In 2020, a record-breaking 19 rural hospitals closed their doors due to a combination of worsening economic conditions, changing payer mix, and declining patient volumes. But many more are looking to affiliate with larger health systems to remain open and maintain access to care in their communities. The graphic above illustrates how rural hospital affiliations (including acquisitions and other contractual partnerships) have increased over time, and the resulting effects of partnerships.
Affiliation rose nearly 20 percent from 2007 to 2016; today nearly half of rural hospitals are affiliated with a larger health system.
Economic stability is a primary benefit: the average rural hospital becomes profitable post-affiliation, boosting its operating margin roughly three percent in five years. But despite improved margins, many affiliated rural hospitals cut some services, often low-volume obstetrics programs, in the years following affiliation.
Overall, the relationship likely improves quality: a recent JAMA study found that rural hospital mergers are linked to better patient mortality outcomes for certain conditions, like acute myocardial infarction. Still, the ongoing tide of rural hospital closures is concerning, leaving many rural consumers without adequate access to care. Late last month, the Department of Health and Human Services announced it would distribute another $7.5B in American Rescue Plan Act funds to rural providers.
While this cash infusion may forestall some closures, longer-term economic pressures, combined with changing consumer demands, will likely push a growing number of rural hospitals to seek closer ties with larger health systems.
Unemployment claims jumped last week, as the delta variant of the coronavirus sparked rising caseloads around the country and renewed fears about the potential for more restrictions and business closures.
The number of new claims grew to 419,000 from 368,000, the third time in six weeks that they had ticked up, according to data from the Department of Labor.
Economists said the uptick was concerning but cautioned that it was too early to tell whether it was a one week aberration or telegraphed a more concerning turn for the labor market.
“The unexpected bump in claims could be noise in the system, but it’s also not hard to see how the rise of the covid-19 delta variant could add thousands of layoffs to numbers that already are double what they were pre-Covid,” said Robert Frick, corporate economist at Navy Federal Credit Union.
Overall, unemployment numbers have been falling gradually from the peaks at other stages of the pandemic, but they are still well above pre-pandemic averages.
The jobless numbers have provided a jarring catalogue about the economic devastation wrought by the pandemic — spiking to records as the pandemic unfolded in March 2020, and remaining at historic high levels throughout most of 2020.
The coronavirus surge last fall helped precipitate a rise in claims that saw the labor market, as seen in the monthly jobs report, slide backward too.
But until recently, the last few months been marked by strong jobs growth and a sense of optimism as vaccinations picked up, giving economists hope that the country was back on track to recovering the nearly 7 million jobs it is still down from before the pandemic.
Now, the delta variant is driving an alarming increase in covid-19 cases around the country, according to public health officials: the number of new cases increased more than 40 percent in the last week, sending jitters through the stock market, and is raising questions about whether state and local health authorities will reinstitute restrictions to slow the virus’ spread.
Frick said that the report showed the potential for unemployment claims to start trending upward after months of steady declines.
“There’s definitely a correlation, however loose, that the rise in covid does cause a rise in claims,” he said. “My fear is that the rise in the delta variant could cause claims to go back up…Certainly one week doesn’t show that. But I wouldn’t be surprised if we start to see claims rise.”
However, there are also lots of signs that the economy continues to rebound despite rising caseloads.
The more than 2.2 million people that the Transportation Security Administration said it screened at airports on Sunday was the most since late February 2020 — and nearly three times the amount it was on the same day last year.
Restaurant dining has largely rebounded in recent months, at times surpassing the levels from before the pandemic — on Saturday the number of diners was 1 percent higher than the same day in 2019, according to data from Open Table.
Last week, some 12.5 million claims were filed for unemployment insurance overall, according to the most recent numbers — down from 32.9 million filed at the same point last year.
Nevada, Rhode Island and California topped the list of states with the highest number of people on unemployment, the Labor Department said.
Economic concerns in recent months have been more focused on the ways that workers are still held back from filling some of the more than 9 million job openings in the country, than unemployment, with high hopes that school re-openings in the fall will help many parents get back into the labor force.
“For the most part providers were dependent on that CARES funding. I think they would have been in the red or break even without it,” Suzie Desai, a senior director at S&P Global Ratings, said.
The pandemic weighed heavily on the financial performance of not-for-profit hospitals in 2020, but some of the larger health systems remained profitable despite the upheaval — in large part thanks to substantial federal funding earmarked to prop up providers during the global health crisis.
Industry observers have been closely watching to see how health systems ultimately fared in 2020. Now, with the fiscal-year ended and accounted for, analysts say the $175 billion in federal funds was crucial for providers’ bottom lines.
