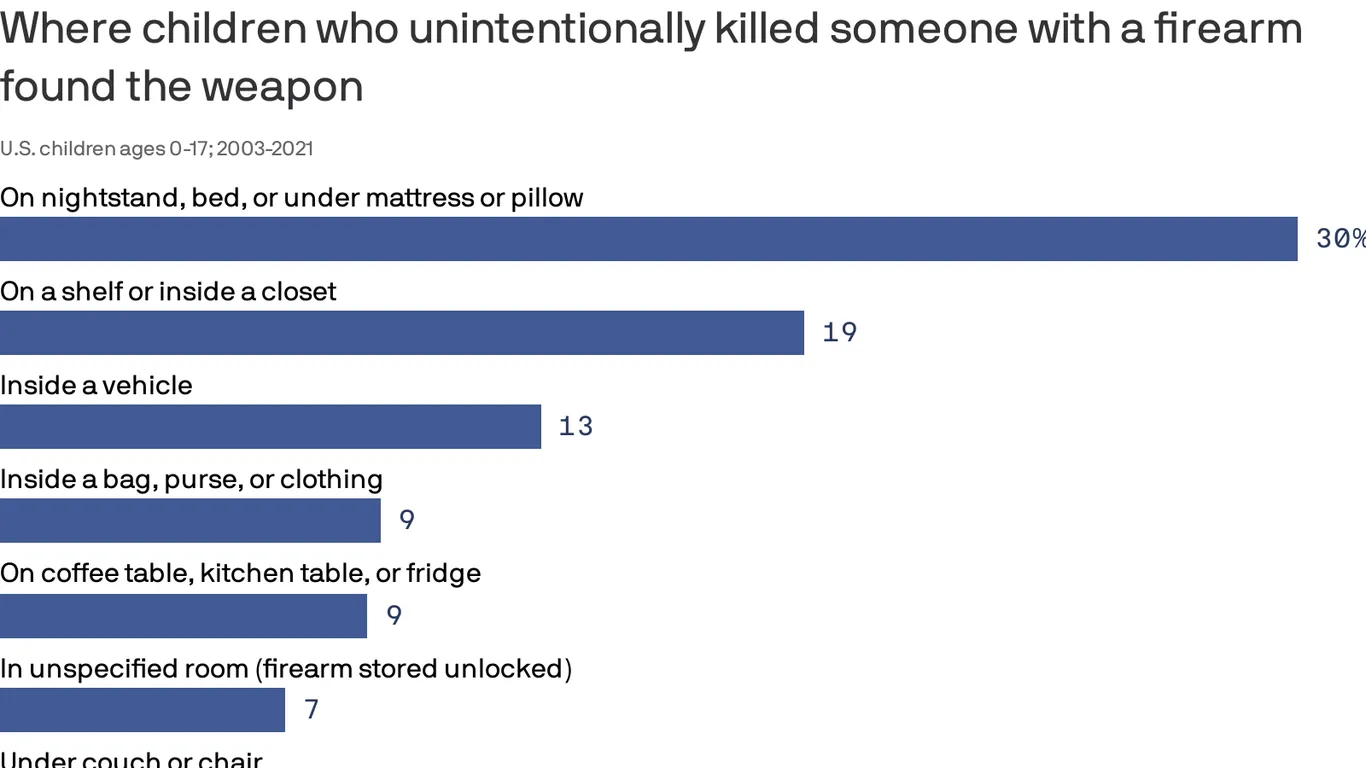
Children and teens involved in unintentional fatal shootings most commonly found the gun inside or on top of a nightstand, under a mattress or pillow, or on top of a bed, according to a new federal study.
Why it matters:
The data from the Centers for Disease Control and Prevention, which covers nearly 20 years of deadly firearm accidents among America’s youth, demonstrates why putting a gun out of sight or out of reach is not “safe storage,” federal researchers said.
It underscores the need for policymakers, health experts and parents to promote safe gun storage, they said.
Using data recorded between 2003 and 2021 by the National Violent Death Reporting System, researchers identified more than 1,250 unintentional gun deaths among kids.
The vast majority involved guns that were unlocked (76%), and most of those unlocked firearms were also loaded (91%).
Two-thirds (67%) of unintentional gun injury deaths among kids occurred when the shooter was playing with the gun or showing it to others.
In 30% of deaths, guns were found around nightstands and other sleeping areas.
Guns were also most commonly found on top of a shelf or inside a closet (18.6%) or inside a vehicle (12.5%).
I began to wonder if this trip to a pediatric urgent care with my son was even necessary.
