Forbes last month released its second-annual “America’s Best Companies” list, recognizing 500 companies, including 44 healthcare companies — several of which are Advisory Board members.
For the list, Forbes looked at public and private companies as well as foreign-based companies with a U.S. subsidiary and analyzed more than 100 metrics across 11 categories. Companies with U.S. headquarters that employ more than 7,000 people in the United States were eligible for the list.
The primary categories Forbes looked at, and the data partner it worked with, were:
Employee sentiment (Glassdoor), where workers rated their company in categories like career opportunities, compensation and benefits, and confidence in senior leadership.
Customer sentiment (HundredX), where consumers rated products they purchased in categories like customer service, value, and dozens more.
Financial performance (Forbes), which looked at one- and five-year metrics for stock prices and revenue growth.
Business trajectory (Crunchbase), which assessed metrics that consider dozens of financial indicators like funding, market share and movements, and company growth.
Cybersecurity (SecurityScorecard), which assessed categories like network and applications security, malware vulnerability, and regularity of patches.
Media sentiment (SignalAI), which reviewed positive and negative company coverage of executive leadership, innovation, diversity performance, and financial performance.
Workforce diversity (Denominator), which assessed representation at both executive and lower levels of the company of different groups, including gender, race/ethnicity, age, education, disability, and nationality.
Sustainability (Morningstar), which assessed the robustness of climate governance, sustainability strategy, risk management, and financial and competitive strength.
Workforce stability (People Data Labs), which looked at each company’s workforce growth rate, churn rate, and average C-suite tenure.
Company size (Data Axle), which looked at each company’s number of U.S. employees.
Each company received an individual category score that was normalized and adjusted where appropriate to reflect how that score compared to competitors in their sector. Those scores were then combined to create a final score to develop the rankings.
The best healthcare companies in the US
In the drugs & biotechnology industry, the companies recognized on the list were:
87. AbbVie* (Chicago, IL)
119. Johnson & Johnson* (New Brunswick, NJ)
164. Amgen (Thousand Oaks, CA)
235. Gilead Sciences (Foster City, CA)
280. Merck & Co. (Kenilworth, NJ)
394. Thermo Fisher Scientific (Waltham, MA)
460. Zoetis (Parsippany, NJ)
477. Biogen* (Cambridge, MA)
*Denotes an Advisory Board member
In the healthcare equipment & services industry, the companies recognized on the list were:
146. GE HealthCare Technologies (Chicago, IL)
331. Ansell Healthcare (Iselin, NJ)
357. Alcon Vision (Fort Worth, TX)
384. Henry Schein* (Melville, NY)
395. Herbalife International of America (Los Angeles, CA)
409. Home Life Care (Ahoskie, NC)
415. Zimmer Biomet* (Warsaw, IN)
422. Smith & Nephew (Memphis, TN)
442. Chemed (Cincinnati, OH)
443. Encompass Health* (Birmingham, AL)
497. Merrill Gardens (Seattle, WA)
*Denotes an Advisory Board member
In the healthcare & social services industry, the companies recognized on the list were:
45. CVS Health (Woonsocket, RI)
275. Northside Hospital* (Atlanta, GA)
309. Main Line Health* (Radnor Township, PA)
374. Oklahoma Heart Hospital (Oklahoma City, OK)
452. Sharp HealthCare* (San Diego, CA)
464. Carle* (Urbana, IL)
468. Henry Ford Health System* (Detroit, MI)
469. Sutter Health* (Sacramento, CA)
475. Virtua* (Marlton, NJ)
484. Cincinnati Children’s (Cincinnati, OH)
492. Harris Health System* (Houston, TX)
*Denotes an Advisory Board member
In the medical equipment & services industry, the companies recognized on the list were:
44. Abbott Laboratories (Chicago, IL)
103. Boston Scientific* (Marlborough, MA)
121. Dexcom* (San Diego, CA)
152. McKesson* (Irving, TX)
200. Intuitive Surgical (Sunnyvale, CA)
219. Stryker* (Kalamazoo, MI)
250. Labcorp Holdings* (Burlington, NC)
286. Cardinal Health (Dublin, OH)
342. Agilent Technologies (Santa Clara, CA)
347. Becton Dickinson* (East Rutherford, NJ)
425. National Vision (Duluth, GA)
436. Quest Diagnostics* (Secaucus, NJ)
*Denotes an Advisory Board member
In the pharmacies industry, the companies recognized on the list were:
Next year, seniors and families will have more stringent and more unaffordable health coverage thanks to new AI-driven prior authorizations in Medicare and loss of subsidies in the ACA.
