Cartoon – I got the Tin Health Plan



GE announced Tuesday it would separate GE Healthcare into a standalone company and use the proceeds from the sale to pay down its debts.
S&P Global Ratings responded to the news by placing GE’s “A” long-term rating on CreditWatch with “negative implications.”
“GE’s divestiture of its core healthcare segment leaves the company with less business diversity, earnings and cash flow and as such, potential for heightened volatility in profits and cash flow. However, debt reduction and substantial cash balances will reduce balance sheet risk,” S&P said.
John Flannery, chairman and CEO of GE, said in a media release that the spin-offs would “improve our operations and balance sheet as we make GE simpler and stronger.”
“Today’s actions unlock both a pure-play healthcare company and a tier-one oil and gas servicing and equipment player,” Flannery said.
“We are confident that positioning GE Healthcare and BHGE outside of GE’s current structure is best not only for GE and its owners, but also for these businesses, which will strengthen their market-leading positions and enhance their ability to invest for the future, while carrying the spirit of GE forward,” he said.
Kieran Murphy, president and CEO of GE Healthcare, will continue to lead the standalone company under the GE brand.
“As an independent global healthcare business, we will have greater flexibility to pursue future growth opportunities, react quickly to changes in the industry and invest in innovation,” Murphy said.
“We will build on strong customer demand for integrated precision health solutions and great technology with digital and analytics capabilities as we enter our next chapter,” he said.
GE Healthcare’s core business is medical imaging, monitoring, and other high-tech hospital equipment. The company does business in 140 countries.
The sell-offs are expected to be completed over the next 12 to 18 months.
The ongoing efforts to destabilize the Affordable Care Act will adversely affect the operating margins of not-for-profit healthcare providers, according to a new analysis from S&P Global.
S&P analyst Allison Bretz said that over time, “a growing uninsured population could be a credit negative for not-for-profit hospitals and health systems, as these facilities would likely see an uptick in self-pay patients, charity care and bad debt.”
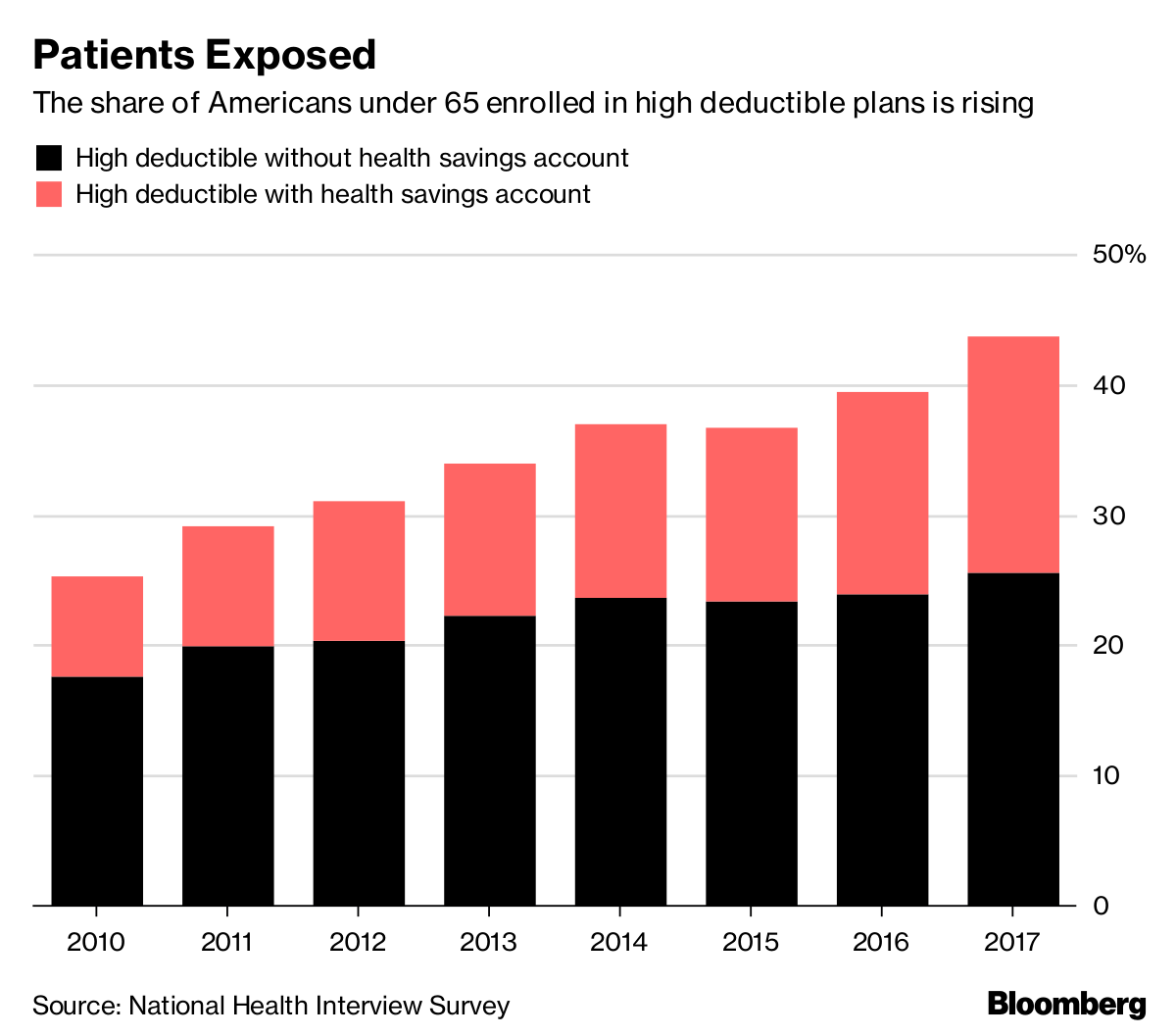
Two years into the Trump administration’s efforts to roll back the ACA, the uninsured population has risen from about 12.7% in 2016 to 15.5% in 2018.
A study by The Commonwealth Fund estimates that 4 million people have lost health insurance since 2016, and that the uninsured rate among lower-income adults rose from 21% in 2016 to 25.7% this spring.
“This will be most acute at safety-net providers and other providers with a high concentration of Medicaid patients, as that population is most vulnerable to many of these changes,” Bretz said in remarks accompanying the report.
Beth Feldpush, senior vice president of policy and advocacy for America’s Essential Hospitals, said the report “underscores concerns we’ve had since last year’s attempts to repeal the ACA and, now, with piecemeal changes that have weakened the law.”
“Many of the people who lose coverage seek care at our hospitals, which adds to uncompensated costs and puts more pressure on our members’ already low operating margins,” Feldpush said. “Because essential hospitals, by their mission, turn no one away, this could prove financially unsustainable for some.
Although active efforts to repeal the ACA in Congress have slowed in the past year, it is facing one of its greatest threats, as a federal judge in Texas hears a lawsuit brought by 20 states that challenges the constitutionality of the sweeping healthcare law.
For-profit, Payer Outlook Stable
While the rising uninsured rate could prove challenging for not-for-profit providers, S&P analyst David Peknay said it should have little effect on for-profit providers.
“The for-profit companies we rate have been reporting some increase in uninsured patients, consistent with national trends, but the impact on ratings is also currently immaterial,” he said.
The losses in covered lives for health insurance companies is offset by other factors, said S&P analyst Joseph Marinucci.
“A key contributing factor is the sustained migration of the government-sponsored insurance segments toward coordinated care (Medicare Advantage and managed Medicaid), which is expanding the market opportunity for health insurers,” Marinucci said.
“We expect ratings in the insurance sector to remain relatively stable in the near term despite the growth in the number of working-age uninsured individuals,” he said.
https://www.healthcaredive.com/news/more-medicare-patients-dying-at-home-jama-study-finds/526477/

