Jamie Dimon, chief executive officer of JPMorgan Chase & Co.
According to Jamie Dimon, chairman and CEO of JPMorgan Chase, the most successful leaders have certain key traits.
″[H]umility, openness, fairness [and] being authentic” are most important – “not [being] the smartest person in the room or the hardest working person in the room,” Dimon, who runs the nation’s largest bank and oversees more than 250,000 employees globally, told LinkedIn editor in chief Daniel Roth in a recent video.
“Management is: Get it done, follow-up, discipline, planning, analysis, facts, facts, facts. It’s [getting] the right people in the room, kill the bureaucracy, all of these various things,” Dimon told Roth. “But the real keys to leadership aren’t just doing that.”
It’s about having “respect for people,” not about having “charisma” or “brain power,” he said.
Having these traits also increases your productivity, along with your success, Dimon said. If you’re “selfish” or “take the credit” when it isn’t warranted, others are “not going to want to work,” which will impact efficiency on the job.
Dimon also looks for these things when hiring, he said in July. When interviewing or assessing a promotion, Dimon asks himself a few questions about the candidate, including, “Would you work for that person? Would you want your kid to work for that person?”
He also considers whether they “take the blame” or “how they act anytime something goes wrong.”
In his role as CEO, Dimon said he tries to practice what he preaches.
“No one would say Jamie Dimon is humble,” he said in July, “but I treat everyone the same, and I expect the same thing. You’d want to work for me if you think I give a s—, if I treat you fairly, if I treat everyone equally.”
To achieve success, “treat people the way you want to be treated,” Dimon told Roth. “Have respect for people.”
In nearly every facet of our lives, all of us are routinely put in the position of trying to settle disputes or disagreements, whether it be with our spouses or significant others, our children, our siblings, co-workers, neighbors, contractors — you name it. It’s part of everyday life. Conflicts arise and we figure out how to resolve them.
Unfortunately, in the politically toxic environment in which we now live, compromise is now perceived as a sign of weakness. Elected leaders are routinely criticized and attacked by fellow party members and their constituents for trying to find middle ground on any issue, particularly those rooted in ideology. The bipartisan agreement reached in Congress last week on gun safety was a rare and welcome exception.
While they hold starkly different positions and come from states that are thousands of miles apart geographically and politically, Senators Chris Murphy, D-Conn., an outspoken proponent of stronger gun safety laws, and John Cornyn, R-Texas, a staunch Second Amendment advocate, found a way to set aside their differences and reach compromise on the so-called Bipartisan Safer Communities Act that was approved by the Senate 65-33 and the House by a margin of 234-193. President Joe Biden signed the legislation into law June 25.
While the new law does not go nearly as far as Senator Murphy and most of his fellow Democrats wanted by, for instance, banning the sale of assault rifles or at least increasing the age to buy them, the willingness to finally get something done after 30 years of Congressional gridlock was a long-overdue victory for common sense.
Bipartisanship has also been evident in Congressional support for military funding for Ukraine and the 2021 Infrastructure Investment and Jobs Act, but little else.
Despite the glimmer of progress in our nation’s legislative branch of government, it appears that polarization now has a firm grip on our nation’s top court. In trying to find middle ground in deliberations on Roe v. Wade, U.S. Supreme Court Chief Justice John Roberts sought this compromise with his five fellow conservatives and three liberals on the bench: support Mississippi’s prohibition against abortion after 15 weeks, but preserve some semblance of reproductive rights for women by not overturning Roe v. Wade or the court’s 1992 ruling in Planned Parenthood v. Casey.
“The Court’s decision to overrule Roe and Casey is a serious jolt to the legal system — regardless of how you view those cases,” Roberts wrote. His incremental approach found no takers among his entrenched colleagues on either the right or the left. Hence, constitutional protections for abortions that had stood for nearly 50 years — and are supported by the vast majority of Americans — were stripped away in a 5-4 vote, leaving the power to individual states.
