1a, were more likely to show clinical improvement than those receiving placebo, a small pilot study in the U.K. found.
Patients randomized to receive SNG001 for 14 days had greater odds of improvement on the World Health Organization (WHO) ordinal scale for clinical improvement (OSCI; OR 2.32, 95% CI 1.07-5.04, P=0.033) on day 15 or 16 compared with those receiving placebo, reported Tom Wilkinson, PhD, of University of Southampton in England, and colleagues.
Moreover, patients in the intervention group were more likely to revert to an OSCI score of 1, or no limitation of activities, on day 15 or 16 (HR 2.19, 95% CI 1.03-4.69, P=0.043), the authors wrote in the Lancet Respiratory Medicine.
Type 1 interferon is “one of the first cytokines induced by viral infection of a cell and is a primary driver of innate immune responses in the human lung,” the researchers noted. They explained that SNG001 is a formulation of recombinant interferon beta “for inhaled delivery by [nebulizer],” which has been well tolerated in clinical studies among patients with asthma or chronic obstructive pulmonary disease.
In addition to different composition of the two trials, the editorialists found another key difference: route of administration. SOLIDARITY used subcutaneous interferon beta-1a, whereas this trial used nebulized therapy that “delivers interferon beta-1a directly to the respiratory tract.”
“[Nebulized] therapy allows targeted delivery of interferon to the lungs, where it can induce the expression of interferon-stimulated genes that participate directly … or indirectly … in the antiviral response in the mucosa,” Peiffer-Smadja and Yazdanpanah wrote.
For the new study, Wilkinson and colleagues randomized adults hospitalized with COVID-19 symptoms, who tested positive for SARS-CoV-2 via reverse-transcriptase polymerase chain reaction or point-of-care test to receive either SNG001 or inhaled placebo for 14 days. Primary outcome was change in clinical condition on the WHO OSCI (a 9-point scale where 0 means no infection and 8 means death).
From March 30 to May 30, a total of 48 patients were randomized to SNG001 and 50 to placebo in an intent-to-treat analysis. Patients were a mean age of 57, 59% were men, and 80% were white. Baseline comorbidities included hypertension, cardiovascular disease, diabetes, chronic lung condition, and cancer.
Demographic characteristics between groups were similar, although the SNG001 group had more severe disease, with 77% of patients receiving oxygen therapy vs 58% in the placebo group. Mean duration of symptoms before treatment initiation was 10 days.
In the SNG001 group, the odds of improvement were more than three-fold greater on day 28 versus placebo (OR 3.15, 95% CI 1.39-7.14, P=0.046), the authors noted.
Five patients underwent intubation or died compared with three in the intervention group. Over the 14 days of treatment, patients in the intervention group were more than twice as likely to recover.
There was no difference in the odds of hospital discharge or time to hospital discharge between groups. By day 14, 73% of the placebo group and 69% of the intervention group had been discharged.
Regarding safety, 54% of patients in the intervention group and 60% in the placebo group reported treatment-emergent adverse events, the most common of which was headache (15% and 10%, respectively). Fewer patients in the intervention group had serious adverse events compared with placebo (15% vs 28%), and the most common were respiratory failure (6% vs 12%) and pneumonia (6% each).
One patient in the placebo group had multiple organ dysfunction syndrome and one had pulmonary embolism, which caused them to withdraw from the study. These patients later died, along with a third patient in the placebo group, who died of COVID-19 pneumonia.
In their editorial, Peiffer-Smadja and Yazdanpanah noted that the study was not powered to assess mortality outcomes, and called for large randomized trials to investigate the effectiveness of nebulized interferon beta-1a, speculating that it might benefit patients in an early stage of disease in the outpatient setting.
“In patients with severe COVID-19, an exacerbated inflammatory response has been identified as a cause of pulmonary complications, and interferon beta-1a — a pro-inflammatory cytokine — could increase the inflammatory response and be associated with safety issues,” the editorialists wrote.
They added that safety will also be a concern, as “[nebulization] of interferon has no marketing [authorization] for any indication yet.”
Dr. Megan Ranney has learned a lot about Covid-19 since she began treating patients with the disease in the emergency department in February.
But there’s one question she still can’t answer: What makes some patients so much sicker than others?
Advancing age and underlying medical problems explain only part of the phenomenon, said Ranney, who has seen patients of similar age, background and health status follow wildly different trajectories.