Sure, he had been diagnosed with pneumonia a week ago and didn’t seem to be getting better. His cough sounded uglier. But here Ethan was in classic two-and-a-half-year-old mode: running in big circles around the waiting room chairs and causing the kind of ruckus only a toddler can.
He’d stuff some Pirate’s Booty I had hastily thrown into my purse in his mouth, before returning to his wild banshee ways and dashing around in circles again.
Our pediatrician said their office was too swamped with sick kids to see us, and referred us to this place. We had been told the wait to see a doctor would be a minimum of an hour. We struggled to find a seat in the packed waiting room as far as possible from other coughing kids.
We finally graduated from the waiting room to the doctor’s office, only for Ethan to continue his marathon by scooting a rolling chair back and forth, roaring with laughter every time it hit the examining table. When the physician walked in, I felt like I needed to defend wasting her time with this visit with my seemingly A-OK, albeit destructive, son.
But Ethan wasn’t OK.
The doctor listened to his chest with her stethoscope and didn’t like what she heard: wheezing, some crackling.
She showed me how Ethan’s Pirate’s Booty-stuffed stomach moved heavily each time he inhaled and exhaled.
They had Ethan complete a nebulizer treatment in the office, which meant slipping a device on his face that resembled an oxygen mask, while medicated air meant to open up his lungs flowed through a frightfully loud machine. I held him in my lap while the nebulizer was on, scrambling to find 100 different versions of “Wheels on the Bus” videos on YouTube to try to distract him from the vacuum-like whirring of the machine.
The doctor listened to his lungs again. His breathing still didn’t sound great, but she said the hospitals were too inundated right now.
I knew all too well what she meant. A few days before our urgent care visit, I had flagged a report for editors at The Hill that said children’s hospitals in the Washington area were at capacity, flooded with young kids suffering from RSV, a potentially life-threatening respiratory illness that has no vaccine.
After a three-hour visit, she gave Ethan a steroid and told us to follow up with his pediatrician the next day.
By the time we got to the pediatrician’s office the following morning, my happy-go-lucky, playful little guy was anything but. He curled up in my lap, as we went through a similar routine that the urgent care doctor had done just the night before. His oxygen levels were too low, and our pediatrician had him do another nebulizer treatment.
“Our goal is to keep you from going to the hospital,” our pediatrician told us.
It seemed like an unusual “goal” from a doctor, but I understood her reasoning. But after Ethan’s oxygen levels dipped lower still after the nebulizer, she said we should rush him straight to the hospital after all.
My “Blue’s Clues” and vehicle-obsessed son, usually the epitome of toddler “I can do it myself!” independence, wouldn’t let me put him down for even a moment as we waited in the emergency room lobby. Surprisingly, a separate waiting area in the ER just for children wasn’t completely full, and I wondered if maybe news reports of endless waits were overblown.
Not so.
“He’s so cute,” a young mother in the waiting room told me, as she motioned to Ethan’s head of curls. She cradled her two-month-old in her arms, patiently rocking the baby after telling me she had waited three hours so far.
I held Ethan as my husband rushed from work to the hospital, meeting us there and with us as we were brought to an ER triage area. They ran more oxygen tests on Ethan, got some of his history, and then sent us back to the waiting room.
Finally, they called Ethan’s name and we were in the ER. My vibrant, otherwise-healthy kid was lethargic, laying on me with a glazed look in his eyes. We struggled to fit the two of us on an exam table meant for a single adult. They draped a lead apron over me and Ethan as they took X-rays of his tiny lungs. The nurse placed a cannula in Ethan’s nose for supplemental oxygen and put an IV in his arm to give him fluids, before wrapping it with a diaper so he wouldn’t try to take out the tube.
My husband and I, loopy from what was happening, laughed at the sight of a diaper being used MacGyver-style. “Hey, it works!” the nurse said, explaining that he’d done the maneuver with kid after kid in recent weeks.
The ER doctor finally came in our room and delivered a crash course in what might be to come. “Everywhere is full. The entire Eastern seaboard,” he said of hospitals.
“We’ve been airlifting kids to Pittsburgh, sometimes to Richmond,” he added. This hospital had a pediatric unit, but not an intensive care geared towards kids. So if Ethan’s condition became even more dire, they wouldn’t be able to treat him there. Our only hope was that the pediatric unit, which had just a few remaining beds, accepted him.
It was a gut punch. As the doctor left, my husband looked at Ethan, who had fallen asleep with a mask on as the nebulizer loudly buzzed away for another treatment.
“He’s just a baby. He’s not supposed to be here,” my husband said, defeated.
