
https://www.axios.com/coronavirus-lessons-other-countries-24794264-1653-4500-922c-7f1c66efa011.html
The countries that have most successfully fended off the novel coronavirus have mainly done it with a combination of new technology and old-school principles.
Why it matters: There’s a lot the U.S. can learn from the way other countries have handled this global pandemic — although we may not be able to apply those lessons as quickly as we’d like.
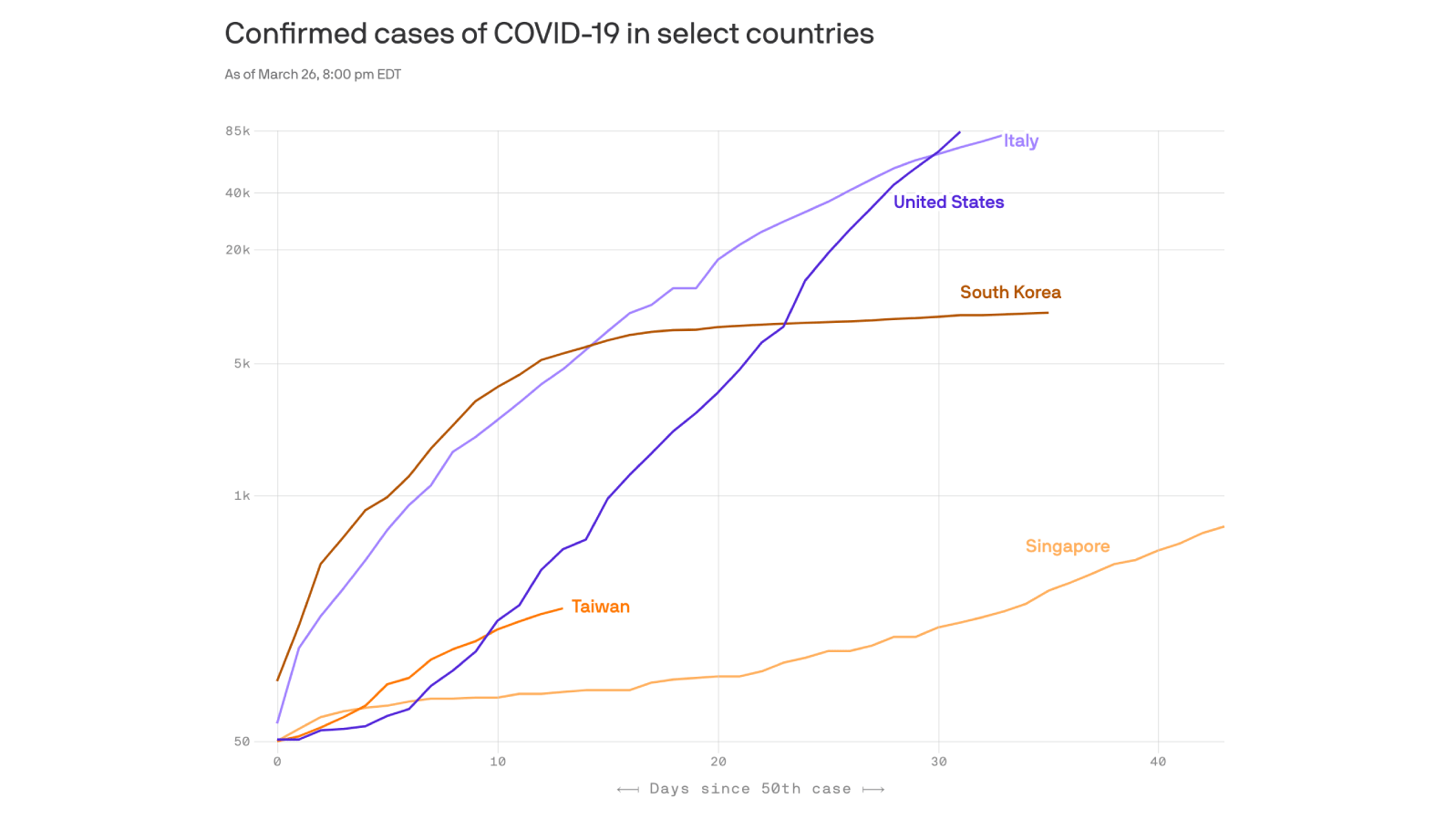
The big picture: A handful of Asian countries, including South Korea, Singapore and Taiwan, have succeeded where the U.S. and Europe have failed.