The New Year is just two weeks away, and when Americans wake after clinking champagne and kissing at midnight, the health care landscape in the United States will be in worse shape than it was in 2025. There is a growing list of why that’s true, but here are a couple of developments that will make it harder for many of us to get the care we need:
The December 31 expiration of the Affordable Care Act enhanced subsidies, which will lead to millions of Americans losing coverage and make premiums barely affordable for millions of others; and
CMS’s January 1 implementation of a new pilot project that will put private, for-profit contractors using AI-powered prior authorization in traditional Medicare.
Unless policymakers change course, many Americans will be ringing in 2026 with higher costs, less access and a nasty health care hangover.
WISeR strikes at 12
As we’ve reported, the implementation of the Wasteful and Inappropriate Service Reduction (WISeR) model’s will mark the first time in traditional Medicare’s 60-year history that for-profit companies will decide whether seniors receive certain medical services their doctors recommend. Six companies — many with deep ties to Big Insurance and insurer-backed venture capital — will suddenly have the power to say yes or no to 17 procedures that never required prior authorization before. And for these companies, the more the denials, the bigger the profits.
As Dr. Seth Glickman documented after sitting through CMS’s own WISeR webinar, the rollout has been vague on details and confusing to providers and patients. CMS even admitted during the webinar that the vendors chosen to administer the model were selected in part based on their “success” of using prior authorization in the private Medicare Advantage program, which is notorious for denials, delays and life altering decisions.
Some lawmakers in Washington have taken notice. A coalition of Democrats introduced the Seniors Deserve SMARTER Care Act, warning that WISeR creates “a dangerous incentive to put profits ahead of patients’ health.” Imposing prior authorization in traditional Medicare “will kill seniors,” said Rep. Mark Pocan, one of the bill’s sponsors.
Kiss subsidies goodbye
While WISeR threatens seniors’ access to care, millions of working families are facing a different New Year’s surprise: the expiration of enhanced ACA marketplace subsidies, which Congress has (so far) failed to extend or replace. As Rachel Madley, PhD wrote in October, families will have to gamble when they pick a health insurance plan. She added:
The enhanced premium subsidies being debated in Congress right now are a lifeline for so many of us and must continue in the short term, but they don’t fix the underlying problem: Private insurers extract value rather than control costs or provide access to necessary and affordable care. Decades of experience show that when profits rule health insurance, families face financial ruin no matter which plan they pick during open enrollment.
But as we’ve noted before, this isn’t an existential crisis for Big Insurance. ACA marketplace plans are not where insurers make their real money. Their profits flow increasingly from taxpayer-funded programs like Medicare Advantage and Medicaid managed care — the same universe WISeR is quietly expanding.
One proposal to “solve” the subsidy issue, endorsed by President Donald Trump and HELP Chairman Bill Cassidy, would not extend the tax credits but put $1000 to $1500 into government-sponsored health savings accounts (HSAs). HSAs can be helpful if you you have crappy insurance – or are rich and need an additional place to put your money to avoid taxes – but not a meaningful solution to the millions of Americans facing a 75% hike in premiums or finding themselves priced out of coverage altogether in 2026. The supporters of this approach claim it would somehow take money away from health insurers, but it would just reroute federal dollars to those same companies. For instance, UnitedHealth Group, which owns the nation’s biggest HSA custodian, could grab even more of our tax dollars than they already do. Meanwhile, families would still be exposed to unaffordable premiums and massive out-of-pocket costs. Champagne dreams.
Thanks to these changes in health care: The hangover on January 1, 2026, won’t only be from the previous night’s festivities – and it won’t be cured with some water and Advil. Cheers.
The OIG found that Anthem paid its own corporate sibling as if it were an outside vendor. The maneuver transformed a cost-based function into a source of “unlimited profit.”
When the Office of Inspector General (OIG) audited Anthem Blue Cross and Blue Shield insurance plans for federal employees recently, auditors appeared to be conducting a typical contract compliance review.
While they may not have been looking for a smoking gun, they stumbled upon one.
At first glance, the report on Elevance Health’s Anthem Blue Cross and Blue Shield insurance under the Federal Employees Health Benefits Program (FEHBP) looks like just another technical review, questioning charges and payments across familiar audit categories such as uncollected claim overpayments, administrative expense overcharges, medical drug rebates, provider offsets and lost investment income. The auditors’ stated goal was to “obtain reasonable assurance” that Anthem was complying with contract terms. The review took a turn from the routine when the OIG looked at how Elevance is using a common insurance practice known as subrogation.
The issue of subrogation emerged after the OIG observed irregularities in recoveries and fees being passed through the plan. Subrogation – recovering costs from insurers, auto carriers or liable third parties – is a familiar function. But the structure Anthem created is not.
