
Thought of the Day: On Unity
https://www.axios.com/2022/11/03/gop-floats-medicare-reform

Some House Republicans aren’t waiting for the election to think about overhauling Medicare. But it’s hard to tell if there are specifics behind the talking point.
Why it matters: Past GOP attempts to cut Medicare landed with a thud, and Democrats in recent weeks have been hammering on the message that Republicans are intent on gutting the program.
What they’re saying: “If we’re going raise the debt ceiling, we can’t just raise it without focusing on some way to address the debt and the deficit,” Rep. Bruce Westerman (R-Ark.), a member of the House GOP’s health care task force, told Axios, adding Medicare should be made “sustainable over time.”
Yes, but: Not all Republicans are eager to kick off their time in the majority with another grinding health care fight against a Democratic president. Health policy experts are also skeptical of how realistic Medicare reform may be, recalling failed GOP agendas from the pre-Trump years.
The big picture: While a GOP Medicare push is not certain, Democrats are seizing on the possibility.
Between the lines: Republicans are not being specific about the changes they would push. But there’s a limited universe of possibilities.
The bottom line: Republicans point to the Medicare trust fund’s projected insolvency date in 2028 to argue change is needed to make the program sustainable. But any change is hard, and cuts that hit beneficiaries are not the only way to seek savings.
https://www.axios.com/2022/10/20/midterm-election-voters-health-care
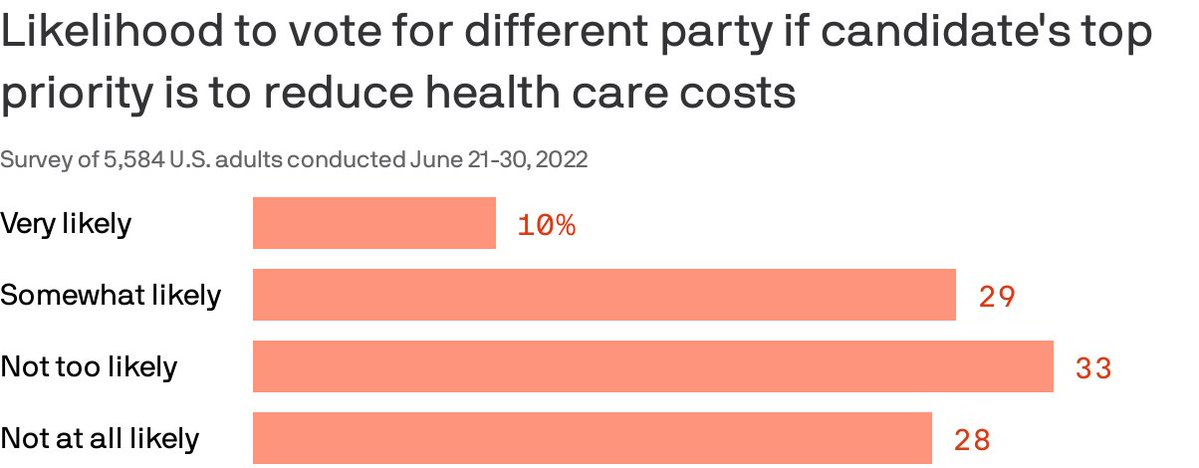
Almost 40% of Americans are willing to split their ticket and vote for a candidate from the opposing party who made a top priority of lowering health costs, according to a Gallup/West Health poll published Thursday.
Why it matters: Though candidates haven’t been talking much about medical costs in the run-up to the midterms, the issue remains enough of a priority that it could erode straight party-line voting.
By the numbers: 87% of Americans polled said a candidate’s plan to reduce the cost of health care services was very or somewhat important in casting a vote.
Of note: Democratic voters were more likely than Republicans to say they would cross party lines because health costs are a top priority. Four in 10 Democrats said they were likely to do so compared to about 1 in 5 Republicans.

Healthcare professionals in Oklahoma who have cared for COVID-19 patients throughout the pandemic are now facing a facility lockdown due to threats made against them.
