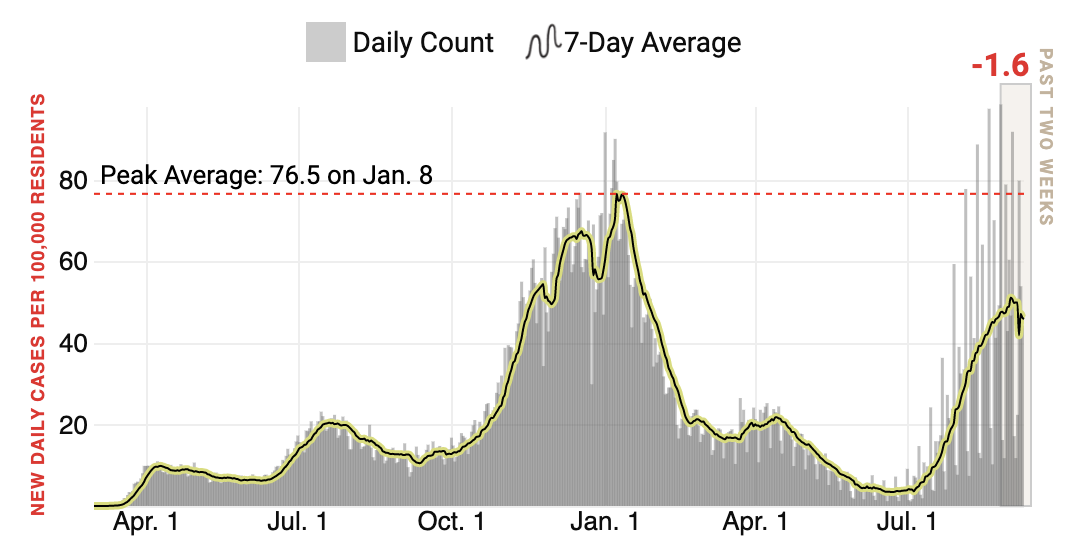
It may feel like eons ago, but try to recall summer 2020: While there were coronavirus surges in some parts of the country, national case rates were low. In some areas, the virus almost faded away entirely. But of course, the respite didn’t last. Cases began rising again in the fall of 2020, peaking at an average of more than 250,000 per day in January 2021.
The U.S. may be in for something even worse this year, my colleague Chris Wilson warns.
After a heartbreakingly bad summer, the virus’ spread appears to be ebbing, Chris writes. As of today, the U.S. is reporting about 145,000 diagnoses per day—too high for comfort, but at least a modest downward trend from over 160,000 daily cases at the end of August. In many hotspot states, diagnoses are significantly lower than they were a month or two ago.
But kids are now returning to school, cooler weather will force social gatherings indoors and holiday travel season will soon be upon us. With the highly contagious Delta variant now the dominant strain and millions of Americans still unvaccinated, we may be heading for a repeat of last year.
Of course, the situation isn’t exactly the same. More than half the population (and counting) is fully vaccinated, and many other people have at least some level of natural immunity after surviving an infection. That will certainly help keep cases down, but it may not be enough. As Chris points out, seven U.S. states set new daily case records this summer, even with vaccines widely available. As long as there are millions of unvaccinated people in the U.S., the virus will find a way to spread—particularly when it’s as contagious as the Delta variant.
So what can you do? At the risk of sounding like a broken record, the advice is the same as ever: get vaccinated if you haven’t, get your kids vaccinated if they’re old enough, wear masks if you gather with people indoors and stay home if you feel unwell.
President Joe Biden’s announcement Thursday that broadly expanded mandatory COVID-19 vaccinations or at least compulsory weekly testing is a sign, possibly, that the administration sees the writing on the wall. Even with tentative but promising signs that the fourth wave of surging cases in COVID-19 in the United States, dating back to the first days of summer, was waning, without drastic measures, the fifth will be catastrophically worse.
The new requirements are estimated to affect about 100 million people, including most federal workers and a substantial number of private sector employees—many of whom are already vaccinated. This would largely affect working-age residents (age 18-64), who currently number above 200 million, of whom 59.8% are vaccinated, according to TIME’s analysis of daily figures from the U.S. Centers for Disease Control and Prevention. That leaves more than 80 million who remain unvaccinated, though the White House orders will only cover a fraction of them.
The question is now: What happens this fall and winter, when children are at school and Americans once again travel for the holidays? In spite of desperate warnings from the CDC that people stay home for last year’s holiday, they largely did not, which led to the third spike in cases, which reached heights that dwarfed the first two. That doesn’t bode well for Christmas 2021, especially given that, in this current, fourth wave, seven states have already surpassed their previous peaks in cases (with another four doing nearly as poorly):
Within the next several days, we may see a modest surge from travel over the Labor Day weekend, but the real test willcome in about two months—still all too soon. The holidays always sneak up on us. Under one possibility, many millions of Americans may be bolstered by a booster shot of the COVID-19 vaccine, though this will be scant protection for those who have yet to receive a first.
Evidence that surging cases could inspire more unvaccinated Americans to change their mind was initially encouraging, but did not extend indefinitely. Should the fourth wave recede considerably, it may take a fifth to convince a significantly greater number.