Unfortunately, bipartisanship can be equally elusive in state capitals around the country, which does not bode well for reproductive rights advocates in 21 states where abortion is now illegal or have “trigger bans” that will take effect within 30 days of the Supreme Court’s June 24 ruling.
Regardless of whether the issue is abortion or other divisive topics such as immigration, gun safety, voting rights, bail reform or LGBTQ rights, governors and state legislators of one controlling party or another routinely dig in and take intractable positions, leaving little or no room for negotiation.
We would all be well served to reintroduce ourselves to the art of compromise, for the good of our family relationships, for the good of our respective professions, for the good of our country and society in general, and even for the good of our own personal health as we consider whether to consume that extra helping of food or another cocktail.
Moderation is key in our lifestyle choices and it could also go a long way in trying to find middle ground with those who have differing opinions. If adversaries are truly motivated to do the right thing, not political gamesmanship, they should always choose their words carefully, listen with an open mind and always be open to making concessions. In short, we should all start by embracing civility.
Job seeking is a grueling process, but it is also an opportunity to put your best foot forward in order to find a company that is the best fit for you.
Although it can be nerve wracking to sit through one interview after another, candidates should remind themselves that these interactions are a two-way street, and they have every right to ask challenging questions to make a decision, should the offer come.
Here are the critical questions you as a candidate must ask during a job interview—because remember, you’re interviewing the employer, too.
QUESTIONS TO ASK YOURSELF BEFORE APPLYING FOR THE JOB
Before setting off on your job search, make a list of the types of companies you’re interested in.
Is this a place you see yourself thriving in?
Do you believe in the mission?
Why do you want to work at this place?
What attracts you about the organization?
Oftentimes, our current situations dictate how we go about making our next move. Perhaps you’re working in an environment that you find suffocating and want out, or you’re seeking more responsibilities, or are looking to become a people manager.
Whatever the case, be sure to keep in mind that in every new workplace, there will be pros and cons, no matter the salary or job description. So be cognizant of all the aspects of a new role that are truly important to you; also, be mindful of what your personal dealbreakers are.
PREPARE A LIST OF STRATEGICALLY PLANNED QUESTIONS
Interviewing is a two-way exchange. While candidates are being scrutinized by the potential employer, the skilled candidate will have an opportunity to evaluate the company based on the flow of the conversation.
Typically, candidates aren’t given the opportunity to ask questions until the very end of the interview. That’s not to say there aren’t ways to integrate specific queries into the conversation, as long as you remember that you’ll get full control of the floor in the grand finale.
In a previous Fast Company story, Patrick Mullane, executive director of Harvard Business School Online, shares how interviewees often will drop the ball when the interviewer tosses out the famous line, “Do you have any questions for me?”
“Candidates forget that when they’re given control of the discussion, it’s an opportunity to do two very important things. First, it’s a chance to learn something genuinely useful about the firm you might be joining. Second, you get to show that you’re thoughtful and conscientious,” he said. “Both are hugely important as you look to make a change. Don’t waste the opportunity.”
When it comes to the questions candidates typically ask companies during an interview, the “big three” revolve around corporate culture, the interviewer’s personal experience (“How have you liked working here?”), and growth.
Rather than default on these inquiries (which interviewers likely receive quite often and may respond in kind with generic answers), Mullane challenged candidates to take these questions and reframe them in a more thoughtful, strategic way:
Culture questions: Rather than asking, “What’s the culture like here,” ask something along the lines of, “Can you share a time when the company’s culture made you excited to work here or helped you during a challenging time?” This bypasses a typical answer like “It’s collaborative,” and dives into the intersection of employees and culture, offering an in-depth look into a specific, and perhaps relatable, scenario.
Personal experience questions: Instead of “How do you like working here?” try, “I noticed you left X company for this one. What convinced you to make the jump?” This reframing achieves two things: It shows the interviewer you did your research and gives you insight into their decision-making, which may help you make your own.