Mercy Hospital Oklahoma City upped its security and locked down its intensive care unit following online threats against the facility and its staff, mostly revolving around COVID treatments and conspiracy theories, Becker’s Hospital Review reported.
Claims made during a recent protest outside the facility and online included that the hospital had a “Fauci protocol,” and that it received government vouchers for using certain medications or treatments for COVID patients, which Mercy Hospital denied, according to Becker’s.
Hospital officials released a statement to staff on Friday, which they shared with MedPage Today. “There is truly nothing more important to us than your safety. We have a team monitoring these online attacks in real time. Every level of our ministry is deeply concerned and committed to doing whatever it takes to protect our co-workers against these baseless attacks,” they said.
“We are proud to serve with you,” they added. “We know you are tired and weary, but please try your best to put these baseless claims out of your mind. Remember, you are called to serve our patients and each other. We are praying for peace and protection over each of you, as well as the protection of all our patients and visitors, while we take action on your behalf.”
Late last week, the hospital filed a restraining order against the founder and director of an Oklahoma church group that has been protesting outside the facility and making threats against its staff online, Oklahoma’s KFOR reported.
In a recent press release, the church group, known as Ekklesia Oklahoma, called Mercy Hospital an “evil Marxist controlled death camp.”
Court documents stated that the founder of the group called one of the hospital’s doctors a “murderer,” noting that members even posted the doctor’s home address online, according to KFOR.
Hospital officials told KFOR that they are thankful for local police departments that are providing extra security for staff and patients.
Other hospitals across the U.S. have also received threats to the safety of healthcare workers in recent days.
Last week, the Massachusetts Medical Society said it was “angered” over the recent neo-Nazi protest outside Brigham and Women’s Hospital in Boston that targeted two doctors whose work focuses on health equity.
Carole Allen, MD, MBA, president of the society, told MedPage Today that the protest outside Brigham and Women’s was a threat to healthcare workers who were just trying to do their jobs, as well as to patients, and was so disruptive that it “could endanger healthcare in general.”

The website for the group Physicians for Informed Consent (PIC) reads like an apolitical, educational resource that provides information on vaccines and why they shouldn’t be government-mandated. Its mission is “that doctors and the public are able to evaluate the data on infectious diseases and vaccines objectively, and voluntarily engage in informed decision-making about vaccination.”
The group’s accompanying social media accounts, however, tell a different story. On PIC’s Facebook, Twitter, Instagram, and LinkedIn feeds, you’ll find post after post about reasons to be scared of vaccines – especially for children – often highlighting selective portions of scientific research that contain vaccination risks.
Who’s Behind PIC?
The group was founded in 2015 after California passed a law that prohibited the use of personal belief exemptions from vaccinations required for children to attend any public or private school in the state.
Three years later, the number of waivers issued by doctors to parents seeking medical exemptions for their children tripled. As a result, another law was passed in 2019, cracking down on the inappropriate use of medical exemptions.
The group’s founder, Shira Miller, MD, is a concierge integrative medicine doctor based in Los Angeles, specializing in menopausal care. On her own Twitter profile, she describes herself as “Facebook’s Most Popular Menopause Doctor.”
Miller earned her medical degree in 2002 from Technion-Israel Institute of Technology in Haifa, Israel, and has reportedly been working as a concierge physician since 2010.
PIC’s leadership team also includes 20 physicians from a wide range of specialties, most of whom, like Miller, don’t specialize in infectious diseases.
Among its leaders is Paul Thomas, MD, an Oregon-based pediatrician. Thomas, who is listed as one of PIC’s founding directors, was issued an emergency suspension order of his medical license in 2021 by the state medical board, in which they cited at least eight cases of alleged patient harm. In line with PIC’s philosophy, Thomas maintains that he isn’t “anti-vax” – he’s pro-informed-consent.
Also on the team is Jane Orient, MD, internist and executive director of the Association of American Physicians and Surgeons (AAPS), a group that also opposes vaccine mandates. Orient received her medical degree from Columbia University and currently practices in Arizona. In 2020, the AAPS sued the federal government for withholding its stockpile of hydroxychloroquine from COVID patients, despite research showing that the drug is ineffective. The complaint was dismissed in September 2021.