“Without the stimulus funding, it is very likely we would have seen more issuers [hospitals/health] systems experience either lower profitable margins, or outright losses from operations,” Kevin Holloran, senior director of U.S. public finance for Fitch Ratings, said.
Still, the pandemic put a squeeze on nonprofit hospital margins last year, according to a recent Moody’s report that showed the median operating margin was 0.5% in 2020 compared to 2.4% in 2019.
The first half of the year hit providers especially hard as volumes fell drastically, seemingly overnight. Revenue plummeted alongside the volume declines as the nation paused lucrative elective procedures to preserve medical resources.
One estimate showed hospitals lost more than $20 billion as they halted surgeries in the early months of the outbreak in the U.S.
But as the year wore on, the outlook improved as some volumes returned closer to pre-pandemic levels. At the same time, health systems worked to cut expenses to mitigate the financial strain.
Still, some health systems did post operational losses even with the federal funds meant to help them. Moody’s found that 42% of 130 hospitals surveyed posted an operating loss, an increase from 23% the year prior. Yet, the 2019 survey included more hospitals, a total of 282.
Sutter Health, the Northern California giant, reported an operating loss for 2020 and said it was launching a “sweeping review” of its finances as the pandemic exacerbated existing challenges for the provider. Washington-based Providence also reported an operating loss for 2020. However, both Sutter and Providence were able to post positive net income thanks in large part to investment gains.
Investment income can aid nonprofit operators even when core operations are stunted like during 2020. Though, initially, the pandemic put stress on the stock market as uncertainty around the virus and its duration ballooned. The stock market took a dive and it was reflected in some six-month financials as both operations and investments took a hit.
“COVID and the stimulus is (hopefully) a once in a lifetime disruption of operations,” Holloran said, who noted analysts have been trying to assess whether the top line losses can be placed squarely on COVID-19. If that’s the case, analysts are typically more apt to keep the provider’s existing rating.
“For the most part providers were dependent on that CARES funding. I think they would have been in the red or break even without it,” Suzie Desai, a senior director at S&P Global Ratings, said.
For example, Arizona’s Banner Health would have posted an operating loss without federal relief, according to their financial reports. Banner Health was able to work its way back to black after it reported a loss through the first six months of the year. The same was true for Midwest behemoth Advocate Aurora.
The providers that were able to weather the storm of the pandemic tended to be integrated systems that had a health plan under their umbrella.
Kaiser Permanente ended the year with both positive operating and net income and returned relief funds it received.
“The integrated providers, yeah, were one group that just had a natural hedge with the insurance premiums still coming in,” Desai said.
Still, the hospital lobby is hoping to secure more funding for its members as the threat of the virus is still present even amid large scale efforts to vaccinate a majority of Americans to reach a blanket of protection from the novel coronavirus and its variants.
The Democratic bill has $410 billion in stimulus checks and $360 billion in aid to state and local governments.
Expanded unemployment benefits cost $242 billion.
School spending is nearly $170 billion spread out over 10 years.
There are a few big chunks of money in the American Rescue Plan Act that have generated a lot of news coverage and are pretty well known. In response to a reader’s request, we present the whopping $1.86 trillion spending plan in pie chart form.
There are the $1,400 checks (or more likely deposits) to many citizens or permanent legal residents and their dependents. That comes to about $410 billion.
Aid to state, local, territorial and tribal governments costs about $360 billion.
The bill boosts and extends unemployment benefits. Add another $242 billion.
Over the next 10 years, the law spends nearly $170 billion on education. That includes $129 billion for K-12 schools — both public and private — and about $40 billion for higher education.
The money for vaccines and corralling the coronavirus became a political talking point. Democrats touted the $20-25 billion they included for vaccine supplies and research. Republicans argued that the bill spent less than 10% of its total cost on COVID-19.
People will parse the numbers in different ways. Some only count money spent directly on vaccine production. Some look more broadly at the economic damage wrought by the virus. We looked for money that went towards health care, whether that meant improving treatment on tribal lands, adding health care workers at clinics, or anything that reduced the health impacts of the pandemic.
We put the bill’s total public health spending at $143 billion.
Within that, the single biggest line item is $47.8 billion for mitigating the disease, a broad description that includes testing and surveillance. There is also $15 billion for COVID-related health care for veterans, $7.6 billion to help community health centers distribute vaccines, and about the same amount to the Centers for Disease Control and Prevention for roughly the same purpose.
The chart above lays out how the money breaks down.
All of the amounts so far come to $1.3 trillion over 10 years.The bill’s total cost is $1.86 trillion, which leaves about $500 billion dollars to flesh out.