Declaring that “our patience is wearing thin” with Americans who refuse to be vaccinated against COVID-19, President Biden announced sweeping new plans to implement vaccine mandates on Thursday.
Businesses that employ more than 100 people must require their employees to get vaccinated or face weekly COVID testing, federal workers and contractors must be vaccinated or face disciplinary measures, and all healthcare organizations that receive Medicare or Medicaid funds must ensure 100 percent employee vaccination as a condition of continued participation in those federal payment programs. The healthcare component of the mandate will impact about 17 million workers, including those at hospitals, surgery centers, dialysis facilities, and home health agencies. The Centers for Medicare & Medicaid Services (CMS) already requires nursing home workers to be vaccinated, and yesterday announced plans to release a new regulation by October 1st, implementing the expanded mandate. According to Fierce Healthcare, at least 172 hospital systems have already announced some form of vaccine mandate, but others have expressed concerns that forcing workers to get vaccinated might exacerbate labor shortages and result in employees seeking work elsewhere.
Responding to President Biden’s announcement, the American Hospital Association (AHA) echoed those concerns, citing “the critical challenges that we are facing in maintaining the resiliency of our workforce.” In our view, that concern pales in comparison to the imperative to protect patients by reducing the potential for exposure by unvaccinated caregivers. If anything, the national healthcare mandate should provide cover for those hospitals and care providers that have shied away from mandates, letting other organizations take the lead. Once universal healthcare mandates are implemented, vaccine resistant workers will find few employment alternatives left, significantly dampening the risk of widespread resignations. If you don’t want to take the necessary precautions to keep patients safe, you shouldn’t be working in healthcare in the first place. Yesterday’s mandate announcement, while aggressive, is overdue.
For much of August, the U.S. South showed up fire-engine red on our map of COVID-19’s spread in the U.S., meaning case counts were shooting up. But now, Florida, Louisiana, Mississippi, Arkansas and Missouri show up in shades of green, meaning cases—while still high—are trending down.
Does that mean the Delta surge is nearing its end?
If covering the pandemic for 18 months has taught me anything, it’s that confident predictions often come back to bite you. But there is reason for cautious optimism. Past U.S. surges have played out in short, intense bursts, and some experts have predicted, based on Delta’s behavior in other countries, that U.S. infections could peak in late August or early September. Covidestim, a modeling project from researchers at Yale, Harvard and Stanford, points to another promising sign: In more than half of states, a person infected with COVID-19 would currently be expected to transmit the virus to less than one other person, in what is perhaps a sign of waning community transmission and/or better population immunity.
Still, we shouldn’t get ahead of ourselves. The U.S. is recording an average of about 150,000 new diagnoses per day, a number not seen since this past winter’s pre-vaccination spike. And in many states, like South Dakota and West Virginia, the trends are going in the wrong direction—and fast. That suggests Delta may be moving to new states, rather than fading away completely.
The situation may become even messier as the school year gets underway. Far more kids have gotten seriously ill during this wave compared to previous ones, in part because of Delta’s contagiousness and in part because children younger than 12 cannot be vaccinated, whereas older Americans are better protected from infection. In a worst-case scenario, pediatric ICUs nationwide may be heading for a repeat of what the South has seen this summer.
While the virus behaves in mysterious ways, people in the U.S. are not powerless. The Delta variant is indeed extra contagious, but the summer surge also coincided with relaxed mask guidelines and, for many people, a return to indoor activities. In South Dakota, one of the states currently seeing the largest increases in cases, the spike seems to be related to large-scale gatherings at the Sturgis Motorcycle Rally. That suggests our behavior matters just as much as the virus’. Getting vaccinated, wearing masks indoors and avoiding large crowds can all help the Delta surge come to an end.
TODAY’S CORONAVIRUS OUTLOOK
About 445.6 million doses of the COVID-19 vaccine have been shipped to various U.S. states as of this afternoon, of which some 372.1 million doses have been administered thus far, according to TIME’s vaccine tracker. About 52.7% of Americans have been completely vaccinated.
More than 219 million people around the world had been diagnosed with COVID-19 as of this afternoon, and more than 4.5 million people have died. On September 2, there were 631,605 new cases globally.
Here’s how the world as a whole is currently trending:
Here’s where daily cases have risen or fallen over the last 14 days, shown in confirmed cases per 100,000 residents:
And here’s every country that has reported over 4 million cases:
The U.S. had recorded more than 39.5 million coronavirus cases as of this afternoon. More than 643,000 people have died. On September 2, there were 153,143 new cases and 1,588 new deaths confirmed in the U.S.
Here’s how the country as a whole is currently trending:
Here’s where daily cases have risen or fallen over the last 14 days, shown in confirmed cases per 100,000 residents:
All numbers unless otherwise specified are from the Johns Hopkins University Center for Systems Science and Engineering, and are accurate as of Sept. 3 1 a.m. E.T. To see larger, interactive versions of these maps and charts, click here.
WHAT ELSE YOU SHOULD KNOW
The U.S. economy gained only 235,000 jobs in August, according to new data from the U.S. Bureau of Labor Statistics—far below this year’s average of 586,000 per month and economists’ expectations of more than 700,000 in August. The retail and dining sectors lost jobs in August, which suggests the Delta-related surge is again putting the squeeze on customer-facing businesses.
