The new year is always an ideal time for healthcare leaders to reflect on the state of our industry and their own organizations, as well as the challenges and opportunities ahead.
As the CEO of a large health system, I always like to reflect on one basic question at the end of each year: Are we staying true to our mission?
Certainly, maintaining an organization’s financial health must always be a priority but we should also never lose sight of our core purpose. In a business like ours that has confronted and endured a global pandemic and immense financial struggles over the past several years, I recognize it’s increasingly difficult to maintain our focus on mission while trying to find ways to pay for rising labor and supply costs, infrastructure improvements needed to remain competitive and other pressures on our day-to-day operations.
After all, the investments we need to make to promote community wellness, mental health, environmental sustainability and health equity receive little or no reimbursement, negatively impacting our financial bottom lines. During an era of unprecedented expansion of Medicaid and Medicare, we get less and less relief from commercial insurers, whose denial and delay tactics for reimbursing medical claims continue to erode the stability of many health systems and hospitals, especially those caring for low-income communities.
Despite those enormous pressures, it’s imperative that we continue to support underserved communities, military veterans struggling with post-traumatic stress, and intervention programs that help deter gun violence and addiction.
The list of other worthy investments goes on and on: charity care to uninsured or underinsured patients who can’t pay their medical bills, funding for emergency services that play such a critical role during public health emergencies, nutritional services for families struggling to put food on the table, programs that combat human trafficking and support women’s health, the LGBTQIA+ community and global health initiatives that aid Ukraine, the Middle East and other countries torn apart by war, famine and natural disasters.
We must also recognize the key role of healthcare providers as educators. School-based mental health programs are saving lives by identifying children exhibiting suicidal behaviors, anger management issues and other troublesome behaviors. School outreach efforts have the added benefit of helping health systems and hospitals address their own labor shortages by introducing young people to career paths that will help shape the future healthcare workforce.
Without a doubt, the “to-do” list of community health initiatives that support our mission is daunting. We can’t do it all alone, but as the largest employers in cities and towns across America, health systems and hospitals can serve as a catalyst to get all sectors of our society — government, businesses, schools, law enforcement, churches, social service groups and other community-based organizations — to recognize that “health” goes far beyond the delivery of medical care.
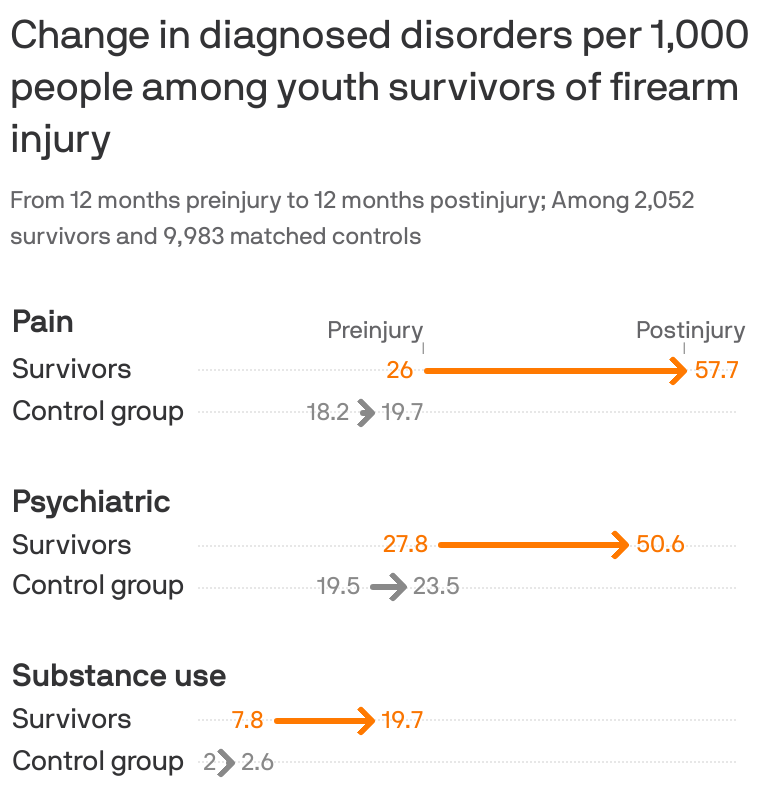
The health of individuals, families and communities hinges on the prevalence of good-paying jobs, decent and affordable housing, quality education, access to healthy foods, medical care, transportation, clean air and water, low prevalence of crime and illicit drugs, and numerous other variables that typically depend on the zip codes where we live. Those so-called social determinants of health are the driving factors that enable communities and the people who live there to either prosper or struggle, resulting in disparities that are the underlying cause of why so many cities and towns across the country fall into economic decay and become havens for crime and hotbeds for gun violence, which shamefully is now the leading cause of death for children and adolescents.
To revive these underserved communities, many of which are in our own backyards, we have to look at all of the socioeconomic issues they struggle with through the prism of health and use the collective resources of all stakeholders to bring about positive change.
Health is how we work together to build a sense of community. Having a healthy community also requires everyone doing what they can to tone down the political rhetoric and social media-fueled anger that is polarizing our society. Health is bringing back a sense of civility and respect in our public discourse, and promoting the values of honesty, decency and integrity.
As healthcare providers and respected business leaders, we should all make a New Year’s resolution to stay true to our mission and do what we can within our communities to bring oxygen to hope, optimism and a healthier future.