Company growth questions: A question like, “I noticed the company is growing rapidly. Do you expect that to continue?” will often bear a generic, dead-end answer. To get additional, more useful information, put a spin on it. Ask something like, “I noticed the company is expanding rapidly. Is this putting a strain on your customer service team?” Getting information on a company’s financials is not particularly difficult, especially if it is already publicly traded. But asking a question of this nature is especially useful if you are interviewing for a role like Customer Success Manager, as it allows you to get a better sense of how growth impacts the day-to-day of the team.
Overall, it will only work in your favor when you do your due diligence in gathering intelligence on the company you are interviewing for; also, you’ll be setting yourself up for success by having prepared questions that lead to a conversation and present yourself as a thoughtful and conscientious candidate.
“In a hot job market, it’s tempting to be lazy when doing the upfront work to prepare for an interview,” said Mullane. “It’s easy to figure that the interview is over when the person interviewing you gives you the floor. But it’s not. Asking better questions in the right way can significantly increase the chances you’ll not only impress the interviewer, but also gain valuable insights that can help you decide if the position is right for you.”
COVER THE BASICS
It can be easy to get caught up in nerves when interviewing for a company you are extremely attracted to—or even in general. Interviewing is a lot of pressure!
However, when preparing to ask your questions, the areas that you as a candidate must focus on should give you a well-rounded perspective on multiple aspects of the company, not just the specific job description.
This Fast Company article shared a roundup of all the pertinent focus areas that your questions should fall under to get you the best answers, which include:
The specific role you are interviewing for
The management style of your would-be boss or team
Company culture and reputation
What performance metrics look like
What kind of colleagues you can expect to work with
Opportunities for growth
ASK TOUGH BUT FAIR HIGH-LEVEL QUESTIONS
Sometimes it’s not enough to consider the high-level questions, such as salary and work culture. Many of us are in a unique position in life, whether that involves our personal situations, families, health, or other concerns.
When considering your interest in a company, it’s helpful to understand how they can help or support you as an individual beyond your contributions to the job.
On the flip side, you’ll want to know other aspects of internal support for employees. How does this company support internal mobility? How do managers deliver feedback? In other words, what will a day in the life of this role really be like?
Prepare to ask the employer a series of questions tailored to your situation. FlexJobs’ team of career coaches offers guidance in this Fast Company story, including specific inquiries to ask your interviewer, such as:
Why is this position available? This can give you some insight into the way things are handled at the company. Was someone fired? Are they unable to keep the position filled because of the workload?
What makes it a great day at work, and what makes it a challenging day? Answers to this question can vary depending on the personal experience of the interviewer, but it’s good to get a sense of how they approach the question.
How are criticism and feedback handled within the team? Mistakes can happen, and knowing that managers on the team can handle employee errors with grace will offer a sense of relief rather than unnecessary conflict when they do occur.
Do you have any Employee Resource Groups (ERGs)? How do they support the company’s DEI plans? This question gives you an opportunity to understand where the company stands in terms of diversity, equity, and inclusion (DEI) and how well they support the objectives of ERGs, as well as pushing forward their higher-level strategy.
How does the company approach salary differences? This can highlight whether the company pays people differently based on location, if they work remotely, in-office, or hybrid. It can also shed light on whether the company has done a pay audit to achieve equity, especially for women and underrepresented groups.
What’s the company’s approach to supporting work-life balance? Many companies have put forth specific benefits and incentives to support employees in the past two years, including mental health initiatives, fitness classes, therapy, and flexibility. This critical question will help you determine just how the company views employees as individuals and not just by their work output.
An example of a tough conversation to navigate can pertain to how the organization supports employees in specific work situations. If this particular job requires you to relocate, an example of how to navigate the question of moving-cost accommodations might go something like this:
Candidate (C): I noticed this position is based in San Francisco. Is there an option for potential hires to work remotely?
Interviewer (I): I’m afraid our new company policy is to operate on a hybrid schedule. This particular role is based in the Bay Area and requires the individual to come into work three times a week.
C: I understand. Sometimes companies need to make tough decisions based on their needs.
I: Do you think you would be willing to relocate, should we decide to move forward with your application?