The law has over $40 billion for child care. Money to keep people in their homes and to house the homeless comes to about $44 billion. There is $10 billion to put food on people’s tables. The expected cost of temporarily boosting the child tax credit is $109 billion.
In our chart, we fold all of that, plus subsidies for pensions and health insurance premiums, into the category of support for families. Our total is $352 billion.
Our last distinct category is transportation. Under that umbrella, we put $30 billion for mass transit, $15 billion for the airline industry, $8 billion for airports, and other related activities. That came to $58 billion.
The catch-all bucket of other spending includes items such as $66 billion for businesses, $50 billion for disaster relief at the Federal Emergency Management Agency, and $7 billion to expand broadband internet.
The financial challenges caused by the COVID-19 pandemic forced hundreds of hospitals across the nation to furlough, lay off or reduce pay for workers, and others have had to scale back services or close.
Lower patient volume, canceled elective procedures and higher expenses tied to the pandemic have created a cash crunch for hospitals, and hospitals are taking a number of steps to offset financial damage. Executives, clinicians and other staff are taking pay cuts, capital projects are being put on hold, and some employees are losing their jobs. More than 260 hospitals and health systems furloughed workers in the last year, and dozens of others have implemented layoffs.
Below are six hospitals and health systems that are laying off employees in the next 2 months. Some of the layoffs were attributed to financial strain caused by the pandemic.
1. Sacramento, Calif.-based Sutter Healthis laying off hundreds of employees, most of whom work in information technology. In a filing with the state, Sutter said it plans to lay off 277 employees on April 2. The 277 jobs being eliminated include 92 analysts, 43 engineers and 28 project managers, according to the Sacramento Business Journal, citing the system’s filing with California’s Employment Development Department.
2. Plattsburgh, N.Y.-based Champlain Valley Physicians Hospitalplans to cut 60 jobs. The hospital, which is facing a $6.5 million deficit in fiscal year 2021, said the cuts include 10 people who were laid off or had permanent hour reductions, 12 people who are planning retirement, and the rest are open positions that will not be filled.
3. Hialeah (Fla.) Hospital is closing its maternity ward and laying off 62 employees April 5, according to a notice filed with the state. Most of those affected by the layoffs are registered nurses.
4. The outgoing owners of Providence Behavioral Health Hospitalin Holyoke, Mass., are laying off the hospital’s 151 employees, effective April 20, according to MassLive. Trinity Health of New England, part of Livonia, Mich.-based Trinity Health, is selling the hospital to Health Partners New England, which plans to take over the hospital April 20.
5. Olympia Medical Center in Los Angeles is slated to close March 31. The closure will result in the layoffs of about 450 employees.
6. Minneapolis-based Children’s Minnesota is laying off 150 employees, or about 3 percent of its workforce. Children’s Minnesota cited several reasons for the layoffs, including the financial hit from the COVID-19 pandemic. Some layoffs occured in December and the rest will occur at the end of March.
One year after the World Health Organization declared COVID-19 a pandemic, the end of that pandemic is within reach.
The big picture:The death and suffering caused by the coronavirus have been much worse than many people expected a year ago — but the vaccines have been much better.
Flashback: “Bottom line, it’s going to get worse,” Anthony Fauci told a congressional panel on March 11, 2020, the day the WHO formally declared COVID-19 to be a global pandemic.
A year ago today, the U.S. had confirmed 1,000 coronavirus infections. Now we’re approaching 30 million.
In the earliest days of the pandemic, Americans were terrified by the White House’s projections — informed by well-respected modeling — that 100,000 to 240,000 Americans could die from the virus. That actual number now sits at just under 530,000.
Many models at the time thought the virus would peak last May. It was nowhere close to its height by then. The deadliest month of the pandemic was January.
Yes, but: Last March, even the sunniest optimists didn’t expect the U.S. to have a vaccine by now.
They certainly didn’t anticipate that over 300 million shots would already be in arms worldwide, and they didn’t think the eventual vaccines, whenever they arrived, would be anywhere near as effective as these shots turned out to be.
Where it stands: President Biden has said every American adult who wants a vaccine will be able to get one by the end of May, and the country is on track to meet that target.