South Africa will no longer export Johnson & Johnson vaccines to Europe, under a deal struck by leaders from South Africa, France and the European Commission. The shots will instead be distributed among people on the African continent, where only about 3% of the population is fully vaccinated against COVID-19, compared to nearly 60% in the European Union. The European Commission will also return shots already shipped to Europe from South Africa to help aid the continent’s vaccination campaign, CNN reports.
The U.S. government will invest $3 billion in the vaccine supply chain, in an effort to help manufacturers churn out more shots and supplies for both the U.S. and the rest of the world. Federal officials have not publicly announced which companies will receive that money, but White House COVID-19 adviser Jeff Zients said yesterday that funding will be channeled toward firms that make materials needed for vaccine production and administration, as well as facilities that fill vaccine vials and those that make personal protective equipment.
Employers and private businesses around the world have begun to mandate COVID-19 vaccination. Now, Italian officials are mulling a population-wide vaccine requirement for anyone old enough to receive a shot, according to Reuters. Such a policy wouldn’t happen until the European Medicines Agency gives the shots full approval, but it would still likely be unpopular in a country with a significant vaccine-hesitant population. At present, about 70% of Italians 12 and older are fully vaccinated.
On the other end of the spectrum, U.K. regulators reportedly may not recommend vaccines for healthy children ages 12 to 15. While shots are recommended for children with underlying conditions that put them at risk of severe disease, U.K. authorities are still assessing whether immunization is necessary for healthy kids, given their relatively low risk of hospitalization or death. The country’s regulators are, however, analyzing whether universal pediatric vaccination may be necessary to maintain safe schools.
Dr. Anthony Fauci, the top U.S. expert on COVID-19, added to the back-and-forth on booster shots yesterday, noting that a three-shot regimen will probably become standard for COVID-19 vaccines. He said a three-dose system would likely ensure more “durable” protection against the virus than a two-shot schedule, CNN reports. Ultimately, though, that decision isn’t up to Fauci. It will be decided by regulators at the U.S. Food and Drug Administration, who are set to discuss booster shots at a meeting later this month.
Many people are seeking definitive answers about what they can and can’t do after being vaccinated against Covid-19. Is it OK to travel? Should I go to a big wedding? Does the Delta variant make spending time with my vaccinated grandmother more risky?
But there’s no one-size-fits-all answer to those questions because risk changes from one individual to the next, depending on a person’s overall health, where they live and those they spend time with.
The bottom line is that vaccines are highly protective against serious illness, and, with some precautions, will allow people to return to more normal lives, experts say.A recent study in Los Angeles County showed that while breakthrough infections can happen, the unvaccinated are 29 times as likely to end up hospitalized from Covid-19 as a vaccinated person.
Experts say anxiety about breakthrough infections remains pervasive, fueled in part by frightening headlines and unrealistic expectations about the role of vaccines.
“There’s been a lot of miscommunication about what the risks really are to vaccinated people, and how vaccinated people should be thinking about their lives,” said Dr. Ashish K. Jha, dean of the Brown University School of Public Health. “There are people who think we are back to square one, but we are in a much, much better place.”
While the Delta variant is causing a surge in infections in various hot spots around the country, including Florida and Louisiana, there will eventually be an end to the pandemic. Getting there will require ongoing precautions in the coming months, but vaccinated people will have more freedom to enjoy life than they did during the early lockdowns. Here are answers to some common questions about the road ahead.
What’s my risk of getting Covid if I’m vaccinated?
To understand why there is no simple answer to this question, think about another common risk: driving in a snowstorm. While we know that tens of thousands of people are injured or killed each year on icy roads, your individual risk depends on local conditions, the speed at which you travel, whether you’re wearing a seatbelt, the safety features on your car and whether you encounter a reckless driver on the road.
Your individual risk for Covid after vaccination also depends on local conditions, your overall health, the precautions you take and how often you are exposed to unvaccinated people who could be infected.
“People want to be told what to do — is it safe if I do this?” said Dr. Sharon Balter, director of the division of communicable disease control and prevention at the Los Angeles County Department of Public Health. “What we can say is, ‘These are the things that are more risky, and these are the things that are less risky.’”
Dr. Balter’s team has recently collected surveillance data that give us a clearer picture of the difference in risk to the vaccinated and unvaccinated as the Delta variant surged from May 1 through July 25. They studied infections in 10,895 fully vaccinated people and 30,801 unvaccinated people.The data showed that:
The rate of infection in unvaccinated people is five times the rate of infection in vaccinated people. By the end of the study period, the age-adjusted incidence of Covid-19 among unvaccinated persons was 315.1 per 100,000 people over a seven-day period compared to 63.8 per 100,000 incidence rate among fully vaccinated people. (Age adjustment is a statistical method used so the data are representative of the general population.)
The rate of hospitalization among the vaccinated was 1 per 100,000 people. The age-adjusted hospitalization rate in unvaccinated persons was 29.4 per 100,000.
Older vaccinated people were most vulnerable to serious illness after a breakthrough infection. The median age of vaccinated people who were hospitalized for Covid was 64 years. Among unvaccinated people who were hospitalized, the median age was 49.