The pediatric unit doctor finally came into our room. She examined Ethan, and briefed us on how they’ve been dealing with case after case of the same thing: RSV.
But she offered us hope: he could head to the pediatric unit at the hospital. We wouldn’t need to travel for his care, as long as he didn’t worsen. Ten hours after we first entered the hospital, we had a bed for Ethan.
We’re among the lucky ones. We were told beyond airlifting, plenty of families had been spending multiple nights in the ER because there were no beds.
In Maryland, Gov. Larry Hogan (R) announced last week that that hospitals would receive $25 million in additional funding from the state to prioritize pediatric intensive care unit staffing. Children from birth to age two comprised 57 percent of hospitalizations last week, according to Hogan’s office.
Next to the ghost decorations for Halloween adorning the doors of the pediatric unit, room after room had the same notice taped up: isolation guidelines. The rooms were all filled with kids facing the exact same thing as Ethan. RSV was everywhere.
There’s no cure for RSV. Every two hours on the dot, the nurses would give Ethan the nebulizer treatment.
A monitor affixed to his foot would alert nurses if his oxygen dipped dangerously low, which it did several times throughout the first night. I thought at one point to ask what happens if Ethan stopped responding to the treatments, but then didn’t ask because I didn’t want to know the answer.
The goal was to get him going without the need for additional oxygen, and breathing well for at least four hours between treatments, two times in a row.
That seemingly simple goal proved elusive for two full days. I originally thought it would be a nightmare trying to get a two-year-old to stay in a hospital bed for more than five minutes, but Ethan was in such bad shape that he barely made a fuss. Then, after midnight on our second night in the hospital, Ethan suddenly perked up.
He sat up and rolled over in the hospital bed. Then, he rolled onto my head, spreading his arms and legs out as far as he could stretch, and giggled.
“Should I sleep here?” he said, cracking himself up.
It was like someone hit the power button on my kid, and suddenly he snapped back to himself. I didn’t care that it was midnight and we needed to get some extremely interrupted sleep before the next nebulizer treatment. My son was back.
A nurse later told me that she enjoyed working with kids because for as quickly as their health can deteriorate, they can just as speedily bounce back.
After that, the doctor advised us to try stretching out his time between treatments. Finally, we were told he was stable enough to go home. I somehow hadn’t shed a tear the entire time we were at the hospital, but when the doctor signed off on us leaving, I bawled.
As nightmarish an experience as it was, I realize how incredibly fortunate my family is.
My husband and I have jobs that allowed us to drop everything when our son needed help, we have health insurance policies, and resources to get through spending days at the hospital.
Perhaps most importantly, we had access to an incredible team of doctors and nurses and the sheer fortune of being able to get a bed for our son during an unprecedented and unthinkable time for hospitals.
At the risk of repeating one of those parenting cliches that I would’ve rolled my eyes at a week ago, I’m thankful that I trusted my gut. Even when Ethan was being a wild child at urgent care, I knew something just wasn’t right. What I didn’t know was how much he had been struggling to breathe.
At the hospital after being discharged, Ethan and I waited in the lobby as my husband went to get our car from the parking lot to pick us up. Ethan spotted some empty wheelchairs in the corner of the lobby, and immediately ran over to them. He giggled as he tried to roll one of the chairs into the automatic opening and closing doors. As I looked on as he laughed and laughed at the pint-sized commotion he created, I breathed a sigh of relief.
Americans and global leaders have responded to the May 24 shooting at a Texas elementary school with heartbreak, anger and calls for change to better fight gun violence. But if you’re paying attention, the calls out of healthcare — from trauma surgeons, pediatricians, nurses, leaders and more — carry a distinct type of exasperation and sorrow.
“I’m in one of my hospitals now, sitting with some staff talking about it — it’s just so frustrating,” Michael Dowling, president and CEO of New Hyde Park, N.Y.-based Northwell Health, told me over the phone early Wednesday morning. “This does not represent what the United States stands for — that we allow people who should never be allowed to carry a gun to do so and walk into a school and kill fourth graders.”
The attack by a lone 18-year-old gunman at Robb Elementary School in the small town of Uvalde, Texas, has left at least 19 students and two adults dead. Students in the school, grades 2 through 4, were two days away from summer vacation.
Unlike many other known threats to our health, seeing the medical community condemn mass shootings still seems to leave some Americans doing a double take. It’s increasingly difficult to see what has them confused.