“Why does one 40-year-old get really sick and another one not even need to be admitted?” asked Ranney, an associate professor of emergency medicine at Brown University.
In some cases, provocative new research shows, some people — men in particular — succumb because their immune systems are hit by friendly fire. Researchers hope the finding will help them develop targeted therapies for those patients.
In an international study in Science, 10 percent of nearly 1,000 Covid-19 patients who developed life-threatening pneumonia had antibodies that disable key immune system proteins called interferons. These antibodies — known as autoantibodies, because they attack the body itself — weren’t found at all in 663 people with mild or asymptomatic Covid-19 infections. Only four of 1,227 healthy patients had the autoantibodies. The study was led by the Covid Human Genetic Effort, which includes 200 research centers in 40 countries.
“This is one of the most important things we’ve learned about the immune system since the start of the pandemic,” said Dr. Eric Topol, executive vice president for research at Scripps Research in San Diego, who wasn’t involved in the new study. “This is a breakthrough finding.”
In a second Science study by the same team, the authors found that an additional 3.5 percent of critically ill patients had mutations in genes that control the interferons involved in fighting viruses. Given that the body has 500 to 600 of those genes, it’s possible that researchers will find more mutations, said Qian Zhang, lead author of the second study.
Interferons serve as the body’s first line of defense against infection, sounding the alarm and activating an army of virus-fighting genes, said virologist Angela Rasmussen, an associate research scientist at the Center for Infection and Immunity at Columbia University’s Mailman School of Public Health.
“Interferons are like a fire alarm and a sprinkler system all in one,” said Rasmussen, who wasn’t involved in the new studies.
Lab studies show that interferons are suppressed in some people with Covid-19, perhaps by the virus itself.
Interferons are particularly important for protecting the body against new viruses, such as the coronavirus, which the body has never encountered, said Zhang, a researcher at Rockefeller University’s St. Giles Laboratory of Human Genetics of Infectious Diseases.
When infected with the novel coronavirus, “your body should have alarms ringing everywhere,” Zhang said. “If you don’t get the alarm out, you could have viruses everywhere in large numbers.”
Significantly, patients didn’t make autoantibodies in response to the virus. Instead, they appeared to have had them before the pandemic even began, said Paul Bastard, the antibody study’s lead author, who is also a researcher at Rockefeller University.
For reasons that researchers don’t understand, the autoantibodies never caused a problem until patients were infected with Covid-19, Bastard said. Somehow, the coronavirus, or the immune response it triggered, appears to have set them in motion.
“Before Covid, their condition was silent,” Bastard said. “Most of them hadn’t gotten sick before.”
Bastard said he now wonders whether autoantibodies against interferon also increase the risk from other viruses, such as influenza. Among patients in his study, “some of them had gotten flu in the past, and we’re looking to see if the autoantibodies could have had an effect on flu.”
Scientists have long known that viruses and the immune system compete in a sort of arms race, with viruses evolving ways to evade the immune system and even suppress its response, said Sabra Klein, a professor of molecular microbiology and immunology at the Johns Hopkins Bloomberg School of Public Health.
Antibodies are usually the heroes of the immune system, defending the body against viruses and other threats. But sometimes, in a phenomenon known as autoimmune disease, the immune system appears confused and creates autoantibodies. This occurs in diseases such as rheumatoid arthritis, when antibodies attack the joints, and Type 1 diabetes, in which the immune system attacks insulin-producing cells in the pancreas.
Although doctors don’t know the exact causes of autoimmune disease, they’ve observed that the conditions often occur after viral infections. Autoimmune diseases are more common as people age.
In yet another unexpected finding, 94 percent of patients in the study with the autoantibodies were men. About 12.5 percent of men with life-threatening Covid-19 pneumonia had autoantibodies against interferon, compared with 2.6 percent of women.
That was unexpected, given that autoimmune disease is far more common in women, Klein said.
“I’ve been studying sex differences in viral infections for 22 years, and I don’t think anybody who studies autoantibodies thought this would be a risk factor for Covid-19,” Klein said.
The study might help explain why men are more likely than women to become critically ill with Covid-19 and die, Klein said.
“You see significantly more men dying in their 30s, not just in their 80s,” she said.
Akiko Iwasaki, a professor of immunobiology at the Yale School of Medicine, noted that several genes involved in the immune system’s response to viruses are on the X chromosome.
Women have two copies of this chromosome — along with two copies of each gene. That gives women a backup in case one copy of a gene becomes defective, Iwasaki said.
