While we have mercifully moved beyond the crisis phase of the pandemic, COVID remains a leading cause of US deaths, taking the lives of hundreds of Americans each day.
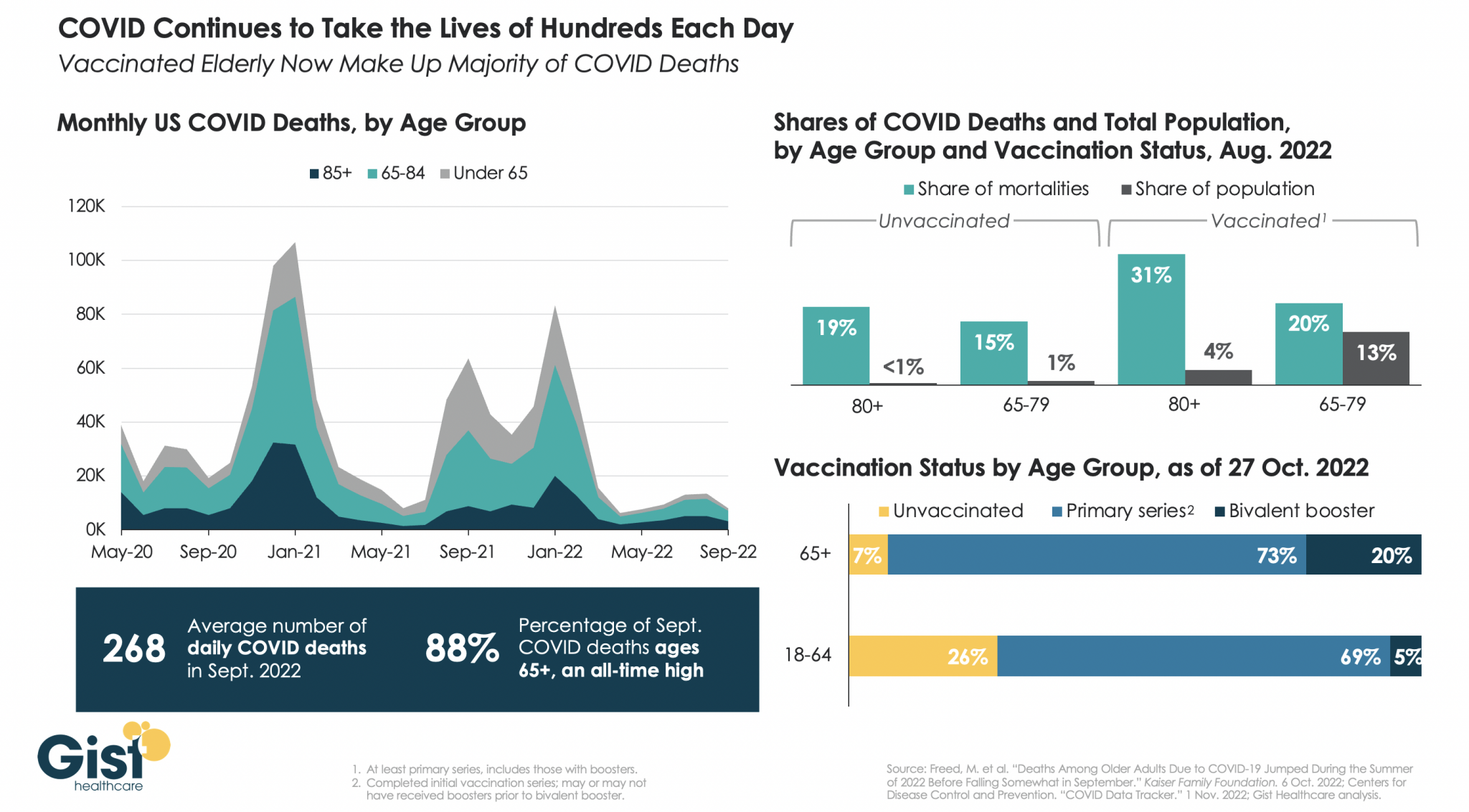
In the graphic above, we analyzed COVID mortality data, finding the defining characteristic of Americans still dying of COVID is age. As death rates have dropped, the percentage of COVID deaths accounted for by individuals 65 years or older has risen to an all-time high of 88 percent.