In 2016, the American Medical Association declared gun violence a public health crisis after a lone gunman killed 49 people and wounded 53 more in a mass shooting in a gay nightclub in Orlando, Fla. Even after the declaration, healthcare professionals and leaders continued to defy insistence from gun rights advocates that gun violence was not within their specialty or expertise. Or as the National Rifle Association put it in simpler terms in 2018: “Someone should tell self-important anti-gun doctors to stay in their lane.” The #ThisIsOurLane movement started then. The attempt to silence medical professionals ironically made their calls for action louder.
As healthcare professionals responded to the ongoing public health emergency of COVID-19, the arms race grew and gun buying intensified — “a surge in purchasing unlike anything we’ve ever seen,” as one gun researcher at the University of California, Davis, put it. People who already owned guns bought more, and people who had never owned a gun bought them too. In 2020, firearm-related injuries were the No. 1 cause of death of children and teens, according to the CDC.
Every day, 321 people are shot in the United States, and more than 40,000 Americans die from gun violence each year. Yet some healthcare executives still fear that taking the position that gun violence is a public health crisis will throw them into political turmoil given how toxic politics are in this country. It’s one position for the AMA and its 250,000-plus members to take, but another for an individual leader who may be the face of an organization in their community. There are risks of offending board members, donors, elected officials and other constituents — including patients. But here’s the thing: There will always be a reason to delay, to soften language, to wonder if this mass shooting is the one to react to.
Mr. Dowling urges his colleagues to step it up, noting how hospital and health system leaders can be ambassadors for gun safety in their communities, given the influence they wield as the largest employers in many communities.
“This is about protecting people’s health. This is about protecting kids’ lives. Have some courage. Stand up and do something,” he said. “Put the interest of the community in the center of what you think about each and every day. Our job is to save lives and prevent people from illness and death. Gun violence is not an issue on the outside — it’s a central public health issue for us. Every single hospital leader in the United States should be standing up and screaming about what an abomination this is.
“If you were hesitant about getting involved the day before May 24, May 24 should have changed your perspective. It’s time.”
Northwell established The Gun Violence Prevention Learning Collaborative for Health Systems and Hospitals, a grassroots initiative that gives healthcare professionals the space to have open dialogue about the impact of gun violence, share best practices and collectively take action. Learn more here.
The formal end of the pandemic could swell the ranks of uninsured children by 6 million or more as temporary reforms to Medicaid are lifted.
Why it matters: Gaps in coverage could limit access to needed care and widen health disparities, by hitting lower-income families and children of color the hardest, experts say.
The big picture: A requirement that states keep Medicaid beneficiaries enrolled during the public health emergency in order to get more federal funding is credited with preventing a spike in uninsured adults and kids during the crisis.
Children are the biggest eligibility group in Medicaid, especially in the 12 states that haven’t expanded their Medicaid programs under the Affordable Care Act.
The lifting of the public health emergency, which was just extended to July 15, will lead states to determine whether their Medicaid enrollees are still eligible for coverage — a complicated process that could result in millions of Americans being removed from the program.
That would more than double the number of uninsured kids, which stood at 4.4 million in 2019.
“It is a stark, though we believe conservative, estimate,” said Joan Alker, the center’s executive director. “There are a lot of children on Medicaid.”
Between the lines: Not all of the Medicaid enrollees who are removed from the program would become uninsured. But parents and their children could be headed down different paths if their household income has risen even slightly.
Adults who’ve returned to work may be able to get insurance through their employer. Others could get coverage through the ACA marketplace, though it’s unclear whether that would come the COVID-inspired extra financial assistance that’s now being offered.
Most kids would be headed for the Children’s Health Insurance Program, Alker said — a prospect that can entail added red tape and the payment of premiums or an annual enrollment fee, depending on the state.
What we’re watching: Changes in children’s coverage could be most pronounced in Texas, Florida and Georgia — the biggest non-Medicaid expansion states, which have higher rates of uninsured children than the national average.
Congress could still require continuous Medicaid coverage, the way the House did when it passed the sweeping social policy package that stalled in the Senate over cost concerns.
CMS’ Office of the Actuary projects a smaller decline in Medicaid enrollment than some health policy experts are predicting — and the Biden administration continues to move people deemed ineligible for Medicaid onto ACA plans, Raymond James analyst Chris Meekins noted in a recent report on the unwinding of the public health emergency.
Access to healthcare in childhood has long term effects on health outcomes, but many children in the US are either uninsured or underinsured, meaning they often don’t have access to the care they need. Why is that and what can we do about it?
Healthy individuals who have been vaccinated, and especially those who have been boosted, appear unlikely to develop severe infections from the omicron variant that would land them in the hospital, say medical experts who have monitored the effects of the newest coronavirus variant since it was identified over four weeks ago.