Doug Mackenzie, MD, a plastic surgeon who graduated from Johns Hopkins University of Medicine, is PIC’s treasurer. He has previously identified himself as an “ex-vaxxer” rather than an anti-vaxxer when speaking on a panel in 2019.
The only RN on the team is Tawny Buettner. After California mandated vaccinations for healthcare workers, Buettner organized a protest outside of her place of work, Rady Children’s Hospital in San Diego; she later sued the hospital after she was dismissed from her job. According to the complaint, Buettner and the 36 other plaintiffs alleged that their requests for religious exemptions from the COVID-19 vaccine were all denied.
Kenneth Stoller, MD, also listed on the leadership team, graduated from the American University of the Caribbean School of Medicine and completed pediatric residency training at the University of California Los Angeles. Stoller was disciplined in 2019 for doling out medical exemptions to children without adequate evidence. According to state records, his license in California has since been revoked; he currently holds a medical license in New Mexico.
What’s PIC?
The most notable physician groups accused of spreading COVID-19 misinformation since the vaccine rollout have been affiliated with right-wing media, if not overtly proclaiming conservative, anti-vaccination beliefs.
For example, America’s Frontline Doctors, a group notorious for its support of hydroxychloroquine as a treatment for COVID-19, has made its values well-known. The group’s founder, Simone Gold, MD, JD, was arrested for participating in the Jan. 6 capitol riot and has openly opposed mask-wearing. Similarly, physician leaders of the Front Line COVID-19 Critical Care Alliance, known for promoting the use of ivermectin to treat COVID-19, tout their appearances on the ultra-conservative Newsmax on the website’s homepage.
PIC wants to be different. The group’s focus, according to its general counsel Greg Glaser, JD, of Copperopolis, California, is on the “authoritative citations that show, or calculate, the risks [of vaccines] to the public,” he told MedPage Today.
“We are pro-informed consent, pro-ethics, pro-health. PIC is not anti-vaccine, and PIC is not pro-vaccine – PIC is neutral,” Glaser said on behalf of the group.
In August 2021, Glaser submitted an amicus brief to the Supreme Court PIC’s behalf, arguing against the implementation of vaccine mandates. The document claims that “government statements confirm there is no evidence that COVID-19 vaccines prevent the spread of SARS-CoV-2 or COVID-19,” ignoring the breadth of existing literature that says otherwise.

America was not prepared for COVID-19 when it arrived. It was not prepared for last winter’s surge. It was not prepared for Delta’s arrival in the summer or its current winter assault. More than 1,000 Americans are still dying of COVID every day, and more have died this year than last. Hospitalizations are rising in 42 states. The University of Nebraska Medical Center in Omaha, which entered the pandemic as arguably the best-prepared hospital in the country, recently went from 70 COVID patients to 110 in four days, leaving its staff “grasping for resolve,” the virologist John Lowe told me. And now comes Omicron.
Will the new and rapidly spreading variant overwhelm the U.S. health-care system? The question is moot because the system is already overwhelmed, in a way that is affecting all patients, COVID or otherwise. “The level of care that we’ve come to expect in our hospitals no longer exists,” Lowe said.
The real unknown is what an Omicron cross will do when it follows a Delta hook. Given what scientists have learned in the three weeks since Omicron’s discovery, “some of the absolute worst-case scenarios that were possible when we saw its genome are off the table, but so are some of the most hopeful scenarios,” Dylan Morris, an evolutionary biologist at UCLA, told me. In any case, America is not prepared for Omicron. The variant’s threat is far greater at the societal level than at the personal one, and policy makers have already cut themselves off from the tools needed to protect the populations they serve. Like the variants that preceded it, Omicron requires individuals to think and act for the collective good—which is to say, it poses a heightened version of the same challenge that the U.S. has failed for two straight years, in bipartisan fashion.