Notably, a majority of people dying of COVID today are vaccinated, due to the high rate of vaccination in the 65+ population. While the near-universal vaccination of seniors, including the fact that one in five have received the most recent bivalent booster, is not sufficient to save all of their lives, unvaccinated seniors are still dying at higher rates than vaccinated ones.
In August 2022, vaccinated individuals over age 80, who represent about four percent of the total US population, made up 31 percent of COVID deaths, while unvaccinated individuals in the same age group, who represent less than one percent of the total population, made up 19 percent of COVID deaths.
We entered 2020 with about 55M Americans ages 65 and older, and have since lost 790K, or nearly 1.5 percent of the senior population, to COVID. Meanwhile, reports of the new, immune-evasive BQ variant sweeping New York and California remind us that COVID’s not done with us yet, even if we think we’re done with it.
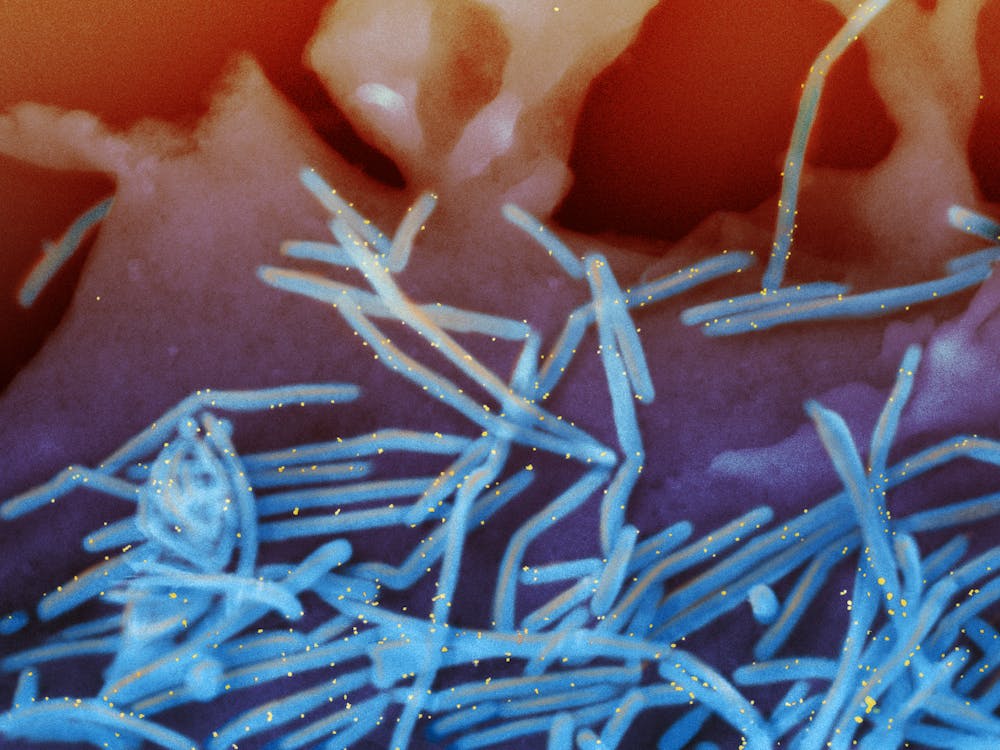
Respiratory syncytial virus, more commonly known as RSV, sends thousands of children to the hospital every year in the U.S. But during September and October 2022, health professionals across the country have watched an unprecedented spike in the number of cases of this usually mild, but occasionally dangerous, respiratory infection in children.Jennifer Girotto is a pharmacist who studies pediatric infectious diseases. She explains how RSV infects the human body, who is most at risk and what might be causing this year’s outbreak to be worse than normal.
1. What is respiratory syncytial virus?
RSV is a common, RNA respiratory virus that affects about 2 million children under 5 years old annually nationwide. Researchers think that most children have been infected by age 2. Like the flu, in most areas of the U.S., RSV usually circulates from November through March and then mostly disappears during the summer months, with only sporadic cases being seen.