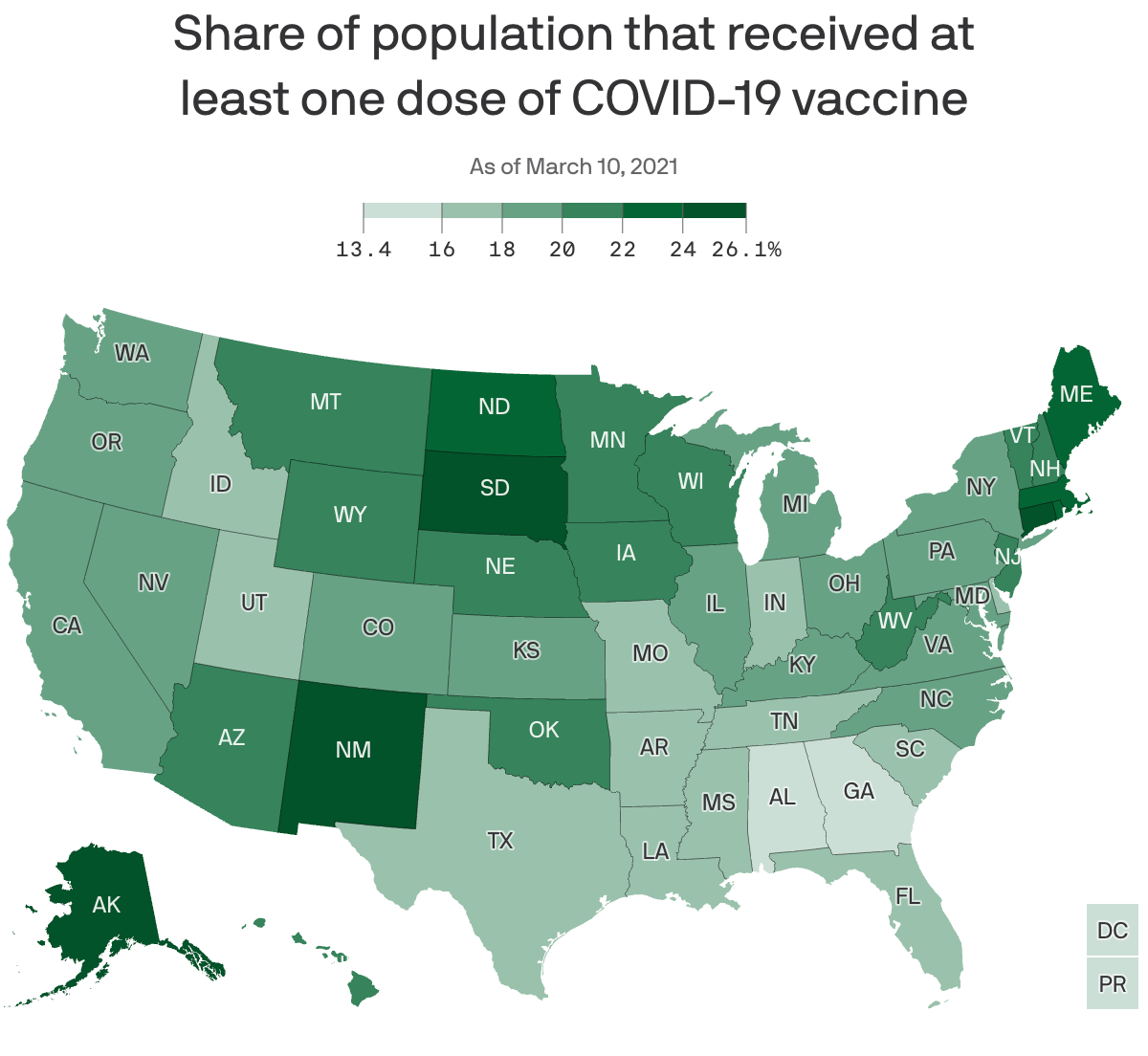
The U.S. is administering over 2 million shots per day, on average. Roughly 25% of the adult population has gotten at least one shot.
The federal government has purchased more doses than this country will be able to use: 300 million from Pfizer, 300 million from Moderna and 200 million from Johnson & Johnson.
The Pfizer and Moderna orders alone would be more than enough to fully vaccinate every American adult. (The vaccines aren’t yet authorized for use in children.)
Yes, millions of Americans are still anxiously awaiting their first shot — and navigating signup websites that are often frustrating and awful.
But the supply of available vaccines is expected to surge this month, and the companies say the bulk of those doses should be available by the end of May.
Cases, hospitalizations and deaths are all falling sharply at the same time vaccinations are ramping up.
The bottom line: Measured in death, loss, isolation and financial ruin, one year has felt like an eternity. Measured as the time between the declaration of a pandemic and vaccinating 60 million Americans, one year is an instant.
The virus hasn’t been defeated, and may never fully go away. Getting back to “normal” will be a moving target. Nothing’s over yet. But the end of the worst of it — the long, brutal nightmare of death and suffering — is getting close.