While omicron has sent U.S. infections soaring to levels not seen since last winter’s wave, it appears to have less severe effects than the delta variant, according to a handful of international studies and early data from several U.S. hospitals.
Those infected by the omicron variant are 15 to 20 percent less likely to go to an emergency room, and 40 percent less likely to be hospitalized overnight, compared with those infected with delta, according to English data analyzed by scientists from Imperial College London. That aligns with early U.S. data from some hospitals.
At the Houston Methodist hospital system, about 15 percent of symptomatic individuals have ended up hospitalized — around a 70 percent reduction compared with those infected by the delta variant, said James Musser, chair of pathology and genomic medicine.
A separate study from Britain, which is not yet peer reviewed, found that people infected with omicron were almost 60 percent less likely to enter the hospital than those infected with delta.
“What is absolutely clear is there is lower rate of hospitalization with our omicron patients in our hospital system,” Musser said. “That does not necessarily mean that this variant is quote-unquote ‘less virulent.’ The jury’s still out on that. What we know now is that … if you are immunized and, more importantly, if you are boosted, you’re going to stay out of substantial trouble.”
He and other experts warn against complacency, however, cautioning that millions of Americans, particularly the unvaccinated, remain vulnerable to more serious disease from the most transmissible coronavirus variant to date.
Other factors that might lead to greater risk include an individual’s age, the type of vaccine or booster they received, and whether they have underlying health problems, such as heart disease or obesity, said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota and a member of President Biden’s covid-19 transition task force.
“Have you previously had infection? Were you vaccinated? How many doses of vaccine, and was it more than six months ago? So in some ways this is almost like a calculus problem. It’s got a lot of moving parts to it and we’re trying to figure it out,” Osterholm said.
Doctors also caution that far more people will become infected with omicron simply because of its transmissibility. If even a small fraction of those land in the hospital, they worry that health care systems that are already short-staffed because of delta infections could be overwhelmed — with potentially dire results for those needing critical care as a result of car accidents, heart attacks, strokes, or any number of things that bring people to emergency rooms.
“We need to be respectful of the fact that our hospital system has been under this kind of duress for such a long time,” said Larry Corey, a virologist at the Fred Hutchinson Cancer Research Center in Seattle. “We need to do everything we can to not allow the situation, where there’s such crowding and such intensity that we can’t optimally take care of the people who get severe disease.”
Anthony S. Fauci, Biden’s chief medical adviser, said the rapid increase in the numbers of people getting infected with the omicron variant will invariably put additional strain on the system.
“We’re going to have a real challenge to the health-care delivery system — namely the number of beds, the number of ICU beds and even the number of health care providers,” Fauci said in an interview. “Even vaccinated people are getting breakthrough infections. So if you get enough nurses and doctors infected, they are going to temporarily be out of action. And if you get enough of them out of action, you could have a double stress on the health care system.”
The welcome news for most people who are vaccinated and boosted is that omicron infections often mimic the symptoms of the common cold. Those with two shots of vaccine, but no booster, also appear to fare relatively well, though they may develop more intense symptoms that may last longer, experts said.
In a series of Twitter posts, Craig Spencer, who teaches emergency medicine at Columbia University Medical Center, said every boosted patient he has seen in the emergency room has had no difficulty breathing or shortness of breath. Those who have had two doses of either the Pfizer or Moderna vaccines also have had mild symptoms, he said, “but more than those who had received a third dose.”
But almost every patient who had to be hospitalized was unvaccinated, he said.
“No matter your political affiliation, or thoughts on masks, or where you live in this country, as an ER doctor you’d trust with your life if you rolled into my emergency room at 3am, I promise you that you’d rather face the oncoming Omicron wave vaccinated,” Spencer wrote.
Children are also filling up hospital beds in many parts of the country, especially in New York. State officials issued a warning on Christmas Eve after a fourfold increase in hospitalizations in children under 18 in New York City between Dec. 5 and last week. About half of the admissions were children under 5, who are not eligible for vaccination, according to the New York Department of Health.
Experts cautioned that those at higher risk of severe infection to previous variants probably remain vulnerable to this one.
It’s not yet clear whether older, boosted individuals and those with underlying conditions, such as diabetes and heart disease, face the same lowered risk with omicron. Answering such questions is key to assessing the likely trajectory of the variant in the U.S. since it is older and less healthy than many of its global peers.
So far, though, early U.S. data echoes what has been seen in South Africa and Britain, where omicron waves are slightly ahead of this country’s.
A group of Scottish scientists said recently that vaccinated people appear to have some protection against symptomatic infection from omicron, although less than they did against delta. A third dose or booster of an mRNA vaccine was associated with a 57 percent reduction in the odds of developing a symptomatic omicron case.