For most people, especially those who have had an RSV infection in the past, the virus only causes mild symptoms like cough, runny nose and fever, with instances of wheezing and decreased appetite more common in young children.
But young infants, especially those under 6 months old, born prematurely or with congenital heart, lung or other health issues are at increased risk for more severe symptoms. The U.S. Centers for Disease Control and Prevention estimates that 1% to 2% of infants younger than 6 months who get infected with RSV require hospitalization. In an average year, around 250 children die from the disease.
The main reason RSV sends babies and young children to the hospital is because the virus infects and kills surface cells within small sacs of the lungs. The body responds by increasing the production of mucus and fluid in these areas. But the extra mucus can plug up and obstruct these parts of the lung and make it so that an infant doesn’t get enough oxygen.
A second common cause for hospitalization due to RSV is pneumonia, where a person’s lungs fill up with fluid. The pneumonia can either be triggered by the virus itself or by a secondary, bacterial infection. Finally, some infants get so sick that they struggle to eat and are unable to take in sufficient nutrients, eventually landing them in the hospital.
Health officials aren’t yet sure why the outbreak is so bad this year, but the COVID-19 pandemic may have something to do with it. Some research has shown that seasonality of RSV has shifted. In 2021, RSV infections started much earlier than normal, and over the summer of 2022, they never quite went away. One theory as to why RSV season is starting earlier and hitting harder is that, due to social distancing measures since 2020, an unusually high number of infants and children are experiencing their first exposures and infections at once.
5. How can you protect against catching RSV?
Like colds and the flu, RSV infections spread when people touch dirty surfaces or from respiratory droplets, when an infected person coughs or sneezes.
If someone is sick with symptoms that look like a cold, it may be best to avoid close contact until they feel better, especially if you have young children or high-risk people around.
While infections, hospitalizations, and deaths from Covid-19 have been steadily declining in the United States in recent months, experts warn that rising cases in Europe may be “a harbinger for what’s about to happen in the United States,” Rob Stein writes for NPR’s “Shots.”
Will the US see a ‘winter resurgence’ of Covid-19?
Currently, several models project that U.S. Covid-19 infections will continue to decline at least until the end of 2022. However, researchers caution that there are multiple variables that could change current projections, including whether more infectious strains start circulating around the nation.
According to Stein, “[t]he first hint of what could be in store is what’s happening in Europe.” Recently, many European countries, including the U.K., France, and Italy, have seen an increase in Covid-19 infections.
“In the past, what’s happened in Europe often has been a harbinger for what’s about to happen in the United States,” said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota. “So I think the bottom line message for us in this country is: We have to be prepared for what they are beginning to see in Europe.”
“We look around the world and see countries such as Germany and France are seeing increases as we speak,” said Lauren Ancel Meyers, director of the UT COVID-19 Modeling Consortium at the University of Texas at Austin. “That gives me pause. It adds uncertainty about what we can expect in the coming weeks and the coming months.”
However, Justin Lessler, an epidemiologist at the University of North Carolina who helps run the COVID-19 Scenario Modeling Hub, noted that the United States may not have the same experience as Europe, largely because it is unclear whether Europe’s increase is related to individuals’ vulnerability to new strains.
“If it is mostly just behavioral changes and climate, we might be able to avoid similar upticks if there is broad uptake of the bivalent vaccine,” Lessler added. “If it is immune escape across several variants with convergent evolution, the outlook for the U.S. may be more concerning.”
Some researchers believe the United States is already experiencing early signs of this. “For example, the levels of virus being detected in wastewater is up in some parts of the country, such in Pennsylvania, Connecticut, Vermont and other parts of Northeast,” Stein writes. “That could an early-warning sign of what’s coming, though overall the virus is declining nationally.”
“It’s really too early to say something big is happening, but it’s something that we’re keeping an eye on,” said Amy Kirby, national wastewater surveillance program lead at CDC.
According to David Rubin, the director of the PolicyLab at Children’s Hospital of Philadelphia, which tracks the pandemic, Covid-19 infections and hospitalizations are already rising in some parts of New England, and other northern regions, including the Pacific Northwest.
“We’re seeing the northern rim of the country beginning to show some evidence of increasing transmission,” Rubin said. “The winter resurgence is beginning.”