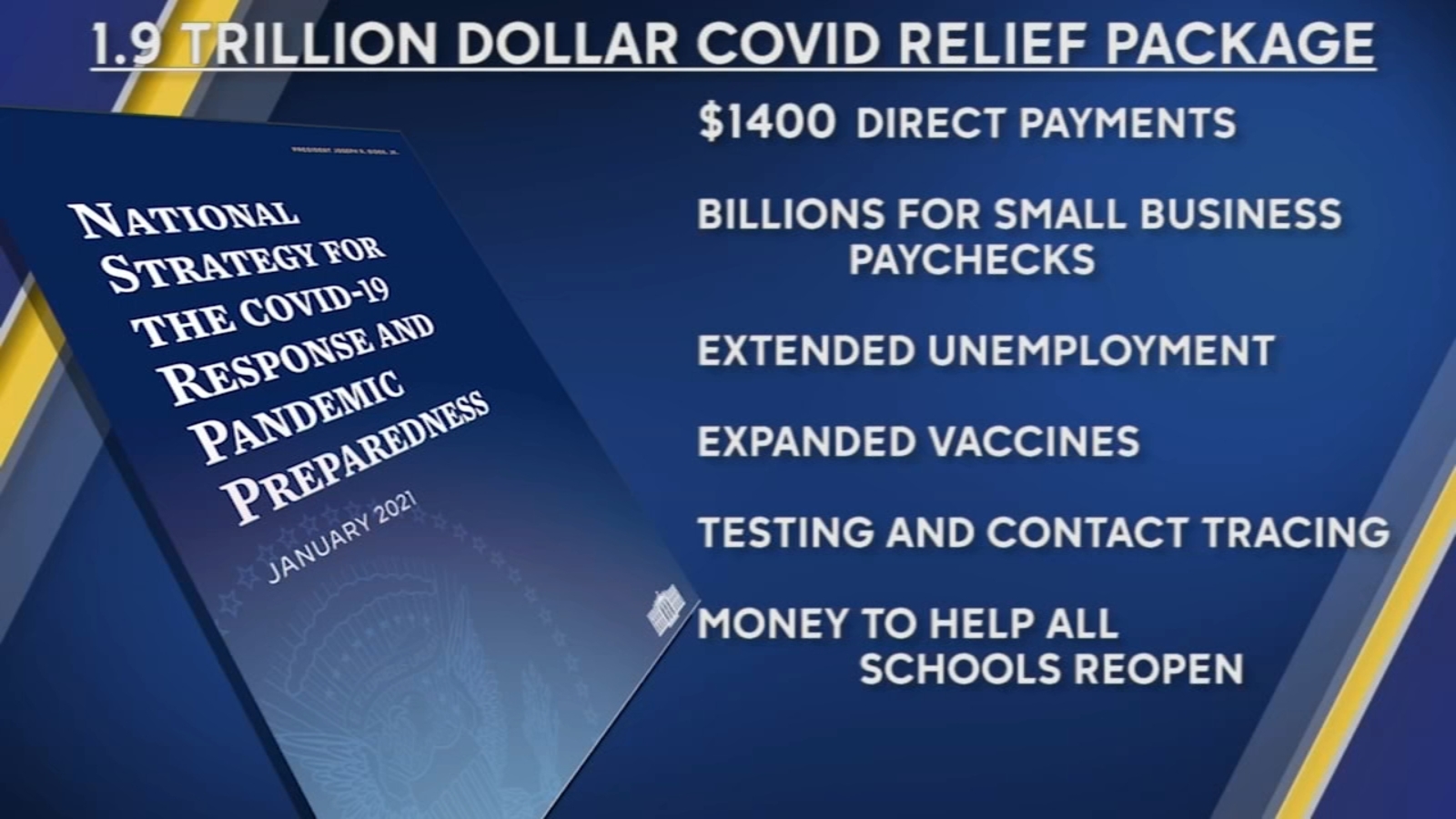
The House on Wednesday passed the mammoth $1.9 trillion COVID-19 relief package, which President Biden is expected to sign Friday.
The House approved the relief package in a starkly partisan 220-211 vote, sending the legislation to the White House and clinching Democrats’ first big legislative victory in the Biden era. No Republicans voted for the package and all but one House Democrat—Rep. Jared Golden of Maine—supported it. The Hill’s Cristina Marcos has more here.
The political split: Unlike the previous relief measures enacted last year, Democrats barely bothered to negotiate with Republicans and pushed the relief package through Congress along party lines using the budget reconciliation process. That allowed them to go as big as they wanted to go without running into a Senate GOP filibuster.
Republicans argue the use of a process dodging the filibuster shows Biden wasn’t serious about bringing unity, and House GOP lawmakers on Wednesday warned of the bill’s total cost.
