Starting next month, UnitedHealthcare says it will move forward with plans to drop prior authorization requirements for a range of procedures, including dozens of radiology services and genetic tests, among others.
Why it matters:
UnitedHealth is among the health insurance giants who have announced plans to cut back on prior authorization as federal regulators consider tougher curbs on the practice.
Catch up quick:
Prior authorization is often criticized by patients and doctors, who complain they are an administrative burden or impede necessary care. Insurers, meanwhile, say prior authorization provides important guardrails against improper health care utilization, helping to keep costs down.
UnitedHealth, the largest commercial U.S. insurer, previously said its prior authorization removals will represent roughly 20% of its overall prior authorization volume.
Cigna and Aetna also announced plans to roll back some prior authorization requirements.
The Centers for Medicare and Medicaid Services proposed a rule to limit the amount of time insurers have to review requests on services for which they require prior approval, BenefitsPro previously reported.
Congress is also eyeing a plan to streamline and add transparency to the process by which Medicare Advantage plans can deny coverage for services via prior authorization.
Zoom in:
UnitedHealth says the removals will take effect Sept. 1 and Nov. 1 across the vast majority of its plans.
The company also spelled out which procedures would see prior authorization requirements removed. For instance, hundreds of codes for genetic testing — accounting for tens of thousands of prior authorization requests a year from commercial and Medicaid members — are among those that will be removed, officials said.
A code for cardiology stress test prior authorization for Medicare Advantage members will also be eliminated, reducing roughly 316,000 prior authorization requests a year.
The company next year also will roll out a “gold card” program eliminating most prior authorization requirements for doctors who have high approval rates.
Flashback: Earlier this summer, UnitedHealth walked back a controversial plan to require prior authorizations for colonoscopies and other endoscopic procedures.
Starting June 1, UnitedHealthcare will require physicians to submit prior authorization requests for certain types of colonoscopies. While routine screening colonoscopies will remain exempt, United beneficiaries requiring surveillance or diagnostic colonoscopies—which are performed on patients at greater risk of developing colon cancer or those already exhibiting worrisome symptoms—will need advance approval for the procedures to be covered by the payer. A UnitedHealthcare spokesperson said that this policy change is due to concerns that colonoscopy overutilization generates unnecessary medical risks and higher healthcare spending for patients.
The American College of Gastroenterology released a statement criticizing the new policy on the grounds that prior authorization requirements create harmful delays for patients and are a significant source of provider burnout.
The Gist: So much for the planned rollback of prior authorizations that UnitedHealthcare recently touted.
While the insurer is not wrong in saying that some studies have documented overutilization of colonoscopies,
prior authorization is a blunt tool that takes care decision making out of practicing providers’ hands, redirecting that power (along with more profit) to the payer.
To process prior authorization requests in a timely manner, insurers now commonly rely on AI algorithms, which are an imperfect solution. For patients exhibiting signs of colon cancer,improper denials and delayed approvals for colonoscopies could have life-threatening implications.
American Medical Association President Jack Resneck Jr., MD, detailed in a post on the medical group’s website the “Kafkaesque” prior authorization process that an unnamed insurance company allegedly put one of his patients through.
Dr. Resneck, a San Francisco-based dermatologist, was treating a patient with severe head-to-toe eczema, who was unable to sleep because of the condition, according to the post. Dr. Resneck found a medication that allowed the patient to sleep and return to work.
Several months later, however, the patient was unable to get the prescription refilled at the pharmacy, according to the report. Dr. Resneck completed the paperwork describing how well the patient had responded to the medication, as required by the insurance company, and faxed it over. The prior authorization request for the prescription refill was rejected.
Dr. Resneck said the insurance company rejected the refill on the grounds that the patient no longer met the severity criteria because not enough of his body was covered and he was not missing enough sleep.
The insurance company allegedly wanted to take the patient off the medication for several weeks to let his eczema flare up again, according to the post. It took more than 20 additional telephone calls until the patient’s prescription was refilled.
A lack of data about Medicare Advantage plans means there are several unanswered questions about the program, according to an analysis from Kaiser Family Foundation.
The analysis, published April 25, breaks down the kinds of Medicare Advantage data not publicly available. Some missing data is not collected from insurers by CMS, and some data is collected by the agency but not available to the public.
Here are five questions researchers can’t answer without more data, according to Kaiser Family Foundation:
Insurers are not required to report how many enrollees use supplemental benefits and if members incur out-of-pocket costs with their supplemental benefits. Without this data, researchers can’t answer what share of enrollees use their supplemental benefits, how much members spend out of pocket for supplemental benefits, and if these benefits are working to achieve better health outcomes.