Anthem Inc. became Elevance Health Inc. in 2022 and also launched Carelon health services. Elevance became the name of the parent company, but the name Anthem was retained for the health plans the company operates across the country. Carelon, a wholly owned Elevance subsidiary, is a corporate sibling of the Anthem health plan division, and it’s the fastest-growing of the two. In fact, Elevance views Carelon as the company’s profit engine.
The OIG discovered that Anthem treated Carelon as a commercial provider of services in an arm’s length transaction and paid Carelon a percentage of recoveries, even though, as OIG wrote, this was a “related party transaction.” Auditors discovered that Anthem had contracted its subrogation work to Carelon, and then billed the FEHBP a percentage-based “fee,” deducted directly from the recoveries, and recorded it as a health benefit expense rather than an administrative cost. The subrogation fees then passed through FEHBP as medical claims, thereby avoiding oversight limits on administrative costs and creating “unlimited” profit on a function that should have been cost-based.
Self-enrichment
The OIG was especially troubled because the transaction was a “related party transaction,” which in government contracting is the polite way of saying you’re paying yourself. Worse, the OIG found that:
“The method Anthem uses to charge these subrogation recovery fees results in unlimited profits for essentially an ‘in-house’ service…
And that:
“Elevance Health, Anthem, and/or Carelon should not benefit or self-enrich at the expense of the FEHBP.”
The auditors also concluded that:
“… the only profit that can be charged to the FEHBP is the negotiated annual service charge…”
But Anthem had charged $39,235,156 in subrogation fees plus $5,638,360 in lost investment income – exactly the kind of profit the contract prohibits.
What’s most shocking about this audit isn’t what Anthem did – it’s how openly they did it, and how little anyone plans to do about it.
To appreciate the magnitude of the audit discovery, it helps to understand how the Federal Employees Health Benefits Program actually operates – and who really runs it. The FEHBP is a roughly $70billion annual program covering more than eight million federal workers, retirees and dependents. Yet the federal government does not administer these benefits directly. Instead, it contracts with the Blue Cross Blue Shield Association (BCBSA), which then delegates day-to-day administration to individual Blue plans across the country.
Among those plans, Anthem administers services in 14 states – more than any other Blue plan – and during the audit period was responsible for $40.6 billion in FEHBP benefit payments and $2.1 billion in administrative expenses. Anthem isn’t simply one contractor in a crowded field; it is the dominant operational arm of the BCBSA for a vast portion of the federal population. When Anthem selects a vendor, sets payment terms or withholds documentation, it is not a peripheral actor – it is effectively shaping how the federal health plan functions.
What’s worse than getting caught red-handed breaching the contract? The company’s response. Its posture throughout the report is equal parts dismissive, pedantic and openly defiant. It insisted the fees represented “allowable, commercially reasonable charges,” argued that subrogation was a “commercial service,” and maintained that the costs were “not subject to cost analysis.”
The company repeatedly pushed back with formulations that would seem to suggest that Elevance itself, and not the OIG, was the final authoritative voice on contract compliance and legality:
“We disagree with the OIG’s characterization.”
“We do not concur.”
“The services are allowable and reasonable in view of the commercial marketplace.”
When the OIG pressed for documentation to substantiate these so-called “commercially reasonable” fees, they were met with outright refusal. They were told that no such documentation existed. Unfortunately for Anthem, they proved themselves wrong in a meeting with OIG when they inadvertently displayed a detailed spreadsheet showing a cost analysis for corporate subrogation services – the very spreadsheet the company had insisted did not exist. As the OIG noted:
“Anthem inadvertently shared an Excel spreadsheet which included the total corporate Carelon subrogation costs by year – precisely the cost data we have been requesting.”
Rather than simply hand it over, the company declared the spreadsheet “not accurate,” “not relevant,” and “not responsive.”
It gets worse. When the auditors asked for a valuation prepared by the company’s accounting firm, Deloitte – the same valuation Anthem itself relied upon as proof that they had studied the reasonableness of their charges – the company responded by producing six heavily-redacted pages out of a 900-page report. That’sless than 1% of the analysis they claimed fully justified their pricing, which costs the FEHBP over $40 million.
The OIG, in its dry bureaucratic tone, noted that the company’s justification for withholding “over 99 percent of the Deloitte study” was “insufficient” – which is government-speak for, “Are you kidding me?” The OIG all but throws up its hands:
“We cannot determine the actual profit charges and/or the reasonableness of these fees due to the scope limitation created by Anthem’s refusal to provide documentation access.”
Anthem behaves as though the worst that can happen is that someone at OIG writes a sternly worded paragraph in a report that will sit unread on a government website. Unfortunately, they are probably right.
As the OIG delicately put it:
“Throughout the audit process, we encountered numerous instances where Anthem responded untimely and/or initially provided incomplete responses.”