How likely is a severe Covid-19 surge?
Unless a “dramatically different new variant emerges,” it is “highly unlikely this year’s surge would get as severe as the last two years in terms of severe disease and deaths,” Stein writes.
“We have a lot more immunity in the population than we did last winter,” said Jennifer Nuzzo, who leads the Pandemic Center at the Brown University School of Public Health.
“Not only have people gotten vaccinated, but a lot of people have now gotten this virus. In fact, some people have gotten it multiple times. And that does build up [immunity] in the population and reduce overall over risk of severe illness,” Nuzzo said.
Another factor that could affect the severity of the impact of rising infections is the number of people who receive updated Covid-19 vaccines, which help boost waning immunity from previous infections or shots.
However, the United States’ booster uptake has been slow. “Nearly 50% of people who are eligible for a booster have not gotten one,” said William Hanage, an associate professor of epidemiology at the Harvard T.H. Chan School of Public Health. “It’s wild. It’s really crazy.”
Since updated boosters became available in September, less than 8 million of the over 200 million people who are eligible have received one.
According to Nuzzo, it is critical for people to stay up to date on their vaccines, especially with the high likelihood of another Covid-19 surge. “The most important thing that we could do is to take off the table that this virus can cause severe illness and death,” Nuzzo said.
“There are a lot of people who could really benefit from getting boosted but have not done so,” she added.
Houston Methodist is reporting an early increase in flu cases, with numbers hitting levels not usually seen until the end of the year.
The hospital recorded 100 cases of influenza A and B in the week ending Sept. 21. A week prior, this figure hit 226.
“We experienced an early uptick in mid-September, which relaxed some last week, but still these are the sorts of numbers we usually see in December, not now,” Wesley Long, MD, PhD, a pathologist and medical director of diagnostic microbiology at Houston Methodist, tweeted Sept. 26.
Texas is the only state in the U.S. — outside of Washington, D.C. — that already has a moderately high rate of flu cases, according to the CDC’s latest weekly flu report published Sept. 23.
The early rise in cases comes amid warnings that this season’s flu season may be severe.
New York Gov. Kathy Hochul on Sept. 9 declared a state of emergency amid evidence that polio is spreading in communities around the state. The move unlocks federal resources to help the state respond and boost vaccination rates.
Under the declaration, pharmacists, emergency medical personnel and midwives can now administer polio vaccines. The executive order also requires providers to send polio vaccination data to the state’s health department.
“On polio, we simply cannot roll the dice,”said Mary Bassett, MD, health commissioner at the state’s health department. “If you or your child are unvaccinated or not up to date with vaccinations, the risk of paralytic disease is real. I urge New Yorkers to not accept any risk at all.”
The declaration came the same day state health officials reported that the virus had been detected in wastewater samples from Nassau County. Officials have also found the virus in sewage samples from New York City, Orange County, Sullivan County and Rockland County, where the nation’s first polio case in nearly a decade was confirmed July 21 in an unvaccinated man. Health officials have suggested the Rockland County case may just be the “tip of the iceberg” with hundreds of other cases potentially going undetected in the state.
The threat of polio’s resurgence is magnified by the many pockets of unvaccinated residents throughout the state. New York’s polio vaccination rate is 78.96 percent. That figure is lower in many of the counties where the virus has been detected in wastewater. In Rockland County, for example, the polio vaccination rate is 60.3 percent, state data shows. Nationwide, polio vaccination coverage sits at about 93 percent, according to the CDC.
One of China’s biggest cities, Chengdu, announced a lockdown of its 21.2 million residents as it launched four days of citywide Covid-19 testing, as some of country’s most populous and economically important urban centers battle outbreaks.
All residents in Chengdu, the capital of Sichuan province, were ordered to stay largely at home from 6 p.m. on Thursday, with households allowed to send one person per day to shop for necessities, the city government said in a statement.
The southwestern Chinese metropolis of Chengdu announced a lockdown of its 21.2 million residents as it launched four days of citywide Covid-19 testing, as some of the country’s most populous and economically important cities battle outbreaks.
Residents of Chengdu, the capital of Sichuan province, were ordered to stay home from 6 p.m. on Thursday, with households allowed to send one person per day to shop for necessities, the city government said in a statement.