- They were able to quickly bring the virus under control, reducing the number of new cases that cropped up each day. And they did it largely without shutting down schools, businesses and public life.
The bad news: It’s too late for the U.S. to simply do what worked in those countries. We’ve already made too many mistakes.
- But there are still lessons for the U.S. to learn for future outbreaks — and, hopefully, there are some pieces of those countries’ larger strategies that we can adapt to our coronavirus response now.
Lesson 1: The playbook works
As a new infection begins to spread, you want to quickly test the people who might have it, and quarantine the ones who do. Then you want to figure out who else they might have infected, and test those people, and quarantine the ones who are indeed sick. This process gets repeated.
- “If you don’t know what your population is that you’re supposed to be monitoring, you don’t have a chance,” said Claire Standley, an infectious-disease expert at Georgetown University’s Center for Global Health Science and Security.
This test-and-trace process is nothing new. It’s the standard playbook. South Korea, Singapore and Taiwan just executed it a lot better than the United States.
- Testing and contact tracing are particularly important with this strain of coronavirus because people can spread it before they start to feel sick — so if you’re only testing the sickest patients, the virus is still spreading unchecked.
- And it’s important to do this early. It’s a lot easier to stop five people from infecting another 15 than it is to stop 20,000 people from infecting another 60,000.
Next time a mysterious virus starts spreading abroad, better testing and a much faster response will be imperative.
Lesson 2: Technology can help
Singapore has gotten pretty draconian with its track-and-trace process.
- The government tracks the location of residents’ smartphones, so it knows exactly who had come within a few feet of an infected or potentially infected person.
- It uses the same location data to help enforce mandatory quarantines.
That might be too Big Brother for the U.S., but a voluntary version of it might work — we already consent to a whole lot of location tracking for much less important ends.
- And researchers are already using population-level smartphone data to see, for example, which cities are flouting stay-at-home orders. That can help inform local response even without individualized tracking.
- “I think we’re further along that pathway than maybe people think,” Standley said.
Taiwan, meanwhile, aided its coronavirus response by making better use of data it already had. It quickly merged its immigration and health care databases, giving authorities a real-time view of who was getting sick and where they had traveled.
- That might be hard to copy in the U.S., though, because the relevant data are scattered across multiple local, state and federal agencies with little to no integration. And we have no centralized health data.
Lesson 3: Messaging matters
Public communication is one of the big things Italy — a leading example of what not to do — got wrong.
- Some Italian officials downplayed the virus for too long. Leaders often contradicted each other, and sometimes themselves, about piecemeal interventions before finally locking down the entire country as cases skyrocketed.
Singapore, by contrast, came out early with a clear message: This was going to be bad for a while, and people needed to stick together and do their part.
The U.S., so far, looks a lot more like Italy.
- President Trump has sent similarly mixed messages here, initially downplaying the virus and saying it would go away on its own before changing his tone as cases mounted.
What’s next
The U.S. can’t go back in time to get things right at the beginning. So we can’t match the success of places like South Korea.
- Our best backup plan is to stick with aggressive social distancing and give our testing capacity more time to ramp up.
- We don’t seem to be on track to ever achieve the kind of sophisticated track-and-trace programs Asia employed, but hopefully some cruder version can help us find our way out of this if we keep the number of new cases low in the meantime.
The bottom line: “If we had got on top of this thing two months ago, America would look very, very different,” Ashish Jha, director of Harvard’s Global Health Institute, said in a recent interview with the New Yorker.