And why would Anthem cooperate? The OIG report is unlikely to trigger meaningful enforcement, the federal Office of Personnel Management has historically acted more like a deferential plan sponsor than a regulator, and Congress appears largely uninterested in disrupting a status quo that serves the BCBSA and its licensees quite well.
62% profit margin
Ultimately, due to the lack of information from Anthem, OIG acknowledged that it was forced to estimate the degree of unallowable profit. Based on the limited corporate subrogation cost data they could see, auditors concluded that Anthem was likely earning a profit margin of approximately 62%.
Think about that: a federal contractor potentially earning a 62% profit margin on a supposedly in-house function, inside a federal health plan that legally prohibits this form of profit.
Discovery of a profit extraction model
All of this is visible only because the OIG happened to expand a limited audit sample into subrogation recoveries. The OIG did not enter the process intending to uncover a profit-extraction model. But it found one.
Which raises the question: what would the numbers look like if OIG examined all subrogation? Or payments for all Carelon services? Or fees related to recovery services, out-of-network negotiation and payment integrity? Or medical management? Or pharmacy recoveries?
The answers are not in the report.
What this audit shows is not just that Anthem crossed a line. It shows that those running the FEHBP lack the power, or the will, to draw one. If a contractor can profit in violation of the contract, get caught, and then simply withhold the evidence and declare they disagree, then the rules are performative and enforcement is imaginary. Anthem’s response – dismissing the OIG’s findings, withholding a 900-page Deloitte report, refusing cost documentation, and asserting a legal right to decide what data the government may review – reflects not caution, but confidence.
Confidence that there will be no consequence. Confidence that the FEHBP cannot or will not act. And, perhaps most troubling, confidence that the American taxpayer will never know the difference.
The contractor knowingly violated profit limits, hid the margin inside claims, refused to provide cost data, and continues billing unchanged. If this is what turns up accidentally, just imagine what would be exposed if anyone actually went looking.
Chris Deacon, JD, is a health care executive and consultant recognized for her advocacy for transparency and accountability. She previously ran New Jersey’s public sector health plan, covering 820k lives.
A striking thing about this week’s flow of news out of the Federal Reserve is how normal it was — at least compared to some of the possibilities that appeared in play last month for a breakdown in the institution’s longstanding norms.
Why it matters:
In the Fed’s decision to cut interest rates on Wednesday, and the unanimous reappointment of 11 of 12 reserve bank presidents announced yesterday, it was clear that Powell has retained his ability to steer a seemingly fractious organization toward consensus.
The next chair may yet shift the institution toward a process with more open dissent and count-the-votes proceduralism, as is seen at the Bank of England and as some Trump associates have advocated.
But for now, Powell looks clearly in charge despite lame-duck status (his term is up in May).
State of play:
Just a few weeks ago, it looked plausible that there would be the most open dissent from the Fed’s December interest rate decision in decades. Five officials of 12 Federal Open Market Committee voting members had expressed significant reservations about a rate cut.
Three officials who were publicly skeptical of cutting rates further — reserve bank presidents Susan Collins (Boston) and Alberto Musalem (St. Louis), and governor Michael Barr — elected to follow the leader when it was time to cast their vote.
While there were three dissents — two opposing the cut, one favoring going further — that’s not terribly abnormal. There were three dissents in September 2019, for example, also in opposite directions.
What they’re saying:
“After the high drama/psychodrama from the October press conference onwards, the end result was more business-as-usual on the part of the Powell Fed,” wrote Krishna Guha and colleagues at Evercore ISI in a note.
In his news conference, “Powell was calm and poised, not on the ropes as in October, with a governance crisis averted,” they wrote.
The big picture:
Fed watchers were braced for the possibility that the every-five-years process of reappointing reserve bank presidents would generate fireworks, an opportunity for Trump-appointed governors to try to create some upheaval at the Fed (or at least make some noise).
It came and went yesterday without signs of public dissent, as the board announced that 11 of 12 reserve bank presidents had been reappointed with “unanimous concurrence” by members of the Board of Governors.
Not only were the 11 officials re-upped, the three Trump-appointed governors did not object.
The odd man out, Atlanta Fed president Raphael Bostic, had previously announced his retirement at the end of his term in February. But one bank president stepping down at the end of a term is not unheard of; it last happened at the end of 2015 with Minneapolis Fed president Narayana Kocherlakota.
Between the lines:
On paper, the Fed chair holds only one vote out of seven on the Board of Governors and one of 12 on the FOMC. Their ability to lead the institution depends on a mix of hard and soft power.
In the hard power department, the chair oversees the staff and sets meeting agendas. In the soft power department, they must persuade their colleagues to line up with the policy path they believe is correct.