Chengdu, which reported 157 domestically transmitted infections on Wednesday, is the largest Chinese city to be locked down since Shanghai in April and May. It remained unclear whether the lockdown would be lifted after the mass testing ends on Sunday.
Other major cities including Shenzhen in the south and Dalian in the northeast have also stepped up Covid restrictions this week, ranging from work-from-home requirements to the closure of entertainment businesses in some districts.
The moves curtail the activities of tens of millions of people, intensifying the challenges for China to minimize the economic impact of a “dynamic-zero” Covid policy that has kept China’s borders mostly shut to international visitors and make it an outlier as other countries try to live with the coronavirus.
Most of the curbs are intended to last a few days for now, although two provincial cities in northern China have extended curbs slightly beyond initial promises.
Chengdu’s lockdown sparked panic buying of essentials among residents.
“I am waiting in a very long queue to get in the grocery near my home,” 28-year-old engineer Kya Zhang said, adding that she was worried about access to fresh food if the lockdown is extended.
Hwabao Trust economist Nie Wen said that because Chengdu acted quickly to lock down, it was unlikely to see a repeat of Shanghai’s two-month ordeal.
Non-essential employees in Chengdu were asked to work from home and residents were urged not to leave the city unless needed. Residents who must leave their residential compounds for hospital visits or other special needs must obtain approval from neighborhood staffers.
Industrial firms engaged in important manufacturing and able to manage on closed campuses were exempted from work-from-home requirements.
Sweden’s Volvo Cars said it would temporarily close its Chengdu plant.
Flights to and from Chengdu were dramatically curtailed, according to Flight Master data. At 10 a.m. local time (0200 GMT) on Thursday, it showed 398 flights had been canceled at Shuangliu Airport in Chengdu, with a cancellation rate of 62%. At Chengdu’s Tianfu Airport, 79%, or 725 flights, were canceled.
Shenzhen curbs
In Shenzhen, which has the third-highest economic output among Chinese cities, the most populous district Baoan and tech hub Nanshan suspended large events and indoor entertainment for a few days and ordered stricter checks of digital health credentials for people entering residential compounds.
Nanshan is home to internet giant Tencent and the world’s biggest dronemaker, DJI, among other major Chinese companies.
More than half of Shenzhen’s ten districts, home to over 15 million people, have ordered blanket closure of entertainment venues and halted or reduced restaurant dining for a few days, with curbs in two districts initially planned to be lifted by the end of Thursday.
Shenzhen authorities have largely avoided shutting down offices and factories as they did during a week-long lockdown in March.
Data on Thursday showed that Chinese factory activity contracted for the first time in three months in August amid weakening demand, while power shortages and fresh Covid-19 flare-ups disrupted production.
In Shanghai, schools reopened on Thursday after being closed for months.
Mainland China has reported no Covid death since May, leaving the death toll at 5,226.
The Food and Drug Administration (FDA) on Wednesday authorized updated COVID-19 booster shots specifically targeting a subvariant of omicron.
The move comes ahead of a fall campaign to give Americans booster shots, which is expected to launch in the coming days.
The move marks the first time the vaccines have been updated since the first shots were cleared at the end of 2020, and the updated shots are designed to catch up to evolutions in the virus.
The shots from Pfizer and Moderna target the omicron subvariants BA.4 and BA.5, as well as the original virus.
The shots can begin going into arms once the final step in the process, a Centers for Disease Control and Prevention committee, clears them, which is expected to occur on Thursday.
A major question, though, is how many people will actually want the new shots, given that uptake for the existing booster shots has lagged.
Only about half of people who got the first two shots received the initial booster dose.
“The COVID-19 vaccines, including boosters, continue to save countless lives and prevent the most serious outcomes (hospitalization and death) of COVID-19,” said FDA Commissioner Robert Califf. “As we head into fall and begin to spend more time indoors, we strongly encourage anyone who is eligible to consider receiving a booster dose with a bivalent COVID-19 vaccine to provide better protection against currently circulating variants.”