The coronavirus is a microscopic ball studded with specially shaped spikes that it uses to recognize and infect our cells. Antibodies can thwart such infections by glomming onto the spikes, like gum messing up a key. But Omicron has a crucial advantage: 30-plus mutations that change the shape of its spike and disable many antibodies that would have stuck to other variants. One early study suggests that antibodies in vaccinated people are about 40 times worse at neutralizing Omicron than the original virus, and the experts I talked with expect that, as more data arrive, that number will stay in the same range. The implications of that decline are still uncertain, but three simple principles should likely hold.
First, the bad news: In terms of catching the virus, everyone should assume that they are less protected than they were two months ago. As a crude shorthand, assume that Omicron negates one previous immunizing event—either an infection or a vaccine dose. Someone who considered themselves fully vaccinated in September would be just partially vaccinated now (and the official definition may change imminently). But someone who’s been boosted has the same ballpark level of protection against Omicron infection as a vaccinated-but-unboosted person did against Delta. The extra dose not only raises a recipient’s level of antibodies but also broadens their range, giving them better odds of recognizing the shape of even Omicron’s altered spike. In a small British study, a booster effectively doubled the level of protection that two Pfizer doses provided against Omicron infection.
Second, some worse news: Boosting isn’t a foolproof shield against Omicron. In South Africa, the variant managed to infect a cluster of seven people who were all boosted. And according to a CDC report, boosted Americans made up a third of the first known Omicron cases in the U.S. “People who thought that they wouldn’t have to worry about infection this winter if they had their booster do still have to worry about infection with Omicron,” Trevor Bedford, a virologist at Fred Hutchinson Cancer Research Center, told me. “I’ve been going to restaurants and movies, and now with Omicron, that will change.”
Third, some better news: Even if Omicron has an easier time infecting vaccinated individuals, it should still have more trouble causing severe disease. The vaccines were always intended to disconnect infection from dangerous illness, turning a life-threatening event into something closer to a cold. Whether they’ll fulfill that promise for Omicron is a major uncertainty, but we can reasonably expect that they will. The variant might sneak past the initial antibody blockade, but slower-acting branches of the immune system (such as T cells) should eventually mobilize to clear it before it wreaks too much havoc.
To see how these principles play out in practice, Dylan Morris suggests watching highly boosted places, such as Israel, and countries where severe epidemics and successful vaccination campaigns have given people layers of immunity, such as Brazil and Chile. In the meantime, it’s reasonable to treat Omicron as a setback but not a catastrophe for most vaccinated people. It will evade some of our hard-won immune defenses, without obliterating them entirely. “It was better than I expected, given the mutational profile,” Alex Sigal of the Africa Health Research Institute, who led the South African antibody study, told me. “It’s not going to be a common cold, but neither do I think it will be a tremendous monster.”
That’s for individuals, though. At a societal level, the outlook is bleaker.
Omicron’s main threat is its shocking speed, as my colleague Sarah Zhang has reported. In South Africa, every infected person has been passing the virus on to 3–3.5 other people—at least twice the pace at which Delta spread in the summer. Similarly, British data suggest that Omicron is twice as good at spreading within households as Delta. That might be because the new variant is inherently more transmissible than its predecessors, or because it is specifically better at moving through vaccinated populations. Either way, it has already overtaken Delta as the dominant variant in South Africa. Soon, it will likely do the same in Scotland and Denmark. Even the U.S., which has much poorer genomic surveillance than those other countries, has detected Omicron in 35 states. “I think that a large Omicron wave is baked in,” Bedford told me. “That’s going to happen.”
More positively, Omicron cases have thus far been relatively mild. This pattern has fueled the widespread claim that the variant might be less severe, or even that its rapid spread could be a welcome development. “People are saying ‘Let it rip’ and ‘It’ll help us build more immunity,’ that this is the exit wave and everything’s going to be fine and rosy after,” Richard Lessells, an infectious-disease physician at the University of KwaZulu-Natal, in South Africa, told me. “I have no confidence in that.”