The Delta variant appears to have increased the risk of breakthrough infections to vaccinated people. At the start of the study, before Delta was dominant, unvaccinated people became infected 10 times as often as vaccinated people did. By the end of study period, when Delta accounted for almost 90 percent of infections, unvaccinated people were five times as likely to get infected as vaccinated people.
What’s the chance of a vaccinated person spreading Covid-19?
While unvaccinated people are by far at highest risk for catching and spreading Covid-19, it’s also possible for a vaccinated person to become infected and transmit the illness to others. A recent outbreak in Provincetown, Mass., where thousands of people gathered in bars and restaurants, showed that vaccinated people can sometimes spread the virus.
Editors’ Picks
Even so, many experts believe the risk of getting infected from a vaccinated person is still relatively low. Dr. Jha noted that after an outbreak among vaccinated and unvaccinated workers at the Singapore airport, tracking studies suggested that most of the spread by vaccinated people happened when they had symptoms.
“When we’ve seen outbreaks, like those among the Yankees earlier in the year and other cases, almost always people are symptomatic when they’re spreading,” Dr. Jha said. “The asymptomatic, pre-symptomatic spread could happen, but we haven’t seen it among vaccinated people with any frequency.”
Another study from Singapore looked at vaccinated and unvaccinated people infected with the Delta variant. The researchers found that while viral loads in vaccinated and unvaccinated workers are similar at the onset of illness, the amount of virus declines more rapidly in the vaccinated after the first week, suggesting vaccinated people are infectious for a shorter period of time.
Is it still safe to gather unmasked with vaccinated people?
In many cases it will be safe, but the answer depends on a number of variables. The risk is lower with a few close family members and friends than a large group of people you don’t know. Outdoor gatherings are safer than indoor gatherings. What’s the community transmission rate? What’s the ventilation in the room? Do you have underlying health issues that would make you vulnerable to complications from Covid-19? Do any of the vaccinated people have a fever, sniffles or a cough?
“The big question is can five people sit around a table unmasked if we know they’re all vaccinated,” Dr. Jha said. “I think the answer is yes. The chances of anybody spreading the virus in that context is exceedingly low. And if someone does spread the virus, the other people are not going to get super sick from it. I certainly think most of us should not fear breakthrough infections to the point where we won’t tolerate doing things we really value in life.”
For larger gatherings or even small gatherings with a highly vulnerable person, rapid antigen testing using home testing kits can lower risk. Asking people to use a test a few days before the event, and then the day of the event, adds another layer of protection. Opening windows and doors or adding a HEPA air cleaner can also help.
How can unvaccinated children go to school safely?
Children under 12 probably will not be eligible for vaccination until the end of the year. As a result, the best way to protect them is to make sure all the adults and older kids around them are vaccinated.A recent report from the C.D.C. found that an unvaccinated elementary schoolteacher who didn’t wear a mask spread the virus to half of the students in a classroom.
Studies show that schools have not been a major cause of Covid-spreading events, particularly when a number of prevention measures are in place. A combination of precautions — masking indoors, keeping students at least three feet apart in classrooms, keeping students in separate cohorts or “pods,” encouraging hand washing and regular testing, and quarantining — have been effective. While many of those studies occurred before the Delta variant became dominant, they also happened when most teachers, staff and parents were unvaccinated, so public health experts are hopeful that the same precautions will work well this fall.
Dr. Balter noted that masking in schools, regular testing and improving ventilation will keep children safer, and that parents should be reassured by the data.
“The level of illness in children is much less than adults,” she said. “You do weigh all these things, but there are also a lot of consequences to not sending children to school.”
Can a vaccinated person visit with an elderly vaccinated person indoors without a mask?
In many cases it will be relatively safe for vaccinated people to spend time, unmasked, with an older relative. But the risk depends on local conditions and the precautions the visitor has taken in the days leading up to the visit. In areas where community vaccination rates are low and overall infection rates are high, meeting outdoors or wearing a mask may be advised.
If you’re vaccinated but have been going to restaurants, large gatherings or spending time with unvaccinated people, it’s a good idea to practice more social distancing in the days leading up to your visit with an older or vulnerable person. Home testing a few days before the visit and the day of the visit will add another layer of protection.
Gregg Gonsalves, an assistant professor of epidemiology at the Yale School of Public Health, said he recently visited his 87-year-old mother and did not wear a mask. But that is because both of them are vaccinated and he still works mostly from home, lives in a highly vaccinated area and has low risk for exposure. He is also investing in home testing kits for reassurance that he is not infectious.
“If I just came back from a big crowded gathering, and I had to go see my mom, I would put on a mask,” he said.
Is it safe to work in an office?
The answer depends on the precautions your workplace has taken. Does the company require proof of vaccination to come into the office? Are unvaccinated people tested regularly? What percentage of people in the office are unvaccinated? What steps did your company take to improve indoor air quality? (Upgrading the filters in ventilation systems and adding stand-alone HEPA air cleaners are two simple steps that can reduce viral particles in the air.)
Offices that mandate vaccination will be safer, but vaccination rates need to exceed 90 percent. Even an 85-percent vaccination rate is not enough, Dr. Jha said. “It’s not going to work because one of those 15-percent unvaccinated is going to cause an outbreak for every single person in that room,” he said. “You do not want a bunch of unvaccinated people running around your offices.”
Should I get a booster shot, and will it help protect me against Delta?