Seeking to keep up with the ever-evolving virus, the FDA did not wait for the time-consuming process of going through full clinical trials on this tweaked vaccine. But it noted that it is highly confident that the vaccines are safe and effective. The agency pointed to the millions of doses of the original vaccines that have been given, as well as data from another version of the updated vaccine, along with preliminary data on this one.
Peter Marks, a top FDA vaccine official, compared the process to the annual updates to the flu vaccine that seek to adapt to the changes in that virus.
“The public can be assured that a great deal of care has been taken by the FDA to ensure that these bivalent COVID-19 vaccines meet our rigorous safety, effectiveness and manufacturing quality standards for emergency use authorization,” Marks said.
The updated Moderna vaccine is cleared for people 18 and older, and the Pfizer vaccine for people 12 and older.
For both, people are eligible for the booster shot of the updated vaccine if it has been at least two months since their last shot.
The virus has likely been circulating in U.S. cities intermittently for years, experts say.
The fact that poliovirus was detected in New York City wastewater samples as far back as April of this year shouldn’t be surprising, as the virus likely has been circulating for longer and more widely than previously believed, several experts told MedPage Today.
“I think you’re gonna see over the next weeks more and more reports of poliovirus in wastewater elsewhere,” said Vincent Racaniello, PhD, a virologist at Columbia University in New York City.
Poliovirus probably still circulated in the U.S. after 2000, when officials stopped giving the oral polio vaccine, he said. That version protects against paralysis and provides short-term protection against intestinal infection from poliovirus.
The transition to injectable polio vaccine, which is equally as effective against paralysis but not against intestinal infection, meant that the U.S. population was more susceptible to transmitting vaccine-associated poliovirus, he explained.
This circulation is likely occasional and sporadic, he said, but the threat to vulnerable populations is still high.
“Here’s the thing: polio is here in the U.S. It’s not gone,” Racaniello said. “It’s in the wastewater. It could contaminate you, so if you’re not vaccinated, that could be a problem.”
Calls for Nationwide Surveillance
Racaniello said there’s value in learning more about the circulation of the virus, especially for communities with low vaccination rates.
The first step to understanding how long and how broadly poliovirus is circulating, he said, is to start testing wastewater everywhere. The CDC used stored wastewater from April to confirm that the virus had been circulating then, but it is just as possible to conduct nationwide surveillance for poliovirus now, he noted.
In fact, Racaniello said, he has long believed that this kind of surveillance should be done routinely to provide an early detection system for poliovirus.
“Ten years ago, I said to the CDC, you should really be looking in the sewage for poliovirus because of this issue where it could come in from overseas and be in our sewage,” he said. “If someone is unvaccinated, that would be a threat to them, but [the CDC] never did it.”
Davida Smyth, PhD, of Texas A&M University-San Antonio, pointed out that the National Wastewater Surveillance System (NWSS) was established to detect COVID-19 in 2020, so the infrastructure to conduct a wide search for the spread of polio is available.
The primary issue, she said, is that the collaboration that academic researchers have enjoyed with the CDC in surveillance of COVID-19 is so far absent with poliovirus.
“I imagine the CDC is testing those samples for polio, even as we speak, given the nature of what has happened,” Smyth said.
Better coordination with academia and better surveillance, she said, is crucial for finding any potential pockets of poliovirus circulating in other communities around the U.S.
In fact, she said, she is “absolutely convinced” that more polio will be found in the coming weeks.
MedPage Today contacted the CDC to ask whether there are plans to use the NWSS to look for polio around the U.S., but as of press time had not received a response.
Smyth noted that most areas in the country have high rates of polio vaccination, but she is concerned about pockets of rural America where vaccination has dipped in recent years.Most states boast polio vaccination rates over 90%, but Smyth said in some regions, the percentages may be as low as the mid-30s.
“[In] the vast majority of the United States, the vaccination rates are quite high, but the COVID pandemic has led to a decrease in vaccination rates,” Smyth told MedPage Today. “The rates are going down. They’re dipping below 90%, which is shocking, frankly.”
Smyth said the decline is largely due to a lack of opportunity or access to healthcare in some areas, but vaccine hesitancy around the COVID-19 vaccine might be affecting polio vaccinations as well.