CMS does not require Medicare Advantage plans to report prior authorizations by type of service. Without more granular data, researchers can’t determine which services have the highest rates of denial and if prior authorization rates vary across insurers and plans.
Insurers are also not required to report the reasons for prior authorization denials to CMS. This leaves unanswered questions, including what is the most common reason for denials and if rates of denials vary across demographics.
Medicare Advantage plans do not report complete data on denied claims for services already provided. Without this data, researchers cannot determine how often payers deny claims for Medicare-covered services and reasons why these claims are denied.
CMS does not publish the names of employers or unions that receive Medicare funds to provide Medicare Advantage plans to retired employees. Without more data, researchers can’t tell which industries use Medicare Advantage most often and how rebates vary across employers.
After 18 years as CEO in Kaiser Permanente, I set my sights on improving the heatlh of the nation, hoping to find a way to achieve the same quality, technology and affordability our medical group delivered to 5 million patients on both coasts.
That quest launched the Fixing Healthcare podcast in 2018, and it inspired interviews with dozens of leaders, thinkers and doers, both in and around medicine. These experts shared innovative ideas and proven solutions for achieving (a) superior quality, (b) improved patient access, (c) lower overall costs, and (d) greater patient and clinician satisfaction.
Which of the hundreds of ideas presented remain most promising?
Why, after five years and so many excellent solutions, has our nation experienced such limited improvements in healthcare?
And finally, how will these great ideas become reality?
To answer the first question, I offer 15 of the best Fixing Healthcare recommendations so far. Some quotes have been modified for clarity with links to all original episodes (and transcripts) included.
Fixing the business of medicine
1. Malcolm Gladwell, journalist and five-time bestselling author: “In other professions, when people break rules and bring greater economic efficiency or value, we reward them. In medicine, we need to demonstrate a consistent pattern of rewarding the person who does things better.”
2. Richard Pollack, CEO of the American Hospital Association (AHA): “I hope in 10 years we have more integrated delivery systems providing care, not bouncing people around from one unconnected facility to the next. I would hope that we’re in a position where there’s a real focus on ensuring that people get care in a very convenient way.”
Eliminating burnout
3. Zubin Damania, aka ZDoggMD, hospitalist and healthcare satirist: “In the culture of medicine, specialists view primary care as the weak medical students, the people who couldn’t get the board scores or rotation honors to become a specialist. Because why would you do primary care? It’s miserable. You don’t get paid enough. It’s drudgery. We must change these perceptions.”
4. Devi Shetty, India’s leading heart surgeon and founder of Narayana Health: “When you strive to work for a purpose, which is not about profiting yourself, the purpose of our action is to help society, mankind on a large scale. When that happens, cosmic forces ensure that all the required components come in place and your dream becomes a reality.”
5. Jonathan Fisher, cardiologist and clinician advocate: “The problem we’re facing in healthcare is that clinicians are all siloed. We may be siloed in our own institution thinking that we’re doing it best. We may be siloed in our own specialty thinking that we’re better than others. All of these divides need to be bridged. We need to begin the bridging.”
Making medicine equitable
6. Jen Gunter, women’s health advocate and “the internet’s OB-GYN”: “Women are not listened to by doctors in the way that men are. They have a harder time navigating the system because of that. Many times, they’re told their pain isn’t that serious or their bleeding isn’t that heavy. We must do better at teaching women’s health in medicine.”
7. Amanda Calhoun, activist, researcher and anti-racism educator: “A 2015 survey showed that white residents and medical students still thought Black people feel less pain, which is wild to me because Black is a race. It’s not biological. This is actually an historical belief that persists. One of the biggest things we can do as the medical system is work on rebuilding trust with the Black community.”
Addressing social determinants of health
8. Don Berwick, former CMS administrator and head of 100,000 Lives campaign: “We know where the money should go if we really want to be a healthy nation: early childhood development, workplaces that thrive, support to the lonely, to elders, to community infrastructures like food security and transportation security and housing security, to anti-racism and criminal-justice reform. But we starve the infrastructures that could produce health to support the massive architecture of intervention.”
9. David T. Feinberg, chairman of Oracle Health: “Twenty percent of whether we live or die, whether we have life in our years and years in our life, is based on going to good doctors and good hospitals. We should put the majority of effort on the stuff that really impacts your health: your genetic code, your zip code, your social environment, your access to clean food, your access to transportation, how much loneliness you have or don’t have.”