Powell has been skilled at using both — and displayed those skills this week.
There’s likely to be one more round of health care votes in the House next week after the Senate votes down two rival Affordable Care Act subsidy proposals Thursday — but they won’t get any closer to extending the enhanced subsidies.
Why it matters:
Those subsidies now appear certain to expire at the end of the year, short of a last-minute breakthrough — and out-of-pocket premium costs will more than double on average for roughly 20 million ACA enrollees.
Driving the news:
The Democratic proposal that will get a Senate vote Thursday would extend the enhanced subsidies for three years, while the Senate GOP proposal would not extend the subsidies but instead provide money for health savings accounts.
Both will fail to get the needed 60 votes.
Senate Majority Leader John Thune (R-S.D.) has left the door open for further bipartisan talks after both votes fail, but there is deep skepticism in both parties that any such deal is possible.
Sen. Tim Kaine (D-Va.) said it’s possible there is “additional discussion” after the failed votes, but said the issue also might end up in a “political solution in November when people pick the side that’s for them.”
The latest:
House GOP leaders outlined a range of possible health care options on Wednesday morning, but they have little to do with the subsidies, which weren’t included in their plans.
GOP leaders will bring “consensus” bills to the floor next weekthat aim to lower health care costs, a source who attended House Republicans’ Wednesday morning conference meeting told Axios.
Those could include expanding health savings accounts and association health plans, which allow employers to band together to purchase coverage.
Overhauling pharmacy benefit managers with the goal of lowering drug costs was also discussed, along with funding ACA payments known as cost-sharing reductions (CSRs).
The intrigue:
On the House side, a bipartisan group of moderates including Reps. Brian Fitzpatrick (R-Pa.) and Jared Golden (D-Maine) filed a discharge petition, a procedural move to force a vote on a compromise extension plan.
But that effort to go around House GOP leadership faces long odds against getting the required majority of the chamber to sign on.
Modifications to the subsidies in that plan designed to win over GOP votes, like a crackdown on zero premium plans that backers say fuel fraud, could lose Democratic support due to concerns about coverage loss.
Democratic leaders havebeen focused on a clean three-year extension, saying that is the clearest way to address the issue with little time remaining to implement changes before the new coverage year starts Jan. 1.
House Democratic Leader Hakeem Jeffries (N.Y.) told reporters Wednesday he has no position on the discharge petition.
The bottom line:
There is also deep resistance to a subsidy extension among many Republicans.
Thune has said he thinks Democratic leadership is more interested in a “political messaging” vote this week than in entertaining reforms to the subsidies that Republicans point to.
Even if members in either chamber are able to make progress on a consensus compromise subsidy plan, which in theory could be attached to a government funding bill needed before Jan. 30, the divisive issue of abortion hangs over all of the discussions.