To begin with, as he and others told me, that argument overlooks a key dynamic: Omicron might not actually be intrinsically milder. In South Africa and the United Kingdom, it has mostly infected younger people, whose bouts of COVID-19 tend to be less severe. And in places with lots of prior immunity, it might have caused few hospitalizations or deaths simply because it has mostly infected hosts with some protection, as Natalie Dean, a biostatistician at Emory University, explained in a Twitter thread. That pattern could change once it reaches more vulnerable communities. (The widespread notion that viruses naturally evolve to become less virulent is mistaken, as the virologist Andrew Pekosz of Johns Hopkins University clarified in The New York Times.) Also, deaths and hospitalizations are not the only fates that matter. Supposedly “mild” bouts of COVID-19 have led to cases of long COVID, in which people struggle with debilitating symptoms for months (or even years), while struggling to get care or disability benefits.
And even if Omicron is milder, greater transmissibility will likely trump that reduced virulence. Omicron is spreading so quickly that a small proportion of severe cases could still flood hospitals. To avert that scenario, the variant would need to be substantially milder than Delta—especially because hospitals are already at a breaking point. Two years of trauma have pushed droves of health-care workers, including many of the most experienced and committed, to quit their job. The remaining staff is ever more exhausted and demoralized, and “exceptionally high numbers” can’t work because they got breakthrough Delta infections and had to be separated from vulnerable patients, John Lowe told me. This pattern will only worsen as Omicron spreads, if the large clusters among South African health-care workers are any indication. “In the West, we’ve painted ourselves into a corner because most countries have huge Delta waves and most of them are stretched to the limit of their health-care systems,” Emma Hodcroft, an epidemiologist at the University of Bern, in Switzerland, told me. “What happens if those waves get even bigger with Omicron?”
The Omicron wave won’t completely topple America’s wall of immunity but will seep into its many cracks and weaknesses. It will find the 39 percent of Americans who are still not fully vaccinated (including 28 percent of adults and 13 percent of over-65s). It will find other biologically vulnerable people, including elderly and immunocompromised individuals whose immune systems weren’t sufficiently girded by the vaccines. It will find the socially vulnerable people who face repeated exposures, either because their “essential” jobs leave them with no choice or because they live in epidemic-prone settings, such as prisons and nursing homes. Omicron is poised to speedily recap all the inequities that the U.S. has experienced in the pandemic thus far.
Here, then, is the problem: People who are unlikely to be hospitalized by Omicron might still feel reasonably protected, but they can spread the virus to those who are more vulnerable, quickly enough to seriously batter an already collapsing health-care system that will then struggle to care for anyone—vaccinated, boosted, or otherwise. The collective threat is substantially greater than the individual one. And the U.S. is ill-poised to meet it.
America’s policy choices have left it with few tangible options for averting an Omicron wave. Boosters can still offer decent protection against infection, but just 17 percent of Americans have had those shots. Many are now struggling to make appointments, and people from rural, low-income, and minority communities will likely experience the greatest delays, “mirroring the inequities we saw with the first two shots,” Arrianna Marie Planey, a medical geographer at the University of North Carolina at Chapel Hill, told me. With a little time, the mRNA vaccines from Pfizer and Moderna could be updated, but “my suspicion is that once we have an Omicron-specific booster, the wave will be past,” Trevor Bedford, the virologist, said.
Two antiviral drugs now exist that could effectively keep people out of the hospital, but neither has been authorized and both are expensive. Both must also be administered within five days of the first symptoms, which means that people need to realize they’re sick and swiftly confirm as much with a test. But instead of distributing rapid tests en masse, the Biden administration opted to merely make them reimbursable through health insurance. “That doesn’t address the need where it is greatest,” Planey told me. Low-wage workers, who face high risk of infection, “are the least able to afford tests up front and the least likely to have insurance,” she said. And testing, rapid or otherwise, is about to get harder, as Omicron’s global spread strains both the supply of reagents and the capacity of laboratories.
Omicron may also be especially difficult to catch before it spreads to others, because its incubation period—the window between infection and symptoms—seems to be very short. At an Oslo Christmas party, almost three-quarters of attendees were infected even though all reported a negative test result one to three days before. That will make Omicron “harder to contain,” Lowe told me. “It’s really going to put a lot of pressure on the prevention measures that are still in place—or rather, the complete lack of prevention that’s still in place.”