In the Johns Hopkins Hospital emergency department, physicians are seeing more infections than atany other point in the pandemic, but most of the cases are not severe, said Stuart Ray, a professor of medicine in the division of infectious diseases. But he warned that there is not yet “reassuring evidence” the United States will be spared from a disruptive wave of infections and complications.
The country faces other challenges with omicron in terms of its medicine cabinet. Two of the three existing intravenous treatments called monoclonal antibodies — those from Regeneron and Eli Lilly — do not work against the variant. Some Republican governors had touted the ability of those with covid-19 to receive monoclonal antibodies, spurring some Americans to see those treatments as an alternative to getting vaccinated.
The only monoclonal antibody that does work, sotrovimab from Vir Biotechnology and GlaxoSmithKline, is in short supply and will not be available to many of those who become infected. The Food and Drug Administration authorized two easy-to-take antiviral pills last week and one has high efficacy against omicron, but it will be in initial short supply. Distribution of the pills is expected to begin shortly.
It is also unclear whether the surge in the United States will follow the same pattern as South Africa’s, which rapidly passed the peak of omicron cases last week.
South Africa’s population is significantly younger and has far lower vaccination rates, with about 35 percent of the population immunized, and virtually no oneboosted.The country also grappled with a delta variant wave that infected a far greater portion of the population than it did in the United States.
The significant number of South African residents infected with delta compared with the United States could prove to be an important distinction that might make more Americans vulnerable to omicron, said Chris Beyrer, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health.
Beyrer also noted that infections in the United States, Britain and Germany seemed to be increasing at a significantly faster rate than they were in South Africa.
“This is an incredibly infectious virus and it is moving right along,” Beyrer said. He added that the United States has numerous tools — including ready access to vaccines and booster shots, the new antiviral medicines, testing and masking — that could help curb its effects.
But referring to those who have refused to follow public health guidelines, Beyrer said, “We have a lot of resistance so that makes us vulnerable to infection.”
The number of children with covid-19 recently hospitalized in New York City has increased by nearly five times this month, state officials said at a news conference Monday.
For the week from Dec. 5, 22 children with covid-19 were admitted to hospitals in the city. During a five-day period beginning on Dec. 19, that figure rose to 109, reflecting a broader national surge in coronavirus infections driven in part by the omicron variant. Daily case counts in recent days have climbed to levels not seen since last winter, when coronavirus vaccines weren’t widely available, though the total number of hospitalizations is still significantly lower.
The increase in pediatric covid patients in New York City has been mirrored nationwide. As of last week, nearly 2,000 confirmed or suspected pediatric covid patients were hospitalized nationally, a 31 percent jump in 10 days.
New York City officials are hoping a city mandate that took effect Monday requiring workers at an estimated 184,000 businesses to get at least one vaccine dose will curb infections. “We need more and more people vaccinated,” Mayor Bill de Blasio (D) told reporters. “We need to keep doubling down on vaccination to get out of the covid era once and for all.”
De Blasio’s office announced the mandate earlier this month, just days after health officials disclosed the first case of the more transmissible omicron variant in the United States. But the mayor leaves office in a few days. Kathryn Wylde, president of the Partnership for New York City, a major corporate advocacy group, said she hopes Mayor-elect Eric Adams (D) will show flexibility in enforcement, the Associated Press reported.
Roughly 92 percent of the city’s adult population has received at least one dose of a vaccine, municipal data show, while 83 percent of adults are considered fully immunized. Youth vaccination rates remain lower: Nearly half the children ages 5 to 17 have not yet received a single dose, according to the city government.
A first COVID shot will give kids some protection, but none of them will be fully vaccinated until the beginning of December.
For many, many months now, 7-year-old Alain Bell has been keeping a very ambitious list of the things he wants to do after he gets his COVID-19 shots: travel (to Disneyworld or Australia, ideally); play more competitive basketball; go to “any restaurants that have french fries, which are my favorite food,” he told me over the phone.
These are very good kid goals, and they are, at last, in sight. On Tuesday evening, about as early as anyone in the general public could, Alain nabbed his first dose of Pfizer’s newly cleared pediatric COVID-19 vaccine. The needle delivered “a little poke,” he said, but also a huge injection of excitement and relief. Since his father, a critical-care physician, was vaccinated last December (the first time I interviewed Alain), “I’ve been impatient,” Alain said. “I really wanted to get mine.” Now he is finally on his way to joining the adults. When he heard on Tuesday that his shot was imminent, he let out a scream of joy, at “a pitch I have never heard him use before,” his mother, Kristen, told me.