Many Republicans insist on new limits preventing the subsidies from going to insurance plans that cover abortion. Democrats say that is a dangerous expansion of safeguards that already require taxpayer funds to be segregated and not pay for abortion coverage.
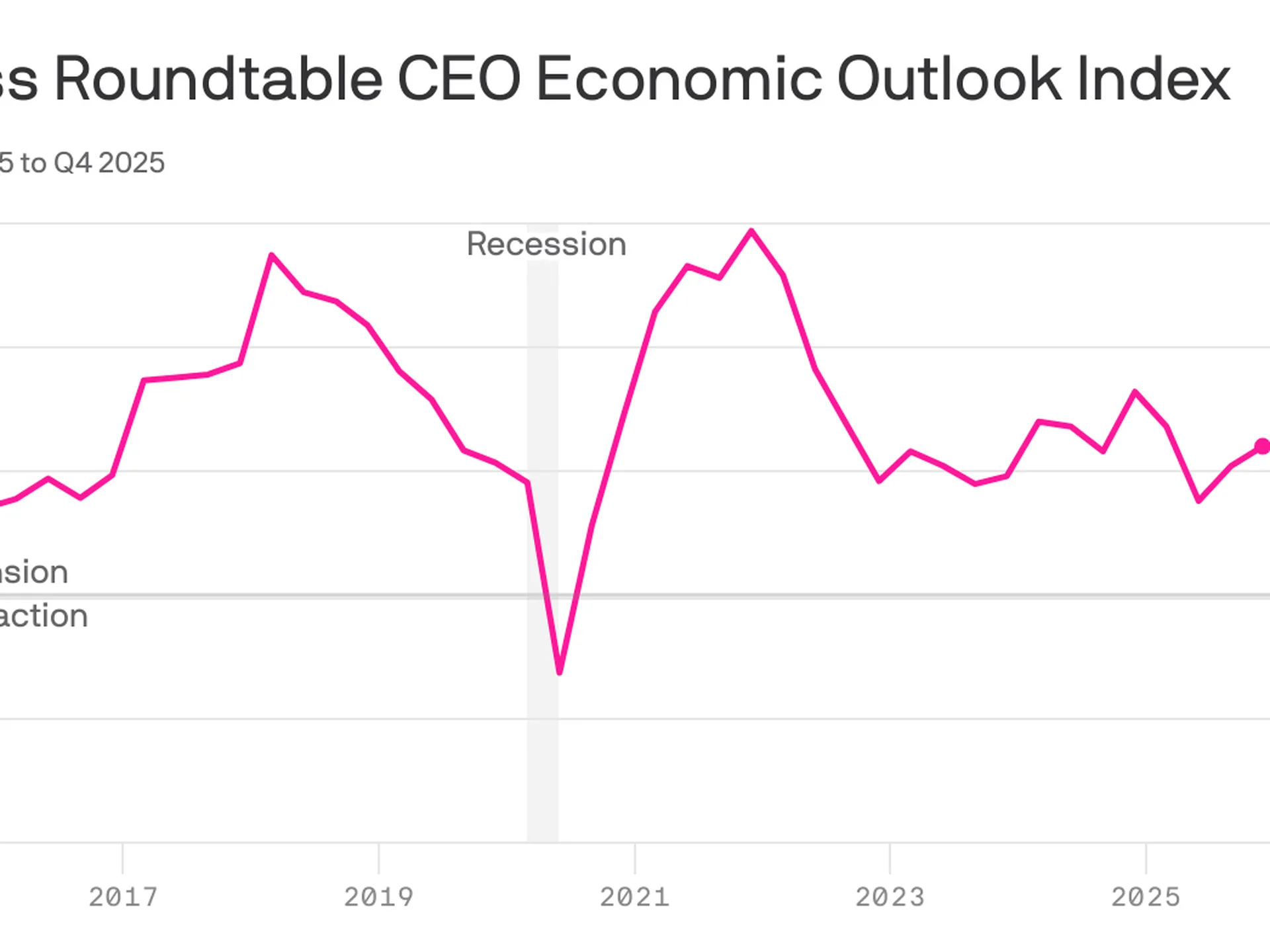
CEO sentiment increasedfor the third consecutive quarter, even as America’s most prominent executives expect underlying job market conditions to remain weak.
Why it matters:
The economic outlook among CEOs has steadily improved since plunging in the aftermath of President Trump’s initiation of the global trade war.
Under the hood, however, there is evidence that structural economic changes — including the proliferation of AI — are weighing on hiring intentions, a warning sign for the labor market.
By the numbers:
The Business Roundtable’s CEO Economic Outlook Index rose by 4 points in its fourth-quarter survey, which was fielded from the final weeks of November through earlier this month.
The index is still shy of the highest level of the Trump 2.0 era and slightly below the historical average of 83.
Zoom in:
The increase reflects a more upbeat view of company revenue in the next six months: Expectations for sales rose 6 points, though the survey does not ask respondents to adjust for the prospect of higher prices.
Plans for capital expenditures — investments in equipment, buildings or software — ticked up 2 points, following a 10-point surge in the previous quarter.
Hiring plans also improved relative to last quarter — up 4 points — though it is the survey’s lone indicator below the level that signals growth.
What they’re saying:
“Notably this quarter, more CEOs plan to reduce employment than increase it for the third quarter in a row – the lowest three-quarter average since the Great Recession,” Business Roundtable CEO Joshua Bolten said in a statement.
About one-quarter of CEOs say they will increase hiring, while 35% say employment will shrink at their respective firms. The remaining 40% plan to keep hiring steady.
A smaller share of CEOs plan to slash workers relative to last quarter, but the figures still show a notable shift among top executives.
Consider the results from this time last year: A similar share of CEOs expected no change in employment levels, but just 21% said they anticipated cutting jobs, while 38% planned to increase hiring.
“CEOs’ softening hiring plans reflect an uncertain economic environment in which AI is driving sizeable [capital expenditures] growth and productivity gains while tariff volatility is increasing costs, particularly for tariff-exposed companies, including small businesses,” Bolten said today.
The big picture:
The in-the-dumps hiring plans signaled by big firm CEOs — alongside a string of layoff announcements in recent months — signal a possible shift for the steady-state labor market that has persisted in recent years.
Powell raised the possibility that the labor market might be even weaker than government data suggests.
The economy has added a monthly average of 40,000 payroll jobs since April. But “we think there’s an overstatement in these numbers, by about 60,000, so that would be negative 20,000 per month,” Powell said at yesterday’s press conference.