Empowering patients
10. Elisabeth Rosenthal, physician, author and editor-in-chief of KHN: “To patients, I say write about your surprise medical bills. Write to a journalist, write to your local newspaper. Hospitals today are very sensitive about their reputations and they do not want to be shamed by some of these charges.”
11. Gordon Chen, ChenMed CMO: “If you think about what leadership really is, it’s influence. Nothing more, nothing less. And the only way to achieve better health in patients is to get them to change their behaviors in a positive way. That behavior change takes influence. It requires primary care physicians to build relationship and earn trust with patients. That is how both doctors and patients can drive better health outcomes.”
Utilizing technology
12. Vinod Khosla, entrepreneur, investor, technologist: “The most expensive part of the U.S. healthcare system is expertise, and expertise can relatively be tamed with technology and AI. We can capture some of that expertise, so each oncologist can do 10 times more patient care than they would on their own without that help.”
13. Rod Rohrich, influential plastic surgeon and social media proponent: “Doctors, use social media to empower your audience, to educate them, and not to overwhelm them. If you approach social media by educating patients about their own health, how they can be better, how can they do things better, how they can find doctors better, that’s a good thing.”
Rethinking medical education
14. Marty Makary, surgeon and public policy researcher: “I would get rid of all the useless sh*t we teach our medical students and residents and fellows. In the 16 years of education that I went through, I learned stuff that has nothing to do with patient care, stuff that nobody needs to memorize.”
15. Eric Topol, cardiologist, scientist and AI expert: “It’s pretty embarrassing. If you go across 150 medical schools, not one has AI as a core curriculum. Patients will get well versed in AI. It’s important that physicians stay ahead, as well.”
Great ideas, but little progress
Since 2018, our nation has spent $20 trillion on medical care, navigated the largest global pandemic in a century and developed an effective mRNA vaccine, nearly from scratch. And yet, despite all this spending and scientific innovation, American medicine has lost ground.
American life expectancy has dropped while maternal mortality rates have worsened. Clinician burnout has accelerated amid a growing shortage of primary care and emergency medicine physicians. And compared to 12 of its wealthiest global peers, the United States spends nearly twice as much per person on medical care, but ranks last in clinical outcomes.
Guests on Fixing Healthcare generally agree on the causes of stagnating national progress.
Healthcare system giants, including those in the drug, insurance and hospital industries, find it easier to drive up prices than to prevent disease or make care-delivery more efficient. Over the past decade, they’ve formed a conglomerate of monopolies that prosper from the existing rules, leaving them little incentive to innovate on behalf of patients. And in this era of deep partisan divide, meaningful healthcare reforms have not (and won’t) come from Congress.
Then who will lead the way?
Industry change never happens because it should. It happens when demand and opportunity collide, creating space for new entrants and outsiders to push past the established incumbents. In healthcare, I see two possibilities:
1. Providers will rally and reform healthcare
Doctors and hospitals are struggling. They’re struggling with declining morale and decreasing revenue. Clinicians are exiting the profession and hospitals are shuttering their doors. As the pain intensifies, medical group leaders may be the ones who decide to begin the process of change.
The first step would be to demand payment reform.
Today’s reimbursement model, fee-for-service, pays doctors and hospitals based on the quantity of care they provide—not the quality of care. This methodology pushes physicians to see more patients, spend less time with them, and perform ever-more administrative (billing) tasks. Physicians liken it to being in a hamster wheel: running faster and faster just to stay in place.
Instead, providers of care could be paid by insurers, the government and self-funded businesses directly, through a model called “capitation.” With capitation, groups of providers receive a fixed amount of money per year. That sum depends on the number of enrollees they care for and the amount of care those individuals are expected to need based on their age and underlying diseases.
This model puts most of the financial risk on providers, encouraging them to deliver high-quality, effective medical care. With capitation, doctors and hospitals have strong financial incentives to prevent illnesses through timely and recommended preventive screenings and a focus on lifestyle-medicine (which includes diet, exercise and stress reduction). They’re rewarded for managing patients’ health and helping them avoid costly complications from chronic diseases, such as heart attacks, strokes and cancer.
Capitation encourages doctors from all specialties to collaborate and work together on behalf of patients, thus reducing the isolation physicians experience while ensuring fewer patients fall through the cracks of our dysfunctional healthcare system. The payment methodology aligns the needs of patients with the interests of providers, which has the power to restore the sense of mission and purpose medicine has lost.
Capitation at the delivery-system level eliminates the need for prior authorization from insurers (a key cause of clinician burnout) and elevates the esteem accorded to primary care doctors (who focus on disease prevention and care coordination). And because the financial benefits are tied to better health outcomes, the capitated model rewards clinicians who eliminate racial and gender disparities in medical care and organizations that take steps to address the social determinants of health.