The people who have the most to gain from booster shots are older people, transplant patients, people with compromised immune systems or those with underlying conditions that put them at high risk for complications from Covid. People who received the single-dose Johnson & Johnson vaccine may also be good candidates for a second dose.
But many experts say healthy people with normal immune systems who received a two-dose mRNA vaccine from Pfizer or Moderna won’t get much benefit right now from a third shot because their vaccine antibodies still offer strong protection against severe illness. That said, the Biden administration appears to be moving ahead with offering booster shots to the general public starting as soon as the week of Sept. 20.
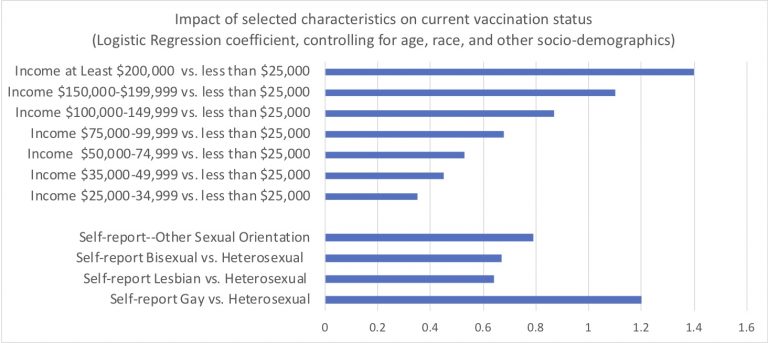
Last night I downloaded the latest Census Bureau July-August week 34 PULSE data. Over two cups of coffee, I ran the obvious multivariable logistic regressions to examine who is now fully vaccinated against COVID. See the above of this post for the full set of resulting Logit coefficients.
I’m sure Reviewer 2 would order due refinements to my quick analysis, were it immediately submitted for peer-review publication. My capacious study limitations section would note the inherent challenges of population surveys to gauge contentious questions like this. These data surely include response biases and likely overstate the true prevalence of COVID vaccination.
The overall patterns and disparities remain clear enough. Of course, we see huge disparities across regions, by education and by income. A bit more surprising: One group appears especially vulnerable and requires specific outreach…Yup. We must formulate culturally competent public health messaging for heterosexual non-Hispanic white Americans. This group conspicuously lags in vaccination status.
Among self-identified male respondents, heterosexual men were almost four times as likely to report not to be fully vaccinated (19%) as were gay men (5%)–an absolute different quite similar to the gradient observed between men with incomes less than $25,000 and those with incomes between $75,000 and $100,000.
I know that there daunting obstacles to reaching this disparity-population of heterosexual American men. We can’t let these barriers deter us. I’m joking–sort of. OK not really.
Droplets, fomites, aerosols…these terms describing the kinds of particles which can spread virus particles rose to the top of our lexicon last year. Initially we focused on fomites, infectious particles deposited on surfaces, and worried that touching our groceries and mail could spread the coronavirus.
Scientists were convinced that most COVID transmission occurred via droplets, large respiratory particles exhaled in a cough or a sneeze that traveled only a short distance from an infected person, which led to the guidance that staying six feet apart would keep us safe. But worrisome case reports of a single individual passing the virus to a roomful of people, and the mitigating effects of ventilation, began to hint at aerosol transmission, a much more insidious type of spread in which the virus is transmitted through much smaller particles, which travel longer distances and can linger in the air for hours.
Aerosol spread is not only worrisome because it makes a pathogen more contagious, but smaller aerosol particles can be inhaled more deeply into the lungs, potentially causing more severe illness. A new review in Science evaluates the current data on COVID transmission and the advances made over the past year in understanding airflow and aerosol spread, making the bold statement that aerosol transmission is not only the main mechanism for COVID-19 spread, but is likely the primary mode of transmission for the vast majority of respiratory diseases.
Today, our lack of attention to ventilation, air purification and other means to reduce aerosol spread means that we are woefully unprepared for children to return to school—and underscores the need for extensive masking to mitigate transmission. But in the long run, better understanding the mechanisms for preventing airborne transmission could allow us to reduce susceptibility to a host of respiratory diseases. Take complications from asthma, which dropped dramatically during the pandemic—leading researchers to posit that viral infections, rather than environmental triggers, could be the more common cause behind exacerbations.
Harnessing this new knowledge will require further research to quantify the effects of spread and mitigation—and the willingness to invest in preventive measures in schools and other public spaces, yet another domain in which bolstering public health could have a meaningful long-term impact on our lives.
When COVID volumes waned in the spring and early summer, most health systems “de-escalated” dedicated COVID testing and triage facilities. But with the Delta variant surging across the country, consumers are now once again looking for services like drive-through testing, which is perceived as more convenient and safer.
One physician leader told us patients in the ED are asking why the hospital got rid of the “COVID tent”, which provided a separate pathway for patients with respiratory and other COVID symptoms—and a highly visible signal that the rest of the department was as COVID-free as possible.
Another system is now fielding questions from the media about whether they’ll bring back their dedicated COVID hospital: “We spent a lot of time last year convincing the community that the dedicated hospital was key to safely managing care during the pandemic. Now we’ve got almost as many COVID admissions spread across our hospitals.”