The various measures that controlled the spread of other variants—masks, better ventilation, contact tracing, quarantine, and restrictions on gatherings—should all theoretically work for Omicron too. But the U.S. has either failed to invest in these tools or has actively made it harder to use them. Republican legislators in at least 26 states have passed laws that curtail the very possibility of quarantines and mask mandates. In September, Alexandra Phelan of Georgetown University told me that when the next variant comes, such measures could create “the worst of all worlds” by “removing emergency actions, without the preventive care that would allow people to protect their own health.” Omicron will test her prediction in the coming weeks.
The longer-term future is uncertain. After Delta’s emergence, it became clear that the coronavirus was too transmissible to fully eradicate. Omicron could potentially shunt us more quickly toward a different endgame—endemicity, the point when humanity has gained enough immunity to hold the virus in a tenuous stalemate—albeit at significant cost. But more complicated futures are also plausible. For example, if Omicron and Delta are so different that each can escape the immunity that the other induces, the two variants could co-circulate. (That’s what happened with the viruses behind polio and influenza B.)
Omicron also reminds us that more variants can still arise—and stranger ones than we might expect. Most scientists I talked with figured the next one to emerge would be a descendant of Delta, featuring a few more mutational bells and whistles. Omicron, however, is “dramatically different,” Shane Crotty, from the La Jolla Institute for Immunology, told me. “It showed a lot more evolutionary potential than I or others had hoped for.” It evolved not from Delta but from older lineages of SARS-CoV-2, and seems to have acquired its smorgasbord of mutations in some hidden setting: perhaps a part of the world that does very little sequencing, or an animal species that was infected by humans and then transmitted the virus back to us, or the body of an immunocompromised patient who was chronically infected with the virus. All of these options are possible, but the people I spoke with felt that the third—the chronically ill patient—was most likely. And if that’s the case, with millions of immunocompromised people in the U.S. alone, many of whom feel overlooked in the vaccine era, will more weird variants keep arising? Omicron “doesn’t look like the end of it,” Crotty told me. One cause for concern: For all the mutations in Omicron’s spike, it actually has fewer mutations in the rest of its proteins than Delta did. The virus might still have many new forms to take.
Vaccinating the world can curtail those possibilities, and is now an even greater matter of moral urgency, given Omicron’s speed. And yet, people in rich countries are getting their booster six times faster than those in low-income countries are getting their first shot. Unless the former seriously commits to vaccinating the world—not just donating doses, but allowing other countries to manufacture and disseminate their own supplies—“it’s going to be a very expensive wild-goose chase until the next variant,” Planey said.
Vaccines can’t be the only strategy, either. The rest of the pandemic playbook remains unchanged and necessary: paid sick leave and other policies that protect essential workers, better masks, improved ventilation, rapid tests, places where sick people can easily isolate, social distancing, a stronger public-health system, and ways of retaining the frayed health-care workforce. The U.S. has consistently dropped the ball on many of these, betting that vaccines alone could get us out of the pandemic. Rather than trying to beat the coronavirus one booster at a time, the country needs to do what it has always needed to do—build systems and enact policies that protect the health of entire communities, especially the most vulnerable ones.
Individualism couldn’t beat Delta, it won’t beat Omicron, and it won’t beat the rest of the Greek alphabet to come.
Self-interest is self-defeating, and as long as its hosts ignore that lesson, the virus will keep teaching it.
https://www.axios.com/gop-targets-dems-with-medicscare-ads-abc27c8c-f2d2-4e3d-9d4b-40a5552d4444.html
Conservative and industry groups are trying to whip up opposition to President Biden’s massive social spending plan by warning it will imperil Medicare benefits, Axios has learned.
Why it matters: “Medicscare” is a well-worn political tactic precisely because it can be effective. For Democrats, there’s zero room for defections against the $3.5 trillion proposal if they want to pass the bill.