C: I think this role is a wonderful opportunity for me, and I truly believe my personal values align with those of this company and its culture. If all goes well, I’d like to learn what the company’s budget is in regards to supporting moving and transition costs.
In this scenario, the interviewer is honest about the new hybrid model their company has adopted. If you, the candidate, are first learning about this aspect during the interview, it’s important to ask direct questions about how the company plans to support potential moving costs, rather than framing the question in a way that offers a loophole or an out.
Organizations are aware that with the plentiful options of remote jobs, finding talent willing to relocate or adopt a hybrid work life will be tougher. Know that the ball is in your court and be straightforward about expensed costs if you are willing to relocate.
WRAP UP THE INTERVIEW WITH THESE KEY QUESTIONS
This will likely be the last time you interact with this team member before either moving onto the next stage or the decision-making process.
In a prior Fast Company story, the founder of executive search firm The Mullings Group shares the best questions to ask when wrapping up.
Don’t let the conversation end without answers to the following questions, so you have enough information to help you reflect on and assess your experience and understanding of the company.
Am I a good fit for this company? The feeling needs to be mutual. Be sure to determine whether your skills, interests, personality, and goals align with the direction of the company.
What are the expected deliverables for this role over the next three months to a year? Depending on the role of the person you are interviewing with, you may get different answers. This is a good question to ask to get a sense of the priorities as it relates to different stakeholders.
How will we both know that I have succeeded in this role? This is another question in which the answers may vary, but it will be helpful for you as a candidate to understand how to work toward specific goals and measure your own impact so that, when it comes time for a raise or promotion in the future, you have the evidence to back it up.
What are the growth opportunities in this role, and what important skills will I learn? It’s not enough to make a lateral move. You need to know how will working for this company enable you to grow and thrive.
Who will I become? Your environment and the people you work with will directly influence your work output, ethic, and your future values. Asking questions about the kind of people you will interact with regularly will help you get a sense of what your day-to-day experiences will look like.
Getting a new job is a big deal. You will be working 40 hours a week in a specific environment that supports a certain culture and hires a certain type of colleague. It’s not just the job description that matters, nor the skill set the company requires to perform in that role. A new job is a combination of your livelihood, a commitment to learn and grow, and contribute.
Remember to be selective in your process because you’re interviewing your next employer, too.
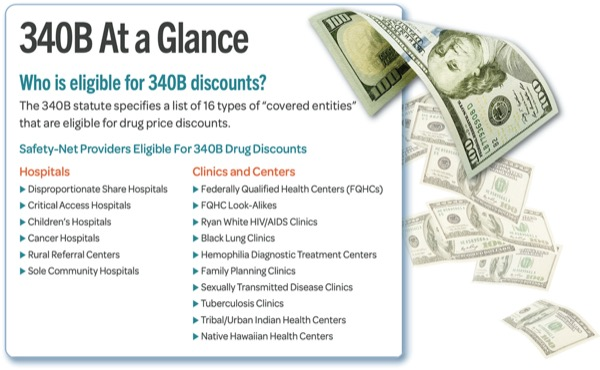
The American Hospital Association wants HHS to act quickly to ensure that affected hospitals receive withheld 340B program funds.
The organization’s June 28 letter to HHS comes after the Supreme Court recently overturned a $1.6 billion 340B payment cut.
The case centered around whether CMS has the authority to make cuts to the program under its Medicare Outpatient Prospective Payment System. Under the payment rule, HHS cut the reimbursement rate for covered drugs by 28.5 percent in 2018, but it later lowered the cut to 22.5 percent. The Supreme Court reversed a federal appeals court’s 2020 ruling that HHS had the authority to make the $1.6 billion annual reimbursement cut.
“Given the vital role that 340B hospitals play in serving vulnerable communities, they should be repaid the funds that have been withheld from them without delay,” the American Hospital Association said in the letter. “They also should be paid for all of the years (2018-2022) in which the Centers for Medicare & Medicaid Services (CMS) illegally cut reimbursement rates.”