Over the past year, providers have learned how to safely manage COVID care and prevent spread in healthcare settings—but consumers may perceive the lack of dedicated facilities as a decline in safety.
Unlike last year, hospitals are full of non-COVID patients, as those who delayed care reemerge. And with the current surge likely to continue into flu season, emergency rooms will only get more crowded, necessitating a new round of communication describing how hospitals are keeping patients safe, and reassuring patients that healthcare settings remain one of the safest places to visit in the community.
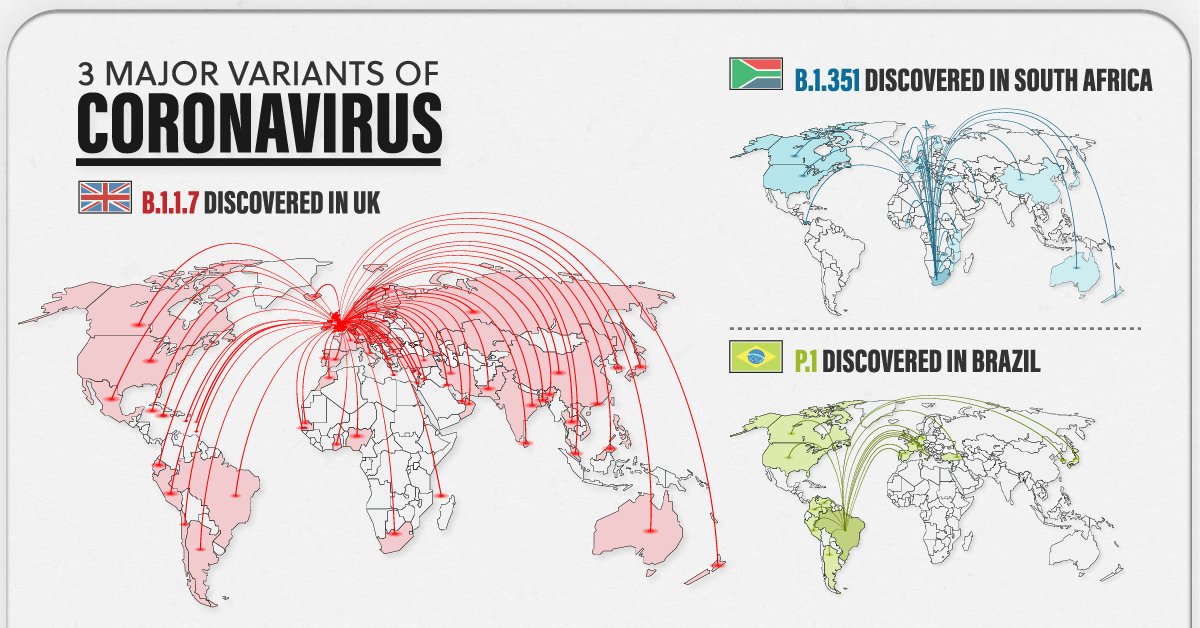
As billions of people gear up for widespread vaccination against COVID-19, another issue has reared its head. Three major COVID-19 variants have emerged across the globe—and preliminary research suggests these variants may be cause for concern.
But what makes them different from the original strain?
The following visualizations answer some key questions, including when these variants were first discovered, how far they’ve spread worldwide, and most importantly, their potential impact on the population.
Some Context: What is a Variant?
Before diving in, it’s important to understand why viruses mutate in the first place.
To infect someone, a virus takes over a host cell and uses it to replicate itself. But nature isn’t perfect, and sometimes, mistakes are made during the replication process—those mistakes are called mutations.
A virus with one or more mutations is referred to as a variant. Most of the time, variants do not affect a virus’s physical structure, and in those instances, they eventually disappear. However, there are certain cases when a mutation impacts part of a virus’s genetic makeup that does change its behavior.
According to the U.S. Centers for Disease Control (CDC) a change in behavior can alter:
Rate of transmission
Deadliness
Ability to potentially infect someone with natural or vaccine-induced immunity
Preliminary research has detected some of these changes in the three major COVID-19 variants—B.1.1.7, B.1.351, and P.1.
The 3 Major COVID-19 Variants
The three major variants emerged at different times, and in different parts of the world. Here’s an overview of each variant, when they were discovered, and how far they’ve spread so far.