“There’s a variety of reasons why people don’t get vaccinated,” she said. “The problem is children are very vulnerable. So if you have a population where the vaccination rates drop, those are exactly the kinds of areas where we need to do this surveillance.”
Racaniello echoed the importance of polio vaccination in adults as well. If patients don’t have a record of their shot, “just vaccinate them,” he said, “because there’s no downside to getting vaccinated again.”
Re-evaluating the Polio Endgame
The recent case of paralytic polio infection and concerns over the wider circulation of poliovirus have also altered some of the thinking around the goal of polio eradication.
In fact, William Schaffner, MD, of Vanderbilt University Medical Center in Nashville, highlighted the unique difficulty of preventing the spread of poliovirus.
“As you can imagine, we’ve gotten into polio endgame,” he told MedPage Today. “I think the notion has now been modified. Eradication isn’t going to be as neat and clean and quick as we once thought. Once we get rid of all paralytic disease, we will have to keep vaccinating for a long time, because there will still be circulating vaccine-associated viruses — some of which will mutate back.”
Schaffner compared the final push to eradicate polio with the successful eradication of smallpox. When the last case of smallpox ended, he explained, public health officials were able to end smallpox vaccination campaigns. For polio, however, he said, it will likely not be that simple, and it will be necessary “to keep vaccinating for quite a long time.”
He said that as public health officials in the U.S. and globally continue to grapple with the nuances of eradicating poliovirus, healthcare providers and their patients will have to come to terms with the simple fact that polio is a real health concern.
“[It’s] the reverse of the old saying, ‘it’s gone, but not forgotten,'” Schaffner said. “Polio is forgotten, but it’s not gone.”
This week, the Food and Drug Administration (FDA) announced a change intended to stretch out the limited supply of monkeypox vaccine doses, allowing the shots to reach five times the number of patients. Monkeypox, a disease in the smallpox family, is spread primarily through skin-to-skin contact, often causing patients to develop painful lesions.
Although most cases resolve within a few weeks, the rapid growth in cases, now more than 9K domestically and 30K globally, is still a cause for concern, leading federal officials to declare a public health emergency last week. The FDA is also recommending that providers administer the vaccine between layers of skin, rather than below the skin into fatty tissue. This dosing change will allow providers to extend the nearly half a million doses not yet sent to states, in order to reach the more than 1.6M Americans considered highest risk.
The Gist: The country is now dealing with two public health emergencies from highly contagious diseases simultaneously. While monkeypox isn’t nearly as transmissible, deadly, or overwhelming to the healthcare system as COVID, the public health response has nonetheless been lackluster (and this week’s new COVID guidance suggests that the CDC has largely given up on managing the response, devolving responsibility to individuals in nearly all settings).
For those hoping that the COVID experience would spark faster action by our public health system, the federal response to monkeypox shows we haven’t applied the lessons learned. Public health authorities aren’t conducting rigorous disease surveillance, testing and treatments remain hard to get, and Congress isn’t dedicating funds for the response. The lack of proactive leadership is likely to result in healthcare providers again bearing the brunt of efforts to manage another unsuppressed viral outbreak.
The monkeypox virus typically spreads through direct contact with respiratory secretions, such as mucus or saliva, or skin lesions. Skin lesions traditionally appear soon after infection as a rash – small pimples or round papules on the face, hands or genitalia. These lesions may also appear inside the mouth, eyes and other parts of the body that produce mucus. They can last for several weeks and be a source of virus before they are fully healed. Other symptoms usually include fever, swollen lymph nodes, fatigue and headache.
I am an epidemiologist who studies emerging infectious diseases that cause outbreaks, epidemics and pandemics. Understanding what’s currently known about how monkeypox is transmitted and ways to protect yourself and others from infection can help reduce the spread of the virus.
How is this outbreak different from prior ones?
The current monkeypox epidemic is a bit unusual in a few ways.
First, the sheer scope of the current epidemic, with over 25,000 cases worldwide as of early August and in countries where the virus has never appeared, sets it apart from previous outbreaks. Monkeypox is endemic to specific areas in central and western Africa, where cases occur sporadically and outbreaks are usually contained and quickly burn out. In the current outbreak, global spread has been rapid. Young men, mostly ages 18 to 44, account for the majority of cases, and over 97% identify as men who have sex with men (MSM). Some superspreading events associated with air travel, international gatherings and multiple-partner sexual encounters contributed to early transmission of the virus.