“The labor market has continued to cool gradually, maybe just a touch more gradually than we thought,” he added.
The bottom line:
CEOs feel more optimistic, though that confidence boost is not expected to translate into more hiring — an unusual dynamic for the economy.
“Although the results signal that CEOs are approaching the first half of 2026 with some caution, they are starting to see opportunities for growth,” Cisco CEO Chuck Robbins, who chairs the Business Roundtable, said in a statement.
“With the Index near its average, it reflects the resilience of the U.S. economy,” he added, citing pro-growth tax policies and fewer regulations.
Yesterday aboard Air Force One, President Trump was asked by a reporter if he supported Senators Bill Cassidy (R-LA) and Mike Crapo’s (R-IN) new health care proposal, which would authorize $1,500 deposits in Health Saving Accounts (HSAs) for lower-income individuals to replace the expiring Affordable Care Act (ACA) subsidies. The president’s response to the question was telling. And it shows just how much Big Insurance has fallen from grace in recent months.
For decades, merely expressing disenchantment with private health insurers could get you labeled as a socialist. Now we are seeing daily criticism of health insurance companies from people across the political spectrum, leading one to not know if a quote like “Americans are getting crushed by health insurance with monthly payments” is coming from a progressive, like AOC, or a conservative like MTG. (Hint: that quote was from MTG). Trump’s response was in the same vein and could lead one to believe there is a chance of the left and right finding common ground in holding insurance companies accountable for their greed.
Where Trump is right. Where Trump is wrong.
Below we will dissect the president’s response and explain where he’s right and wrong.
“I like the concept [of the Cassidy-Crapo legislation]. I don’t want to give the insurance companies any money. They’ve been ripping off the public for years.“
This is true. Big Insurance has been ripping us off for years. And almost all of insurers’ growth in recent years has come from us as taxpayers. Most big insurers now make far more money on the lucrative Medicare Advantage business and managing state Medicaid programs than from their commercial health insurance plans. And they’ve even figured out how to bilk the VA.UnitedHealthcare, the biggest insurer, now gets more than 75% of its revenues from taxpayer-funded programs. And yes, insurers are getting hundreds of billions of dollars every year from the ACA subsidies that are at the center of debate in Washington.
Here are a couple of examples. Private health insurers took in over $500 billion in tax dollars to administer Medicaid in 2023. And this year alone, they will be overpaid – yes overpaid – $85 billion as a consequence of how they’ve rigged the Medicare Advantage program.
Insurers also take in massive amounts of money in the form of premiums that people pay thinking that money goes to care. Much of that money ends up going toward things (and people) that do nothing to get us well or keep us well. Since 2014, the seven largest insurers have made over $500 billion in profits, and they used $146 billion to buy back their own stock. So yes, Trump is correct, health insurance companies have been ripping people off for years.
“Obamacare is a scam to make the insurance companies rich.”
No, Mr. President, the ACA is not a scam and most Americans now know that it has done a lot of good for a lot of people. Among other things, it made it possible for millions of people who previously had been blackballed by insurers because of a preexisting condition to finally get coverage. It brought us many long-overdue consumer protections, outlawed junk insurance, enabled young people to stay on their parents policies until they turned 26, alleviated job-lock through the creation of the ACA (Obamacare) marketplaces, and it made millions more low-income families eligible for Medicaid.
But, the president is right to say that Big Insurance has gotten rich since the passage of the ACA. Between 2014 (the year the entirety of the ACA was implemented) and 2024, just seven for-profit health insurers amassed $543.4 billion in profits and took in a staggering $10.192 trillion in revenues.
“And they have made, I mean, you look, $1,400 to $1,700 increase, 100 percent increase over the last number of years. There’s really few things that have gone up like insurance companies.”
The president is kind of right. As KFF reports, the cost of a family policy has increased 60% since 2014 – a rate of increase much higher than general inflation and also higher than medical inflation. And as we’ve published previously, not only has the total cost of an employer-sponsored plan skyrocketed, so has the share of premiums workers must pay. This year, employers deducted an average of $6,850 from their workers’ paychecks for family coverage, up from $4,823 in 2014. And keep in mind, all that money our employers are having to send to insurance companies is not money that’s available to give raises to workers or hire more people.
“They’re getting numbers and money like nobody’s ever seen before. Billions and billions of dollars is paid directly to insurance companies. We’re not going to do that anymore.”
The president is right. Several Big Insurance companies have ballooned in size over the past decade to become some of the world’s biggest corporate conglomerates. UnitedHealth Group, CVS/Aetna and Cigna are now numbers 3, 5 and 13 on the Fortune 500 list. The only American companies that take in more revenue than UnitedHealth are Walmart and Amazon.