What’s happening: Senior citizens in Arizona, represented by Sen. Kyrsten Sinema (D-Ariz.), potential Democratic holdout, have started receiving large boxes labeled “Medical Shipment. Please open immediately.”
Another nonprofit advocacy group, A Healthy Future, is targeting the prescription drug portions of the bill in a digital ad campaign aimed at key Democratic votes.
The big picture: Democrats have turned to drug pricing reforms to offset part of the legislation’s massive price tag, potentially paying for as much as $600 billion in new spending.
Yes, but: The Mediscare tactic is larger than just the drug pricing fight. Americans for Prosperity, the Koch-backed conservative advocacy group, is running its own ads warning of much larger impending Medicare cuts.

Howard Stern was reflecting this week on the coronavirus deaths of four conservative talk-radio hosts who had espoused anti-vaccine and anti-mask sentiments when he took aim at those who have refused to get vaccinated.
“I want my freedom to live,” he said Tuesday on his SiriusXM program. “I want to get out of the house. I want to go next door and play chess. I want to go take some pictures.”
The shock jock, who advocated for the coronavirus vaccine to be mandatory, then turned his attention to the hesitancy that has played a significant role in the U.S. spread of the virus, leading to what Rochelle Walensky, director of the Centers for Disease Control and Prevention, has called a “pandemic of the unvaccinated.”He pointed to unvaccinated people who are “clogging” up overwhelmed hospitals, calling them “imbeciles” and “nut jobs” and suggesting that doctors and nurses not treat those who have not taken a coronavirus vaccine.
“I’m really of mind to say, ‘Look, if you didn’t get vaccinated [and] you got covid, you don’t get into a hospital,’ ” he said. “You had the cure and you wouldn’t take it.”
Stern’s comments come after several other celebrities expressed to their large social media audiences their frustration with the ongoing lag in vaccinations when hospitals are being pushed to their limits by the highly transmissible delta variant.
More than 185,000 coronavirus infections were reported Wednesday across the United States, according to data compiled by The Washington Post. Nearly 102,000 people are hospitalized with covid-19; more than 26,000 are in intensive care units. A slight decline in hospitalizations over the past week has inspired cautious optimism among public health leaders.
While there is not a nationwide vaccine mandate, President Biden is expected to sign an executive order Thursday requiring that all federal employees be vaccinated, without an alternative for regular coronavirus testing to opt out of the mandate, The Post reported. The order affecting the estimated 2.1 million federal workers comes as Biden plans to outline a “robust plan to stop the spread of the delta variant and boost covid-19 vaccinations,” the White House said.
Health officials, doctors and nurses nationwide have urged those still hesitant to get vaccinated — and some have gone a step further. Jason Valentine, a physician in Mobile, Ala., informed patients last month that he would not treat anyone who was unvaccinated, saying there were “no conspiracy theories, no excuses” preventing anyone from being vaccinated. Linda Marraccini, a doctor in South Miami, said this month that she would not treat unvaccinated patients in person, noting that her office would “no longer subject our patients and staff to unnecessary risk.”
The summer surge also has led celebrities to use their platform to either call on unvaccinated people to get vaccinated or to denounce them for not doing so. Actor and activist Sean Penn said the vaccine should be mandatory and has called on Hollywood to implement vaccination guidelines on film sets. Actors Benicio Del Toro and Zoe Saldana were part of a vaccine video campaign this year to help debunk misinformation about coronavirus vaccination. When actress Melissa Joan Hart revealed her breakthrough coronavirus case last month, she said she was angry that the nation “got lazy” about getting vaccinated and that masking was not required at her children’s school.
Late-night talk host Jimmy Kimmel suggested Tuesday that hospitals shouldn’t treat unvaccinated patients who prefer to take ivermectin — a medicine long used to kill parasites in animals and humans that has soared in popularity despite being an unproven covid-19 treatment and the subject of warnings by health officials against its use for the coronavirus. After noting that Anthony S. Fauci, the chief medical adviser to Biden, warned that some hospitals might be forced to make “tough choices” on who gets an ICU bed, the late-night host quipped that the situation was not difficult.