2. Major retailers will take over
If clinicians don’t lead the way, corporate behemoths like Amazon, CVS and Walmart will disrupt the healthcare system as we know it. These retailers are acquiring the insurance, pharmacy and direct-patient-care pieces needed to squeeze out the incumbents and take over American healthcare.
Each is investing in new ways to empower patients, provide in-home care and radically improve access to both in-person and virtual medicine. Once generative AI solutions like ChatGPT gain enough computing power and users, tech-savvy retailers will apply this tool to monitor patients, enable healthier lifestyles and improve the quality of medical care compared to today.
When Fixing Healthcare debuted five years ago, none of the show’s guests could have foreseen a pandemic that left more than a million dead. But, had our nation embraced their ideas from the outset, many of those lives would have been saved. The pandemic rocked an already unstable and underperforming healthcare system. Our nation’s failure to prevent and control chronic disease resulted in hundreds of thousands of unnecessary deaths from Covid-19. Outdated information technology systems, medical errors and disparities in care caused hundreds of thousands more. As a nation, we could have done much better.
With the cracks in the system widening and the foundation eroding, disruption in healthcare is inevitable. What remains to be seen is whether it will come from inside or outside the U.S. healthcare system.
Last Friday, the Centers for Medicare and Medicaid Services (CMS) announced that it will begin phasing in major Medicare Advantage (MA) risk-adjustment changes over a three-year period, slower than previously anticipated. Thanks to this delay in full implementation, MA plans will see an average 3.3 percent payment increase in 2024, up from the one percent projected in the earlier draft notice.
CMS also finalized regulations this week that aim to limit MA prior authorizations and denials by requiring that coverage decisions align with traditional Medicare.
The Gist: After CMS began proposing changes to MA payment formulas last year, aimed at reining in pervasive abuses and fraud,
the insurance industry responded with a $13M marketing blitz to oppose the changes.
The ads, one of which aired during the Super Bowl, tied Medicare Advantage “cuts” to the time-tested “Hands Off My Medicare” messaging directed at seniors.
With MA enrollment projected to overtake traditional Medicare this year,the federal government finds itself walking a tightrope in clamping down on overpayments to MA plans, given that any reductions will impact a growing number of seniors.
On Wednesday, UnitedHealth Group (UHG) announced that it will reduce its prior authorization claims volume by 20 percent for its commercial, Medicare Advantage, and Medicaid businesses later this year. Next year, it will launch a “gold card” program for qualifying providers that will further streamline care approvals. Cigna also shared that it has removed nearly 500 services from prior authorization review since 2020, relying on an electronic process for faster response times. These changes come in the wake of a Centers for Medicare and Medicaid Services (CMS) proposed rule, set to be finalized in April, that aims to streamline prior authorization by requiring certain payers to establish a method for electronic transmission, shorten response time for physician requests, and provide a reason for denials.
The Gist: These changes address two of providers’ primary complaints around prior authorizations: there are too many of them, and payers take too long to process them. However, technology options aiming to solve this problem through automation are by no means a foolproof solution.
As ProPublica recently reported, algorithm-based electronic claims processing solutions that improve response times can create other challenges, including improper automatic denials, and can expand prior authorization to lower-cost services, for which it was previously determined to be inefficient to rely on human review. Quicker responses must still be accurate and fair, necessitating that insurance companies closely monitor, audit, and hone technology solutions.
A working paper published this week by the National Bureau of Economic Research found that prior authorization requirements reduced drug spending far more than they increased physicians’ administrative costs.
Using a random assignment of plans within Medicare Part D’s low-income subsidy program, the study determined that a prior authorization requirement decreased a drug’s utilization by just over 25 percent, with around half of denied beneficiaries opting for a comparable alternative and the other half receiving no drug at all. This generated $96 in per-beneficiary-per-year savings, which the authors estimate to be around 10 times greater than the administrative costs incurred.
The Gist: Physician groups have long despised prior authorization processes, listing it as their most burdensome regulatory issue. While studies like this are useful for demonstrating the returns from these processes and putting the tradeoffs in perspective, they fail to account for who is bearing the burden of the time spent, and who captures the cost savings: physicians bear the administrative costs, and payers capture the returns. Not to mention that worried patients, anxious to receive treatment, are often put in the position of “quarterbacking” a convoluted and bureaucratic appeals process.