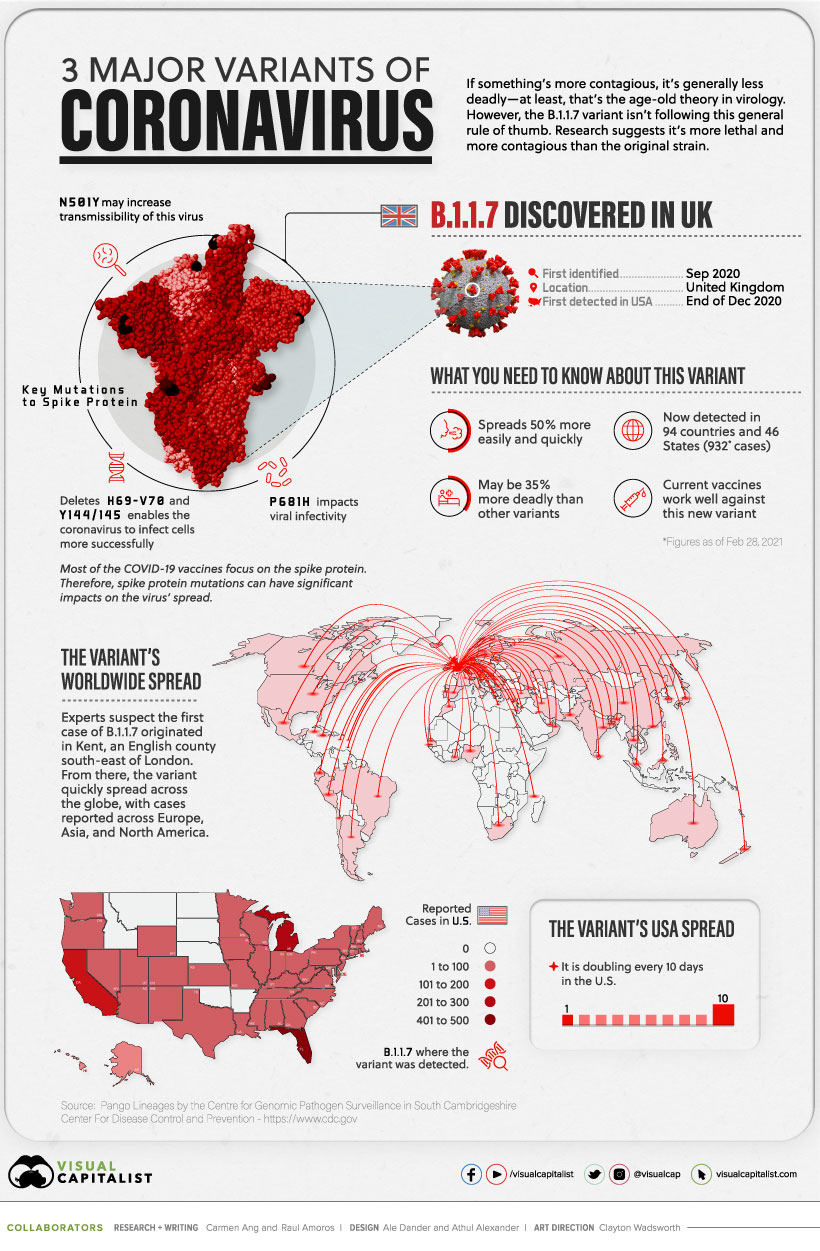
B.1.1.7
The B.1.1.7 variant was detected in the UK in the fall of 2020. By December 2020, it had spread across the globe, with cases emerging across Europe, North America, and Asia.
Currently, the variant has been reported in roughly 94 countries.
Early research suggests it’s 50% more transmissible than other variants, and potentially 35% more deadly than the standard virus. Luckily, studies suggest that some of the existing vaccines work well against it.
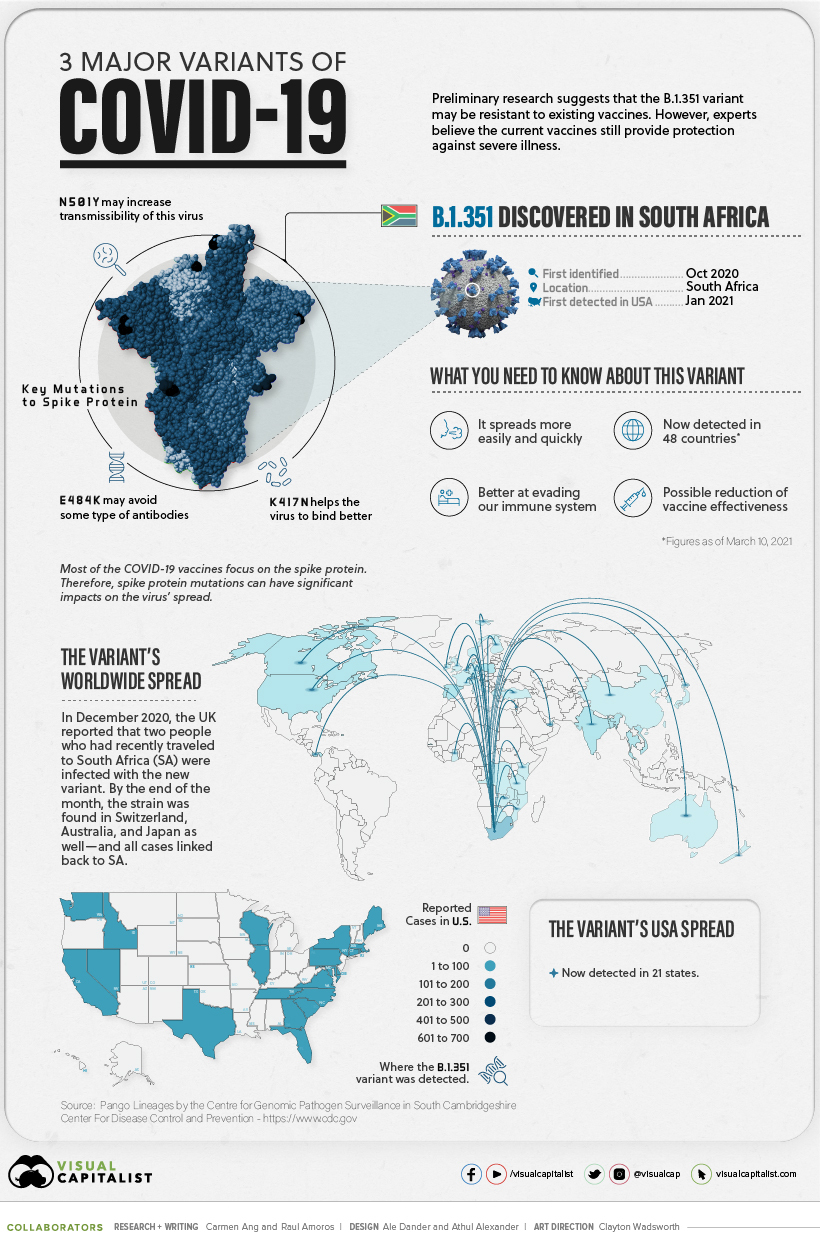
B.1.351
In October 2020, the second major variant was discovered—B.1.351. It was first identified in South Africa, but by end of the year, it had spread to the UK, Switzerland, Australia, and Japan.