There’s an air of cheer among the grown-ups as well. “It’s cause for celebration,” says Angie Kell, who lives in Utah with her spouse and their soon-to-be-vaccinated 6-year-old son, Beck. Their family, like many others, has been reining in their behavior for months to accommodate their still-vulnerable kid, unable to enjoy the full docket of post-inoculation liberties that so many have. Once Beck is vaccinated, though, they can leave mixed-immunity limbo: “We might have an opportunity to live our lives,” Kell told me.
The past year has been trying for young children, a massive test of patience—not always a kid’s strongest skill. And there’s yet another immediate hurdle to clear: the plodding accumulation of immunological defense. Alain has another 15 days to go until his second dose; after that, it’ll be two more weeks before he reaches a truly excellent level of protection. Only then, on December 7, will he count as fully vaccinatedby CDC standards and be able to start adopting the behavioral changes the agency has green-lit. In the intervening weeks, he and the many other 5-to-11-year-olds in his position will remain in a holding pattern. Their wait isn’t over yet.
The timing of this semi-immune stretch might feel particularly frustrating, especially with the winter holidays approaching: At this point, essentially no young kids are slated to be fully vaccinated by Thanksgiving or Hanukkah, except the ones who were enrolled in clinical trials. One shot can offer a level of protection, but experts advise waiting to change behavior for a reason—the extra safeguards that set in about two weeks after the second shot really are that much better, and absolutely worth sitting tight for.
“It takes time for immune cells to get into a position where they’re ready to pounce,” Gigi Gronvall, a senior scholar at the Johns Hopkins Center for Health Security, told me. COVID-19 vaccines teach immune cells to thwart the coronavirus, a process that, like most good boot camps, takes many days to unfold. The second shot is essential to clinch the lesson in the body’s memory, encouraging cells to take the threat more seriously for longer. Immune cells also improve upon themselves over time—the more, the better in these early stages. Gronvall’s own 11-year-old son is also about to get his first shot, and she doesn’t want to risk stumbling so close to the finish line. “I can’t know exactly what his immune system is going to do” after the first dose alone, she said.
Evidence from Pfizer’s original clinical trial, conducted only in adults, hinted that a first, decent defensive bump takes hold after the first shot. Kit Longley, Pfizer’s senior manager of science media relations, pointed to those data when I asked how kids at various points along the vaccination timeline should be approaching behavioral change. “Protection in the vaccinated cohort begins to separate from the placebo arm as early as 12 to 14 days after the first dose,” he told me.
The adult clinical-trial data were collected last year, though, long before the rise of the Delta variant. A more recent study, conducted in the United Kingdom, showed that one dose of Pfizer reduced the risk of symptomatic COVID-19 by only 35.6 percent when the cause was Delta, and by only 47.5 percent with Alpha. (And remember that those numbers apply best on a population scale—not for a single, individual child.) After adding a second dose, though, effectiveness rocketed up to about 90 or 95 percent against either variant. “You really need two doses for adequate, good protection,” Samuel Dominguez, a pediatric-infectious-disease specialist at Children’s Hospital Colorado, told me.
Immunity is so far looking strong in young kids: In a recent trial of thousands of children ages 5 to 11, Pfizer’s vaccine was more than 90 percent effective at blocking symptomatic cases of COVID-19, including ones caused by Delta. Longley said Pfizer expects that the timing of protection will be similar between children and adults—a first dose should lower everyone’s risk to some degree. But the company’s pediatric trial picked up only a few COVID-19 cases; none of them occurred until about three weeks after the first dose was given, or later. So it’s hard to say anything definitive about when “enough” immunity really kicks in for kids.
Some parents are counting on a level of early protection from one shot, including my cousin Joanne Sy, whose 8-year-old son, Jonah, received his first injection on Friday. “He will have good immunity after one dose,” she told me, hopefully enough to guard him on a trip they’re taking to New York for Thanksgiving two weeks from now. “We’re still going to be cautious,” Sy told me: They’ll be watching the Macy’s Thanksgiving Day Parade from a hotel room rather than the streets, and wearing masks, at least on the plane. “But we just need to move forward.”
The calculus is playing out differently for Christy Robinson of Arlington, Virginia, who will again be “hunkering down” with her husband and two daughters, June and Iris, 7 and 5, respectively, this Thanksgiving. The kids got their first Pfizer shot on Saturday, setting their household up for full, full vaccination by mid-December, just in time to hold an indoor gathering with their aunts, uncles, and cousins for Christmas. (Some quick arithmetic: To be fully vaccinated by December 25, a kid would need their first dose by November 20.) June’s also eager to “see my friends inside, because it’s cold outside,” she told me—plus go to movie theaters, and Build-A-Bear, and a trampoline park, and IHOP, and the nail salon.