“I believe Obamacare was set up to take care of insurance companies, not to take care of the American public.”
The president has his history wrong here. While there are plenty of Monday-morning-quarterbacking you can do for the ACA – the law was not passed to “take care of insurance companies.” While the ACA didn’t fix everything – not by a long shot – it did stop some of the insurance industry’s worst abuses, like refusing to sell policies to people with preexisting conditions – even acne – and “rescinding” policies to avoid paying for life-saving care. Some insurers were found to be paying employees bonuses to find policies to rescind, including the policies of women almost immediately after being diagnosed with breast cancer.
It prohibited health insurers from charging people more because of a preexisting condition and from dumping the sick so they could reward their shareholders more generously. Keep in mind that insurers consider every claim they pay as a loss, hence the term “medical loss ratio” (MLR), which the ACA addressed by requiring insurers to spend at least 80%-85% of our premiums on our health care.
And it’s not like Big Insurance wanted the ACA to pass. Back in 2010, America’s Health Insurance Plans (AHIP), the PR and lobbying group for health insurers, quietly funneled $100 million to the U.S. Chamber of Commerce to orchestrate a PR, advertising and lobbying blitz to keep the ACA from being passed.
While big health insurance companies have only grown since the passage of the ACA, it has been Big Insurance’s corporate maneuvers and work on Capitol Hill (not the law itself) that has allowed these companies to flout some of the ACA’s regulations and bend the law to do their will.
“I love the idea of money going directly to the people, not to the insurance companies. Going directly to the people. It could be in the health savings account. It could be a number of different ways.”
While that is a compelling sound bite, it’s disingenuous. The money proposed by Cassidy and Crapo to go to HSAs would then be used by enrollees to buy insurance, thus still giving money to the insurance companies. Even worse, the proposed amount of money to go to people’s HSAs to help them pay for health insurance and care is $1,000-$1,500. This is money that would be used to purchase a bronze or copper plan with a high deductible (with many of those plans having deductibles north of $5,000). That means under this plan people would still need to come up with thousands to meet their deductible on top of paying their premiums every month. $1,000 wouldn’t come close to even covering the premiums for a decent policy, much less the out-of-pocket costs.
Replacing ACA subsidies with HSAs would still keep Americans tied to the same private health insurers that Trump calls “big, bad” and “money-sucking.”Most families would still be exposed to crippling medical bills, and even more tax dollars would flow to insurance conglomerates that own HSA custodian businesses (like UnitedHealth’s Optum Bank).
“And the people go out and buy their own insurance, which can be really much better health insurance, health care.”
That’s wishful thinking far removed from reality. The health insurance plans available to people who get money for their HSAs under the Cassidy-Crapo proposal – rather than getting subsidies – are the same as those currently available. Worse, without the subsidies, people will not be able to afford the gold or silver plans that have lower out-of-pocket costs. In reality the plans that people buy under the proposed Cassidy-Crapo plan would have less value than the plans they previously bought with subsidies.
Trump’s comments are coming ahead of tomorrow’s scheduled vote in the Senate on dueling Democratic and Republican proposals to deal with the enhanced subsidies for ACA plans that will expire in three weeks. Without those subsidies, premiums will spike for many of the 24 million American enrolled in “Obamacare” plans. Democrats want to extend the subsidies for three years. Republicans, led by Senate Majority Leader John Thune, will push a plan replacing those subsidies with direct payments into individuals’ Health Savings Accounts (HSAs), as the president is suggesting. Neither plan is expected to get the 60 votes required for passage. What happens next is anybody’s guess.
Hospitals are closing unprofitable pediatric units and eliminating some surgical services for kids as they grapple with lower Medicaid reimbursements, staffing issues and more complicated cases, a 20-year review in the journal Pediatrics found.
Why it matters:
The cuts can erect additional hurdles to getting care in already underserved communities and require families to travel longer distances to regional or urban health centers.
What they found:
The review of nearly 4,000 facilities from 2003 to 2022 found the proportion of hospitals that researchers identified as having the lowest capabilities for pediatric care more than doubled.
The most common services shed were appendectomies (50.5% fewer hospitals), hospitalizations for pneumonia (42.3%) and asthma hospitalizations (41.1%).
In contrast, capabilities like organ transplantation and open-heart surgery for congenital defects showed little to no change.
The intrigue:
Hospitalizations for children fell 26% from 2000 to 2019, prompting more hospital operators to take pediatric inpatient units offline, with little incentive to bring them back.
The resulting regionalization of pediatric care “has not shown signs of slowing, and it remains to be seen whether there is a floor on pediatric capacity,” they wrote.
Yes, but: The lack of pediatric inpatient beds doesn’t mean that a hospital will not admit a child on an adult ward.