Men, however, have only one copy of the X chromosome. So if there is a defect or a harmful gene on the X chromosome, they have no other copy of the gene to correct the problem, Iwasaki said.
Bastard noted that one woman in the study who developed autoantibodies has a rare genetic condition in which she has only one X chromosome.
Women more likely to be ‘long-haulers’
Scientists have struggled to explain why men have a higher risk of hospitalization and death from Covid-19. When the disease first appeared in China, experts speculated that men suffered more from the virus because they are much more likely to smoke than Chinese women.
Researchers quickly noticed that men in Spain were also more likely to die of Covid-19, however, even though men and women there smoke at about the same rate, Klein said.
Experts have hypothesized that men might be put at higher risk by being less likely to wear masks in public than women and more likely to delay seeking medical care, Klein said.
But behavioral differences between men and women provide only part of the answer. Scientists say it’s possible that the hormone estrogen may somehow protect women, while testosterone may put men at greater risk. Interestingly, recent studies have found that obesity poses a much greater risk to men with Covid-19 than to women, Klein said.
Yet women have their own form of suffering from Covid-19.
Studies show that women are four times more likely to experience long-term Covid-19 symptoms, lasting weeks or months, including fatigue, weakness and a kind of mental confusion known as “brain fog,” Klein said.
As women, “maybe we survive it and are less likely to die, but then we have all these long-term complications,” she said.
After reading the studies, Klein said she would like to learn whether patients who become severely ill from other viruses, such as influenza, also harbor genes or antibodies that disable interferon.
“There’s no evidence for this in flu,” Klein said. “But we haven’t looked. Through Covid-19, we may have uncovered a very novel mechanism of disease, which we could find is present in a number of diseases.”
To be sure, scientists say the new study solves only part of the mystery of why patient outcomes can vary so greatly.
Researchers say it’s possible that some patients are protected by previous exposure to other coronaviruses. Patients who get very sick also may have inhaled higher doses of the virus, such as from repeated exposure to infected co-workers.
Although doctors have looked for links between disease outcomes and blood type, studies have produced conflicting results.
Screening patients for autoantibodies against interferons could help predict which patients are more likely to become very sick, said Bastard, who is also affiliated with the Necker Hospital for Sick Children in Paris. Testing takes about two days. Hospitals in Paris can now screen patients on request from a doctor, he said.
Although only 10 percent of patients with life-threatening Covid-19 have autoantibodies, “I think we should give the test to everyone who is admitted,” Bastard said. Otherwise, “we wouldn’t know who is at risk for a severe form of the disease.”
Bastard said he hopes his findings will lead to new therapies that save lives. He noted that the body manufactures many types of interferons. Giving patients a different type of interferon — one not disabled by their genes or autoantibodies — might help them fight off the virus.
In fact, a pilot study of 98 patients published Thursday in the Lancet Respiratory Medicine journal found benefits from an inhaled form of interferon. In the industry-funded British study, hospitalized Covid-19 patients randomly assigned to receive interferon beta-1a were more than twice as likely as others to recover enough to resume their regular activities.
Researchers need to confirm the findings in a much larger study, said Dr. Nathan Peiffer-Smadja, a researcher at Imperial College London who wasn’t involved in the study but wrote an accompanying editorial. Future studies should test patients’ blood for genetic mutations and autoantibodies against interferon to see whether they respond differently from others.
Peiffer-Smadja said inhaled interferon may work better than an injected form of the drug because it’s delivered directly to the lungs. While injected versions of interferon have been used for years to treat other diseases, the inhaled version is still experimental and not commercially available.
And doctors should be cautious about interferon for now, because a study led by the World Health Organization found no benefit to an injected form of the drug in Covid-19 patients, Peiffer-Smadja said. In fact, there was a trend toward higher mortality rates in patients given interferon, although the finding could have been due to chance. Giving interferon later in the course of disease could encourage a destructive immune overreaction called a cytokine storm, in which the immune system does more damage than the virus.
Around the world, scientists have launched more than 100 clinical trials of interferons, according to clinicaltrials.gov, a database of research studies from the National Institutes of Health.
Until larger studies are completed, doctors say, Bastard’s findings are unlikely to change how they treat Covid-19.
Dr. Lewis Kaplan, president of the Society of Critical Care Medicine, said he treats patients according to their symptoms, not their risk factors.