But Democrats think Republicans will pay for their opposition to the popular bill and argued that they would oppose anything Biden proposed.
What’s in the $1.9T COVID-19 relief package: Along with $1,400 direct payments to households, an extension of expanded unemployment benefits, and aid for state and local governments, the package is loaded with other provisions intended to speed up the recovery from the recession and help struggling families fight the impact of COVID-19.
Tax credits: The bill increases the child tax credit for households below certain income thresholds for 2021 and makes it fully refundable, and also expands the earned income tax credit for the year.
Child care: $15 billion for grants to help low-income families afford child care and increases the child and dependent care tax credit for one year.
Pensions: $86 billion to bailout struggling union pension funds.
Transportation: $30 billion to bolster local subway and bus systems, $8 billion for airports, $1.5 billion for furloughed Amtrak workers, and $3 billion for wages at aerospace companies.
Housing: $27.4 billion in emergency rental assistance, another $10 billion to help homeowners avoid foreclosure, $5 billion in vouchers for public housing, $5 billion to tackle homelessness and $5 billion more to help households cover utility bills.
Small businesses: The American Rescue Plan broadens eligibility guidelines for the Paycheck Protection Program, allowing more nonprofit entities to be eligible, adds $15 billion in emergency grants and also sets aside more than $28 billion in funding for restaurants.
ObamaCare subsidies and Medicaid expansion: The bill increases ObamaCare subsidies through 2022 to make them more generous, a longtime goal for Democrats, and opens up more fully subsidized plans to individuals. It also would provide extra Medicaid funding to states that expand the program and have yet to do so.
The U.S. may be on the verge of another surge in coronavirus cases, despite weeks of good news.
The big picture:Nationwide, progress against the virus has stalled. And some states are ditching their most important public safety measures even as their outbreaks are getting worse.
Where it stands: The U.S. averaged just under 65,000 new cases per day over the past week. That’s essentially unchanged from the week before, ending a six-week streak of double-digit improvements.
Although the U.S. has been moving in the right direction, 65,000 cases per day is not a number that indicates the virus is under control. It’s the same caseload the U.S. was seeing last July, at the height of the summer surge in cases and deaths.
What we’re watching: Texas Gov. Greg Abbott on Tuesday rescinded the state’s mask mandate and declared that businesses will be able to operate at full capacity, saying risk-mitigation measures are no longer necessary because of the progress on vaccines.
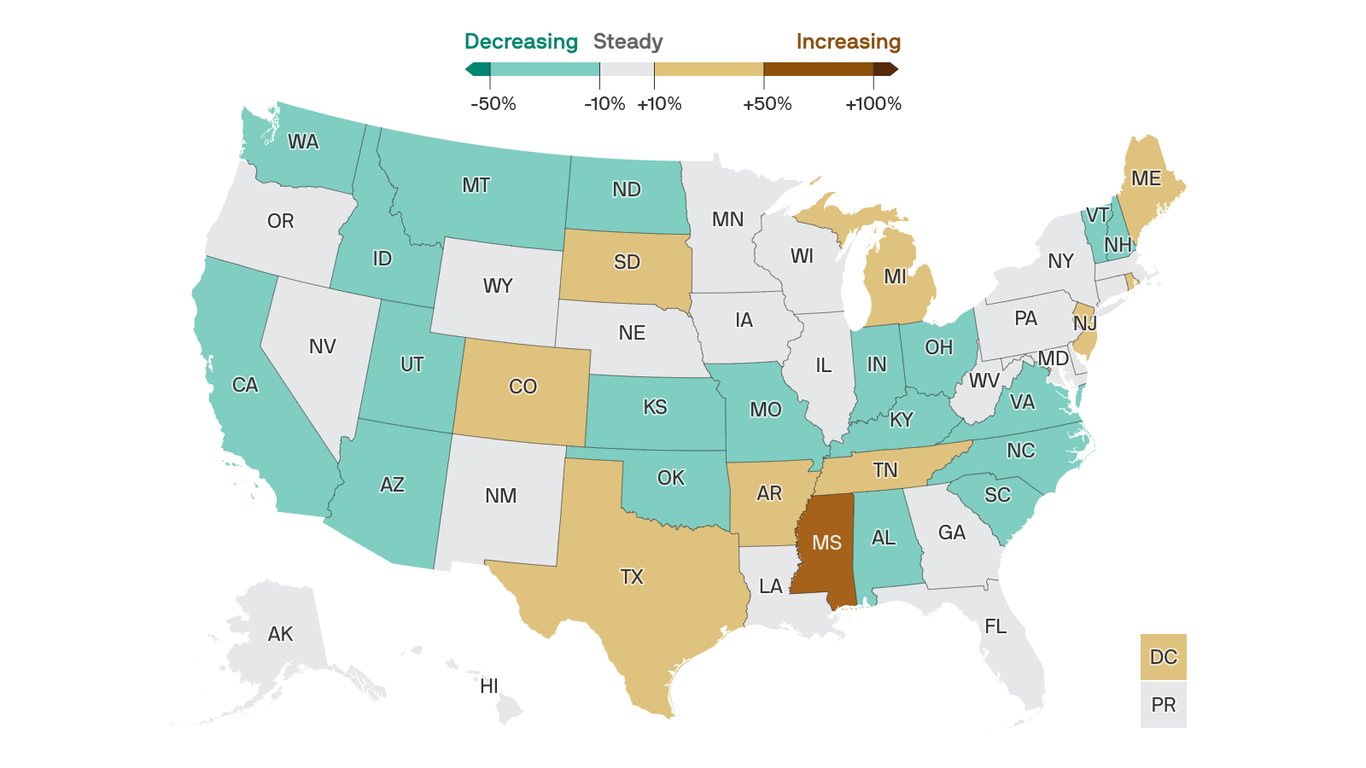
But the risk in Texas is far from over. In fact, its outbreak is growing: New cases in the state rose by 27% over the past week.