There are approximately 48 countries with reported cases, and research suggests several of the existing COVID-19 vaccines may not be as effective against this variant.
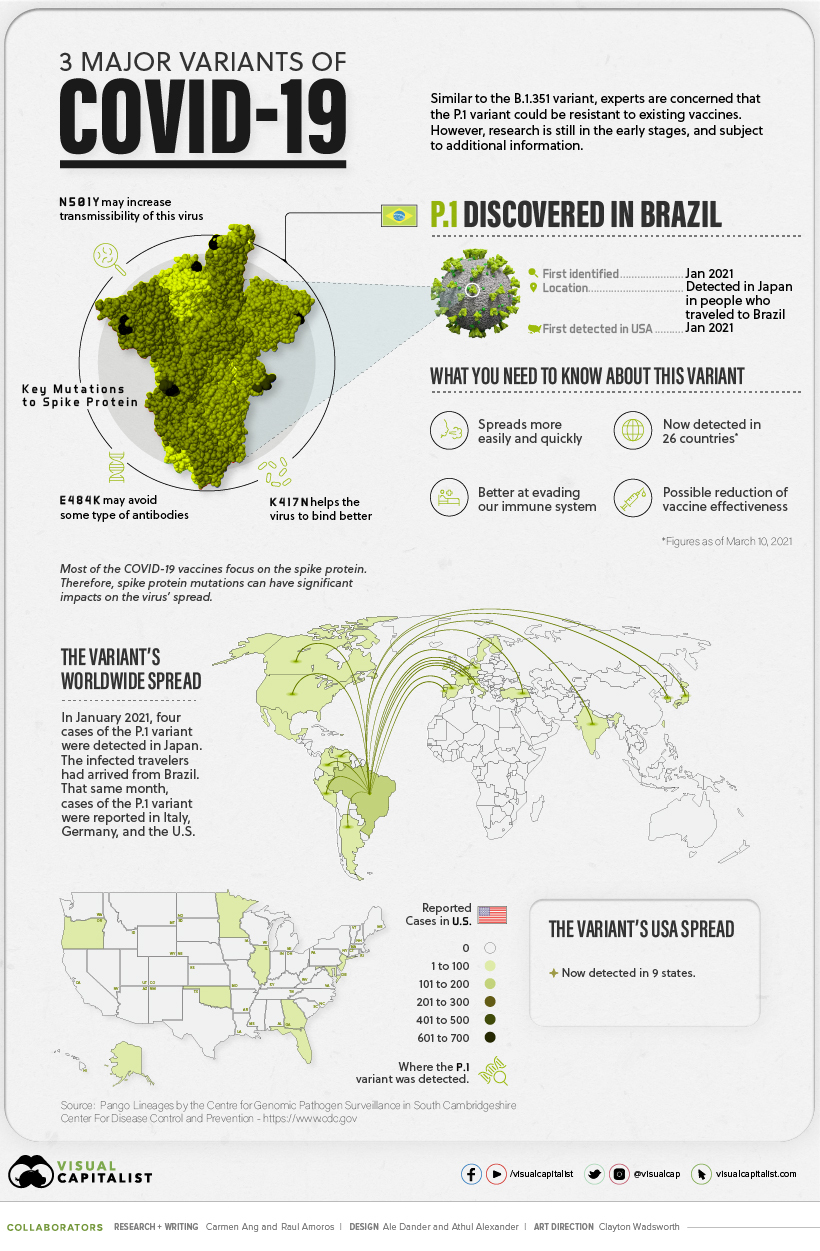
P.1
The P.1 variant was the last to arrive on the scene.
It was first discovered in January 2021, when Japan reported four cases of the variant, which was found in travelers who had arrived from Brazil.
Approximately 25 countries have reported cases of the P.1 variant, and early research suggests this variant is not only more contagious, but could also have the ability to infect people with natural immunity who had already recovered from the original strain.
Still Early Days
While there have been preliminary studies showing a dip in vaccine effectiveness, some experts emphasize that it’s too early to tell for certain. More data is needed to gain a deeper and more accurate understanding.
In the meantime, experts are emphasizing the importance of following our current public health strategies, which include physical distancing, vaccination, washing your hands, and using masks.