Ongoing work should focus on streamlining authorizations, to lessen the impact on physicians’ time and satisfaction, and make navigating the process simpler for patients. An increasing array of technology options aims to solve this problem though automation, but the challenge remains for payers and providers to come together to deliver on that potential.
On Tuesday, the Centers for Medicare and Medicaid Services (CMS) announced a proposed rule that aims to streamline the prior authorization process by requiring certain payers to establish a method for electronic transmission, shorten response time for physician requests, and provide a reason for denials. This rule replaces one proposed in December 2020 that was never finalized.
In addition to applying to Medicaid and Affordable Care Act exchange plans, the new rule would also apply to Medicare Advantage plans, which the previous rule did not. If finalized, it will take effect in 2026.
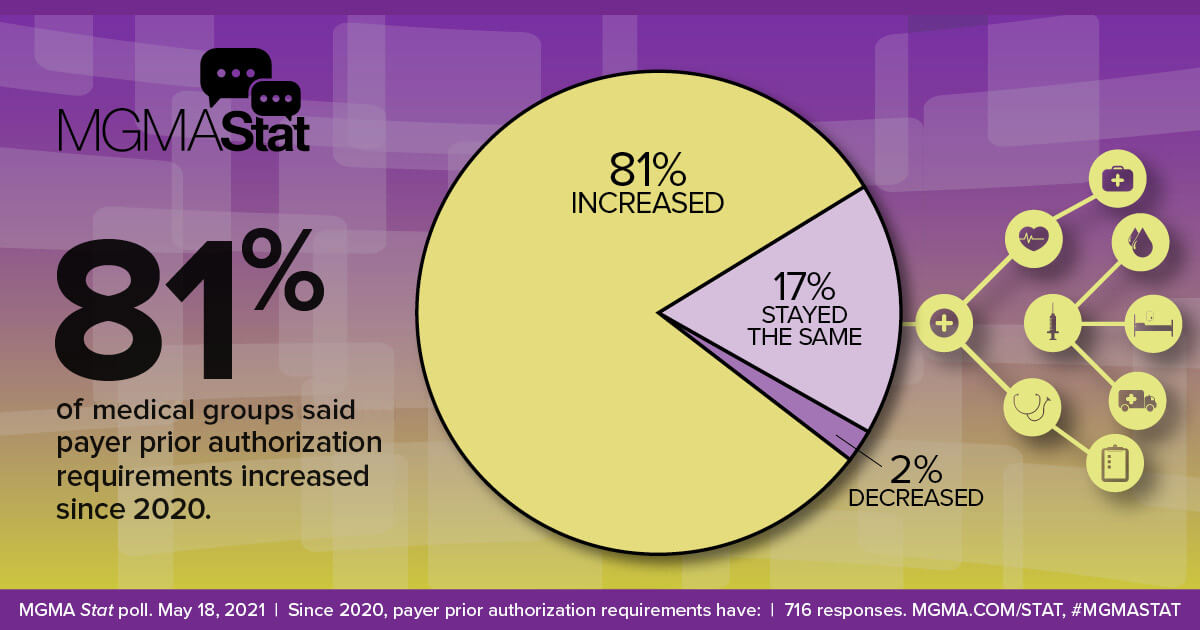
The Gist: Managing prior authorization requests is one of providers’ greatest sources of frustration, with over 80 percent of physicians rating it as “very or extremely burdensome” in a recent Medical Group Management Association survey.
Not only would patients would benefit from faster turnarounds, but even major payers agree that the status quo is suboptimal, and payer advocacy organization AHIP has signaled support for transmitting prior authorization requests electronically.
The challenge for regulators will be to strike a balance that satisfies the competing interests of payers and providers—turnaround time is likely to be a sticking point—but the one good thing about a system that no one likes is that there’s plenty of room for improvement.
Currently there is a resolution HR 7995 in the U.S. House of Representatives, introduced late last week, that will decrease prior authorization delays for patients awaiting care.
The very manual, time-consuming processes, for prior authorization, burden physicians, physician practices, and hospitals while diverting valuable resources away from direct patient care. HR 7995 was referred to the Committee on Ways and Means in addition to the Committee on Energy and Commerce.
Now that the framework of this bill is still being worked, it is crucial to get in front of legislators and let them know that you support this legislation that will decrease prior authorization delays ensuring continuity of care to patients because it:
Exempts qualifying physicians from prior authorization requirements under Medicare Advantage (MA) (providing for a “Gold Card” status for physicians that consistently meet prior authorization requirements).
Allows physicians to appeal “Gold Card” revocation from insurers that are wrongly decided.
Requires Secretary of HHS to issue rules on MA plans.