Mississippi Gov. Tate Reeves also scrapped all business restrictions, along with the state’s mask mandate, on Tuesday. New cases in Mississippi were up 62% over the past week, the biggest jump of any state.
The daily average of new daily cases also increased in eight more states, in addition to Mississippi and Texas.
How it works:If Americans let their guard down too soon, we could experience yet another surge — a fourth wave — before the vaccination campaign has had a chance to do its work.
The vaccine rollout is moving at breakneck speed. The U.S. should have enough doses for every adult who wants one by May, President Biden said this week.
At the same time, however, more contagious variants of the coronavirus are continuing to gain ground, meaning that people who haven’t gotten their vaccines yet may be spreading and contracting the virus even more easily than before.
What’s next: The bigger a foothold those variants can get, the harder it will be to escape COVID-19 — now or in the future.
The existing vaccines appear to be less effective against two variants, discovered in South Africa and Brazil, which means the virus could keep circulating even in a world where the vast majority of people are vaccinated.
And that means it’s increasingly likely that COVID-19 will never fully go away — that outbreaks may flare up here and there for years, requiring vaccine booster shots as well as renewed protective measures.
The bottom line: Variants emerge when viruses spread widely, which is also how people die.
Whatever “the end of the pandemic” looks like — however good it’s possible for things to get — the way to get there is through ramping up vaccinations and continuing to control the virus through masks and social distancing. Not doing those things will only make the future worse.
“Getting as many people vaccinated as possible is still the same answer and the same path forward as it was on December 1 or January 1 … but the expected outcome isn’t the same,” Shane Crotty, a virologist at the La Jolla Institute for Immunology in San Diego, told Reuters.
Dr. Christine Choi, 32, a medical resident at Harbor-UCLA Medical Center in Torrance, prepares to enter an isolation area for COVID-19 inpatients. Health care providers must face daily patient death and suffering.
Soon after the COVID-19 pandemic began last spring, Christine Choi, DO, a second-year medical resident at Harbor-UCLA Medical Center, volunteered to enter COVID-19 patient rooms. Since then, she has worked countless nights in the intensive care unit in full protective gear, often tasked with giving the sickest patients and their families the grim choice between intubation or near-certain death.
“I’m offering this guy two terrible options, and that’s how I feel about work: I can’t fix this for you and it sucks, and I’m sorry that the choices I’m giving you are both terrible,” Choi told the Los Angeles Times’ Soumya Karlamangla about one patient encounter.
While Choi exhibits an “almost startlingly positive attitude” in her work, it’s no match for the psychological burdens placed on her shoulders by the global pandemic, Karlamangla wrote. When an older female COVID-19 patient died in the hospital recently, her husband — in the same hospital with the same diagnosis — soon began struggling to breathe. Sensing that he had little time left, Choi held a mobile phone at his bedside so that each of his children could come on screen to tell him they loved him. “I was just bawling in my [personal protective equipment],” Choi said. “The sound of the family members crying — I probably will never forget that,” she said.
It was not the first time the young doctor helped family members say goodbye to a loved one, and it would not be the last. Health care providers like Choi have had to work through unimaginable tragedies and unprecedented circumstances because of COVID-19, with little time to dedicate to their own mental health or well-being.