“That choice doesn’t seem so tough to me,” Kimmel said. “Vaccinated person having a heart attack? Yes, come right in; we’ll take care of you. Unvaccinated guy who gobbled horse goo? Rest in peace, wheezy.”
Stern has featured front-line workers on his show and has advocated for people to get vaccinated against the coronavirus. In December, the host interviewed Cody Turner, a physician at the Cleveland Clinic, about how the front-line doctor struggled with his mental health while treating infected patients when a vaccine was not widely available.
“We are drowning and we are in hell, and people don’t understand, not only what’s happening to people, you know, but patients across this country,” Turner said.
Stern was a fierce critic of President Donald Trump’s response to the pandemic, saying last year that his former friend was “treasonous” for telling supporters to attend large rallies, despite the risk of infection, in the run-up to the presidential election.
On his eponymous program this week, Stern referred to four conservative talk-radio hosts who bashed the vaccine and eventually died of the virus: Marc Bernier, 65; Phil Valentine, 61; Jimmy DeYoung, 81; and Dick Farrel, 65. In the weeks and months leading up to their deaths last month, all four men had publicly shared their opposition to mainstream public health efforts when coronavirus infections were spiking.
“Four of them were like ranting on the air — they will not get vaccinated,” Stern said Tuesday. “They were on fire … they were all dying and then their dying words were, ‘I wish I had been more into the vaccine. I wish I had taken it.’ ”
After he played a clip of Bernier saying he would not get vaccinated, Stern suggested that the coronavirus vaccine be considered as normal as a measles or mumps vaccine.
“When are we going to stop putting up with the idiots in this country and just say it’s mandatory to get vaccinated?” he asked.
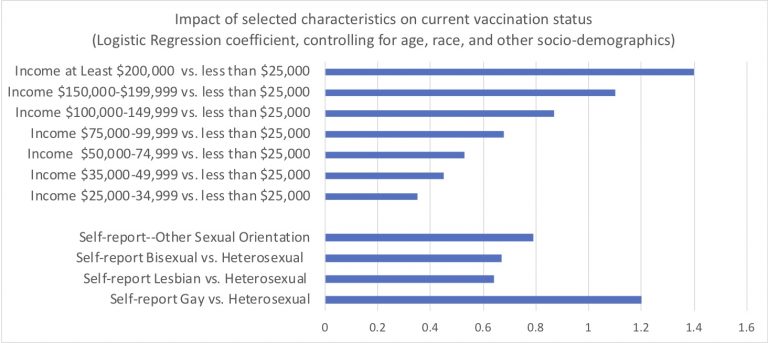
Last night I downloaded the latest Census Bureau July-August week 34 PULSE data. Over two cups of coffee, I ran the obvious multivariable logistic regressions to examine who is now fully vaccinated against COVID. See the above of this post for the full set of resulting Logit coefficients.
I’m sure Reviewer 2 would order due refinements to my quick analysis, were it immediately submitted for peer-review publication. My capacious study limitations section would note the inherent challenges of population surveys to gauge contentious questions like this. These data surely include response biases and likely overstate the true prevalence of COVID vaccination.
The overall patterns and disparities remain clear enough. Of course, we see huge disparities across regions, by education and by income. A bit more surprising: One group appears especially vulnerable and requires specific outreach…Yup. We must formulate culturally competent public health messaging for heterosexual non-Hispanic white Americans. This group conspicuously lags in vaccination status.
Among self-identified male respondents, heterosexual men were almost four times as likely to report not to be fully vaccinated (19%) as were gay men (5%)–an absolute different quite similar to the gradient observed between men with incomes less than $25,000 and those with incomes between $75,000 and $100,000.
I know that there daunting obstacles to reaching this disparity-population of heterosexual American men. We can’t let these barriers deter us. I’m joking–sort of. OK not really.
Political and social polarization are serious obstacles to our COVID efforts. Tribalization of public health may ironically increase vaccination rates among sexual and gender minorities, the educated, residents of blue states, and the socially liberal. We must find ways to push past these divides.