By the end of this conversation, Robinson looked amused and maybe a little regretful that my question had prompted such an extravagant list. As their mother, she’s especially excited for the possibility of no longer having to quarantine her daughters after viral exposures at school. Heftier decisions are ahead too. She and her husband are still weighing whether to bring their daughters into closer, more frequent indoor contact with their grandparents, who are vaccinated but could still get seriously sick if someone ferries the virus into their midst.
And that risk—of transmitting the virus—is worth keeping in mind, with so much SARS-CoV-2 “still circulating around,” cautions Tina Tan, a pediatrician and infectious-disease specialist at Northwestern University. Immunized people are at much lower risk of picking up the virus and passing it on. There still aren’t enough of them, though, to reliably tamp down spread; uptake of shots among young kids, too, is expected to be sluggish in the months to come. Even fully vaccinated families won’t be totally in the clear while our collective defenses remain weak.
That doesn’t mean Thanksgiving has to be a bust—or even a repeat of 2020, before the vaccines rolled out. The Bells will be cautiously gathering with a few loved ones; all the adults in attendance will be immunized and everyone will get tested beforehand. “Then they can come inside the house, mask off,” Taison Bell, Alain’s father, told me. None of those measures is completely reliable on its own; together, though, they’ll hopefully keep the virus out.
The road ahead might feel a little bumpy for Alain, who’s celebrating his 8th birthday at the end of November, a few days after his second shot. (He’s getting the gift of immunity this year, his father joked.) The Bells will do something special “around when he hits full vaccination,” Kristen said, “with something Alain hasn’t gotten to do in the last two years.” But Alain, who has asthma, which can make COVID-19 worse, knows that his own injections won’t wipe the slate clean for him, or those around him. Some people in his neighborhood have caught the virus even after getting vaccinated, and he understands that he could too.
Alain will keep masking, and treading carefully at school, and even a bit at home. His 3-year-old sister, Ruby, hasn’t yet been able to get a shot. (I asked her how she felt about Alain’s vaccine; she responded, almost imperceptibly, “Jealous.”) Until another regulatory green light comes, she will still be waiting, which means that her family will be too.
Pfizer’s COVID-19 vaccine is nearly 91 percent effective at preventing symptomatic infections in children between ages 5 and 11, according to a study released by the FDA Oct. 22.
The study involved 2,268 children given COVID-19 vaccines that are one-third the dosage of the vaccines given to people ages 12 and up. They were given two doses spaced three weeks apart, the same as the adult version of the vaccine. It found that the children developed antibody levels just as strong as older children and adults given the full dosage.
The FDA’s Vaccines and Related Biological Products Advisory Committee is set to meet Oct. 26 to discuss the evidence and vote on whether to recommend FDA authorization for the shots in kids ages 5 to 11.
The CDC’s vaccine advisory panel is set to meet the first week of November to discuss recommending the shots for the age group. That means shots for kids ages 5 to 11 could be authorized in the first week of November. There are about 28 million children in the age group in the U.S.
The vaccines will come in orange capped vials to make them easily distinguishable from adult doses, according toABC News.
As a long hoped-for sign of the “return to normal”, most children went back to in-person learning this fall. And with the patchwork of COVID safety protocols and masking policies across school districts, classrooms became a learning lab for scientists studying the efficacy of masking and other precautions.
Unsurprisingly, getting a bunch of unvaccinated kids back together caused a surge in pediatric COVID cases. But recent Centers for Disease Control and Prevention (CDC)data from 500 counties demonstrate just how effective mask mandates have been at mitigating outbreaks.
The graphic above shows that cases in counties without school mask mandates increased at nearly three times the rate of those with mask mandates. In the five-week period spanning the start of the school year, cases in counties without a mask mandate rose by 62.6 cases per 100K children, while cases in counties with a mask mandate rose by only 23.8 per 100K. COVID outbreaks are incredibly disruptive to learning; according to a recent KFF survey, nearly a quarter of parents report their child has already had to quarantine at home this school year following a possible COVID exposure.
Even once vaccines are approved for children under 12, recent data suggest that a majority of parents will be hesitant to vaccinate their child. Just over half of 12- to 17-year-olds have received at least one dose of the vaccine so far, and only a third of parents of 5- to 11-year-olds plan to vaccinate their child right away, once the shot is approved.
Many want more information, or are worried about side effects—concerns that will best be assuaged by their pediatricians and other trusted sources of unbiased information.