It has been nearly a year since the US reported what was believed at the time to be its first coronavirus death in Washington State. Since then, the pandemic death toll has mushroomed to nearly 500,000 nationwide, including 49,000 Californians. These numbers are shocking, and yet they do not capture the immeasurable emotional weight that falls on the health care providers with the most intimate view of COVID-19’s deadly progression.“The horror of the pandemic has unfolded largely outside public view and inside hospitals, piling a disproportionate share of the trauma on the people whose work takes them inside their walls,” Karlamangla wrote.
Experts are deeply concerned about the psychological and physical burdens that providers must bear, and the fact that there is still no end in sight. “At least with a natural disaster, it happens, people get scattered all over the place, property gets damaged or flooded, but then we begin to rebuild,” Lawrence Palinkas, PhD, MA, a medical anthropologist at USC, told Karlamangla. “We’re not there yet, and we don’t know when that will actually occur.”
Sixty-eight percent of providers said they feel emotionally drained from their work, 59% feel burned out, 57% feel overworked, and 50% feel frustrated. The poll asked providers who say they feel burned out what contributes most to that viewpoint. One doctor from the Central Valley wrote:
“Short staffed due to people out with COVID. I’m seeing three times as many patients, with no time to chart or catch up. Little appreciation or contact from my bosses. I have never had an N95 [mask]. The emotional toll this pandemic is taking. Being sick myself and spreading it to my wife and young kids. Still not fully recovered but needing to be at work due to physician shortages. Lack of professional growth, and a sense of lack of appreciation at work and feeling overworked. The sadness of the COVID-related deaths and the stories that go along with the disease. That’s a lot of stuff to unpack.”
The pandemic has been especially challenging for female health providers, who compose 77% of health care workers with direct patient contact. “The pandemic exacerbated gender inequities in formal and informal work, and in the distribution of home responsibilities, and increased the risk of unemployment and domestic violence,” an international group of experts wrote in the Lancet. “While trying to fulfill their professional responsibilities, women had to meet their families’ needs, including childcare, home schooling, care for older people, and home care.”
For one female doctor from the Bay Area who responded to the CHCF survey, the extra burdens of the pandemic have been unrelenting: “Having to work more, lack of safe, affordable, available childcare while I’m working. As a single mother, working 15 hours straight, then having to care for my daughter when I get home. Just exhausted with no days off. So many Zoom meetings all day long. Miss my family and friends.”
It is unclear how the pandemic will affect the health care workforce in the long term. For now, the damage “can be measured in part by a surge of early retirements and the desperation of community hospitals struggling to hire enough workers to keep their emergency rooms running,” Andrew Jacobs reported in the New York Times.
One of the early retirements Jacobs cited was Sheetal Khedkar Rao, MD, a 42-year-old internist in suburban Chicago. Last October, she decided to stop practicing medicineafter “the emotional burden and moral injury became too much to bear,” she said. Two of the main factors driving her decision were a 30% pay cut to compensate for the decline in revenue from primary care visits and the need to spend more time at home after her two preteen children switched to remote learning.
“Everyone says doctors are heroes and they put us on a pedestal, but we also have kids and aging parents to worry about,” Rao said.
Working Through Unremitting Sickness and Death
In addition to the psychological burden, health care providers must cope with a harsh physical toll. People of color account for most COVID-19 cases and deaths among health care workers, according to a KFF issue brief. Some studies show that health care workers of color “are more likely to report reuse of or inadequate access to [personal protective equipment] and to work in clinical settings with greater exposure to patients with COVID-19.”
“Lost on the Frontline,” a collaboration of Kaiser Health News and the Guardian, has counted more than 3,400 deaths among US health care workers from COVID-19. Eighty-six percent of the workers who died were under age 60, and nurses accounted for roughly one-third of the deaths.
“Lost on the Frontline” provides the most comprehensive picture available of health care worker deaths, because the US still lacks a uniform system to collect COVID-19 morbidity and mortality data among health care workers. A year into the project, the federal government has decided to take action. Officials at the US Department of Health and Human Services cited the project when asking the National Academies of Sciences, Engineering, and Medicine for a rapid expert consultation to understand the causes of deaths among health care workers during the pandemic.
The National Academies’ report, published December 10, recommends the “adoption and use of a uniform national framework for collecting, recording, and reporting mortality and morbidity data” along with the development of national reporting standards for a core set of morbidity impacts, including mental well-being and psychological effects related to working through public health crises. Some health care experts said the data gathering could be modeled on the federal government’s World Trade Center Health Program, which provides no-cost medical monitoring and treatment for workers who responded to the 9/11 terrorist attacks 20 years ago.
“We have a great obligation to people who put their lives on the line for the nation,” Victor J. Dzau, MD, president of the National Academy of Medicine, told Jacobs.