Although most Americans over 65 say that they’d prefer to die at home, in 2009 only 24% of them actually did. Yet, in recent years, more and more Americans are choosing to live out their last days in their home or community instead of being admitted to a hospital.
The JAMA study reveals a potential patient response to the current inadequacy of end-of-life care as, for some older Americans, ending up in a hospital can mean high-cost and aggressive treatment in their final days.
Such treatment does not always equal better care. When it comes to their elderly patients, incumbent healthcare systems increasingly specialize in expensive, often unnecessary services as opposed to a value-based approach.
The findings come on the tide of the so-called “silver tsunami” as the American population skews ever older. The number of Americans aged 65 or older is projected to more than double by 2060, when they will eventually account for 24% of the total population.
New startups have emerged looking to address the institutional inadequacy of end-of-life care, viewing the aging population as a business opportunity. The growing companies zero in on technology-driven solutions in home health, chronic illness and end-of-life care as they look to scale to combat industry issues.
Such startups are a potential wake-up call for traditional healthcare organizations.
“Innovation comes from the private sector,” Teno, a professor of medicine at the University of Washington, told Healthcare Dive.
“I think the implication of this is that hospitals are going to have to change how they’re practicing. They’re going to have to come into new population-based business models that don’t have their entire survival based on their number of admissions,” she said.
On the hospital side, Teno called for multifaceted interventions that address the issue of care overuse and fragmentation in hospitals, such as care bundling and coordination, surveys measuring patient satisfaction and public reporting of readmission rates.
Despite the challenges, Teno was optimistic about study’s implications.
“We’re on the right path,” she said. “We need to wean ourselves off of this fee-for-service world of paying for a procedure and paying for volume, to paying for value.”
“The fee-for-service world provides perverse incentives,” Teno stressed, also noting that it tends to lead to hospital disorganization and miscommunication.
Teno cited the growth of Medicare Advantage as a program (it accounts for a third of Medicare enrollees and spending), and the 9.3% difference in hospitalization rates between MA and fee-for-service as a good sign for the future of healthcare.
Health insurance is complicated. In many states, it’s about to get worse.

Where states allow short-term plans without restriction, the plans will be a lot cheaper than those sold on the exchanges because they don’t have to comply with the ACA. But that low price comes with big tradeoffs.
Short-term plans don’t have to sell to all comers, nor do they have to cover pre-existing conditions. Sick people will have no real choice but to buy insurance on the exchanges. To cover the medical costs of a relatively sicker group of people, exchange insurers will have to increase their premiums.
People who earn less than four times the poverty level will be shielded from the price increases because the ACA caps premiums at no more than about 10% of income. The federal government, however, has to pick up the rest of the tab-so as prices go up, federal outlays will, too, squandering an estimated $38.7 billion over 10 years.
Hurt worst will be people who earn more than four times the poverty level. Federal actuaries estimate that they’ll pay 6% more on account of the short-term rule by 2022. That will come on top of price increases associated with Congress’s repeal of the individual mandate. In 2019 alone, the Urban Institute predicts that insurance prices will grow, on average, by about 18%.
Beyond that, people who buy short-term plans may be surprised to discover just how stingy they are. Insurance is complicated: people rarely read, much less understand, all the fine print. And there’s a lot of fine print.