Second, the way symptoms are appearingmay facilitate spread among people who don’t yet know they are infected. Mostpatients reported mild symptoms without fever or swollen lymph nodes, symptoms that typically appear before a skin rash is visible. While most people do develop skin lesions, many reported having only a single papule that was often obscured inside a mucosal area, such as inside the mouth, throat or rectum, making it easier to miss.
A number of people reported no symptoms at all. Asymptomatic infections are more likely to go undiagnosed and unreported than those with symptoms. But it is not yet known how asymptomatic individuals may be contributing to spread or how many asymptomatic cases may be undetected so far.
Who is at risk of getting monkeypox?
For most people, the risk of getting monkeypox is currently low. Anyone who has prolonged, close contact with an infected person is at risk, including partners, parents, children or siblings, among others. The most common settings for transmission are within households or health care settings.
Because of sustained transmission within the community of men who have sex with men, they are considered an at-risk group, and targeted recommendations can help allocate resources and limit transmission. While monkeypox is spreading primarily among MSM, this does not mean that the virus will remain confined to this group or that it won’t jump to other social networks. The virus itself has no regard for age, gender, ethnicity or sexual orientation.
Anyone who comes into direct contact with the monkeypox virus is at risk of being infected.New cases are recorded daily, with additional countries and regions reporting their first cases and already affected countries observing a continued rise in infections.
As with most infections, other factors, such as the amount of viral exposure, type of contact and individual immune response, play a role in whether an infection takes hold.
Is monkeypox an STI?
While sexual encounters are currently the predominant mode of transmission among reported cases, monkeypox is not a sexually transmitted infection. STIs are spread primarily through sexual contact, while monkeypox can spread through any form of prolonged, close contact.
Close contact that transmits the monkeypox virus involves encounters that are typically more intimate or involved than having a casual conversation or standing next to someone in an elevator. Transmission requires exchange of mucosal fluids or direct contact with the virus in sufficient quantity to seed an infection. This could occur through physical contact during kissing or cuddling.
Because sexual encounters involve direct skin-to-skin physical contact where bodily fluids may be exchanged, these close encounters can transmit viruses more easily. Recently, monkeypox DNA has been detected in feces and various body fluids, including saliva, blood, semen and urine. But the presence of viral DNA does not necessarily mean that the virus can infect someone else. Transmission from these sources is still under investigation.
As the virus moves through populations, public health officials focus on getting the message out to the most at-risk and hardest hit communities about how to stay safe. Currently, breaking the transmission chain among sexual contacts is a priority, including but not limited to MSM communities. Targeted messaging is meant to protect the health of a specific group, not to stigmatize the intended audience.
Other modes of transmission may play a greater role outside the MSM community. Household transmission, where individuals may come into close contact with infected people or contaminated items, is one of the most common types of exposure. Research is ongoing into the potential airborne and respiratory droplet spread of monkeypox in the current situation.
Outbreaks are dynamic situations that evolve over time, which is why public health messages may change as the epidemic progresses. Not every outbreak looks or behaves the same way – even pathogens seen in previous outbreaks can be different the next time around. As researchers learn more about how the disease is transmitted and identify changes in patterns of spread, public health officials will provide updates about specific forms of contact, behaviors or other factors that could increase infection risk. While changing guidelines can be frustrating or confusing, keeping up to date with the latest recommendations can help you protect yourself and stay safe.
What do I do if I’ve been exposed to monkeypox?
Anyone who has been infected can help contain spread by isolating from others, including pets. Covering skin lesions, wearing a mask in shared spaces and decontaminating shared surfaces or items, such as bed linens, dishes, clothes or towels, can also reduce spread.
You can also help interrupt the transmission chain by participating in contact tracing, notifying public health officials of others who may have been exposed through you, which is a basic tenet and common practice of disease control.










_(33114415716).jpg#/media/File:Human_Respiratory_Syncytial_Virus_(RSV)_(33114415716).jpg){kind=link}
{kind=link}