“If you are a little sick, you get treated with a little bit of care,” Kaplan said. “You are really sick, you get a lot of care. But if a Covid patient comes in with hypertension, diabetes and obesity, we don’t say: ‘They have risk factors. Let’s put them in the ICU.'”
Public health experts are sounding the alarm about the trajectory of the pandemic in the United States as the coronavirus spreads through the country largely unabated and officials muse aloud about the possibility of fresh lockdowns.
The experts use different language to underscore the situation’s urgency: Former Centers for Disease Control and Prevention director Tom Frieden said the nation is experiencing a “dangerous time.” CNN chief medical correspondent Sanjay Gupta called the crisis a “humanitarian disaster.” Epidemiologist Michael Osterholm, who was recently named to President-elect Joe Biden’s coronavirus task force, described the situation bluntly as “covid-hell.”
Their warnings come amid widespread fatigue with restrictions, even as the virus is nowhere near finished rampaging across the country. Although several states implemented new mitigation measures this week, many people have been letting down their guards or, in some cases, vowing outright to ignore the rules.
Fourteen states, mostly in the Midwest, had reported record numbers of hospitalizations by midday Thursday as the seven-day average number of cases reached highs in 23 states, from Nevada to Maryland, according to data tracked by The Washington Post. Hospital officials predicted that they could soon face excruciating decisions about how to prioritize care as they run short on beds and staff.
“Our hospitals are full,” Megan Ranney, an emergency medicine professor at Brown University, said in an interview. “Our workers are getting sick. And it is simply overwhelming the system.”
The rapid rise in hospitalizations could foreshadow a long period of rising deaths,said Scott Gottlieb, former director of the Food and Drug Administration. Although improvements in care have pushed the mortality rate below 1 percent in the United States, 1,549 people died of the virus Wednesday, the highest toll since April.
The distribution of hospitalizations across the country means it will be hard for health-care workers from one region of the country to serve as backup in another area, Gottlieb wrote on Twitter. The only slightly reassuring news is that most hospitals have not entered true crisis mode, he said Thursday on CNBC’s “Squawk Box.”
“Every hospital system is a little pressed right now,” Gottlieb said. “There’s only a handful that are really overwhelmed: Wisconsin, parts of Texas, Utah, South and North Dakota.”
But the trends suggest that that could change. Osterholm said ballooning numbers of infections nationwide mean more hospitals could soon look like those in El Paso, where health-care workers are bringing in mobile morgues and airlifting patients to other cities.
“We have to tell the story of what’s coming; people don’t want to hear that El Paso isn’t an isolated event,” he told Yahoo Finance on Thursday. “It will become the norm.”
Frieden tweeted that the United States has entered “the exponential phase” of virus spread and that the situation will worsen significantly before it improves. But he emphasized that policy decisions have an impact, and throwing in the towel is the wrong solution.
“Not all of the US is experiencing the same rate of Covid spread — some states are doing much better than others,” he wrote. “For example, South Dakota (the state with the highest rate) has 100 times more spread than Vermont right now.”
Individual decisions also make a difference, Gottlieb said, especially as people prepare to travel and visit people outside their household for Thanksgiving. The transmission of the virus tracks closely with people’s movement in their communities.
“If people on the whole just go to the store one less time a week, you could substantially reduce spread,” Gottlieb said on “Squawk Box.”
The lack of that kind of self-sacrifice is one factor that Ranney said she believes is contributing to the virus surging to a far greater extent than it did in the spring. New rules from local and state governments, such as curfews, have been relatively mild compared to the widespread shutdowns of March and April.
The holiday season, meanwhile, is a looming danger that Ranney expects will lead to a “deadly” spike in infections. The virus’s prevalence across the country means that this is the worst time for people to increase their risk of transmission by attending family-centric celebrations, she said.
The likelihood that there will be an easily available vaccine next year is the light at the end of the tunnel. But in the meantime, Ranney said people need to fight the urge to pretend that life is normal and instead seek ways to socialize more safely — outdoors, at a distance and while wearing masks.
“A vaccine is coming. This is not forever,” she said. “But right now, we’ve got to stop this chain of transmission.”




:format(webp):no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/22032257/third_wave_hosp_covid_chart_nov11.jpg)
:format(webp):no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/22030735/GettyImages_1229570053t.jpg)
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/22030756/GettyImages_1216851013t.jpg)
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/22030769/GettyImages_1264685606t.jpg)