The hospital group said it is concerned that despite the Supreme Court’s decision, the resolution of these issues “could be bogged down in needless litigation, and that hospitals will not be appropriately compensated at a time when they are weathering significant financial challenges on many fronts.”
Summary U.S. hospitals and health systems continued to face difficult financial and operational headwinds in May. Operating margins rose from April but remained significantly lower than pre-pandemic levels and May 2021.
Volumes were up slightly from the previous month, with rising ED visits close to numbers last seen in 2019 and earlier. Gross operating revenues rose month-over-month and in comparison to May 2021. But expenses — especially labor costs — were elevated across nearly every metric month-over-month.
Margins The median Kaufman Hall Year-To-Date (YTD) Operating Margin Index reflecting actual margins was -0.33% through May. The median change in Operating Margin was up 18.9% from last month but down 45.6% from May 2021. The median change in Operating EBITDA Margin was up 13.5% month-over-month, but down 36.1% from May 2021.
Volumes Patient volumes rose in May, with Length of Stay (LOS) up 2.3% from April and 5.5% compared to May 2021. Patient Days increased by 4.8% month-over-month but dropped 0.5% versus May 2021. Adjusted Patient Days grew 3.5% from April to May and were 4% above May 2021 levels. Adjusted Discharges rose slightly, at 0.6% month-over-month, but were down 0.3% compared to May 2021. Surgeries barely fluctuated, with Operating Room Minutes down 1.0% from last month and up just 0.1% YOY. Emergency Department (ED) Visits jumped 9.5% from April to May and were up 4.5% YOY.
Revenues Volume increases resulted in slightly improved revenue performance in May. Gross Operating Revenue was up 3.4% from April and 7.6% YOY, and is up 6.9% YTD. Similarly, Outpatient (OP) Revenue rose 2.2% from April levels, 9.4% YOY and is up 9.1% YTD. Inpatient (IP) Revenue climbed 3.5% from the previous month and 2.6% from May 2021, and is up 4.2% YTD.
Expenses Total Expenses continued to climb in May, rising 1.1% from April and 10.7% from May 2021. Inflation and labor shortages contributed to total costs climbing 10.4% YTD.
Labor Expense per Adjusted Discharge inched up by 1.0% from April and has surged 13.6% YTD, while Full-Time Employees Per Adjusted Occupied Bed (FTEs per AOB), is down by 2.7% YTD, indicating that hospitals are spending more on labor costs with fewer hours worked. However, FTEs per AOB rose slightly in May, up 2.8% from April. Total Expense per Adjusted Discharge increased by 0.3% from April, and Labor Expense per Adjusted Discharge rose 1.0% from last month.
Non-Operating The Federal Reserve raised its benchmark rate by 75 basis points in mid-June, the most aggressive increase since 1994, as inflation hit a 40-year high of 8.6% in May. New projections show The Federal Open Market Committee (FOMC) participants expect the Fed to raise rates to at least 3% this year, with half indicating 3.375%. Labor metrics remain strong with unemployment reading 3.6% in May and employers adding 390,000 new jobs.
Consumer sentiment hit a record low reading of 50.2 in early June, comparable to the low point reached during the 1980 recession. US equities ended May with marginal gains after weeks of volatile trading due to economic data and corporate earnings sowing doubt over the health of the US economy.
Takeaways at a Glance
Nearly halfway through 2022, margins are cumulatively negative. While some metrics have normalized, hospitals continue to perform below pre-pandemic levels, and there is an uncertain outlook for the rest of the year.
Elevated labor costs remain a significant challenge. Hospitals are still seeing higher labor costs and fewer hours worked, a sign of inflation and an indicator that long-standing labor shortages are likely worsened by increased turnover.
Warmer temperatures and ED visits drove up volumes and revenues. Patients often schedule elective procedures during the summer months, which may have contributed to growing volumes. Emergency department visits also spiked this past month as people spent more time outdoors.
Pent-up demand for hospital services also contributed to an increase in patients. Sicker patients continued to schedule procedures they had previously postponed, suggesting a return to normalcy as COVID-19 hospitalizations remained relatively low.
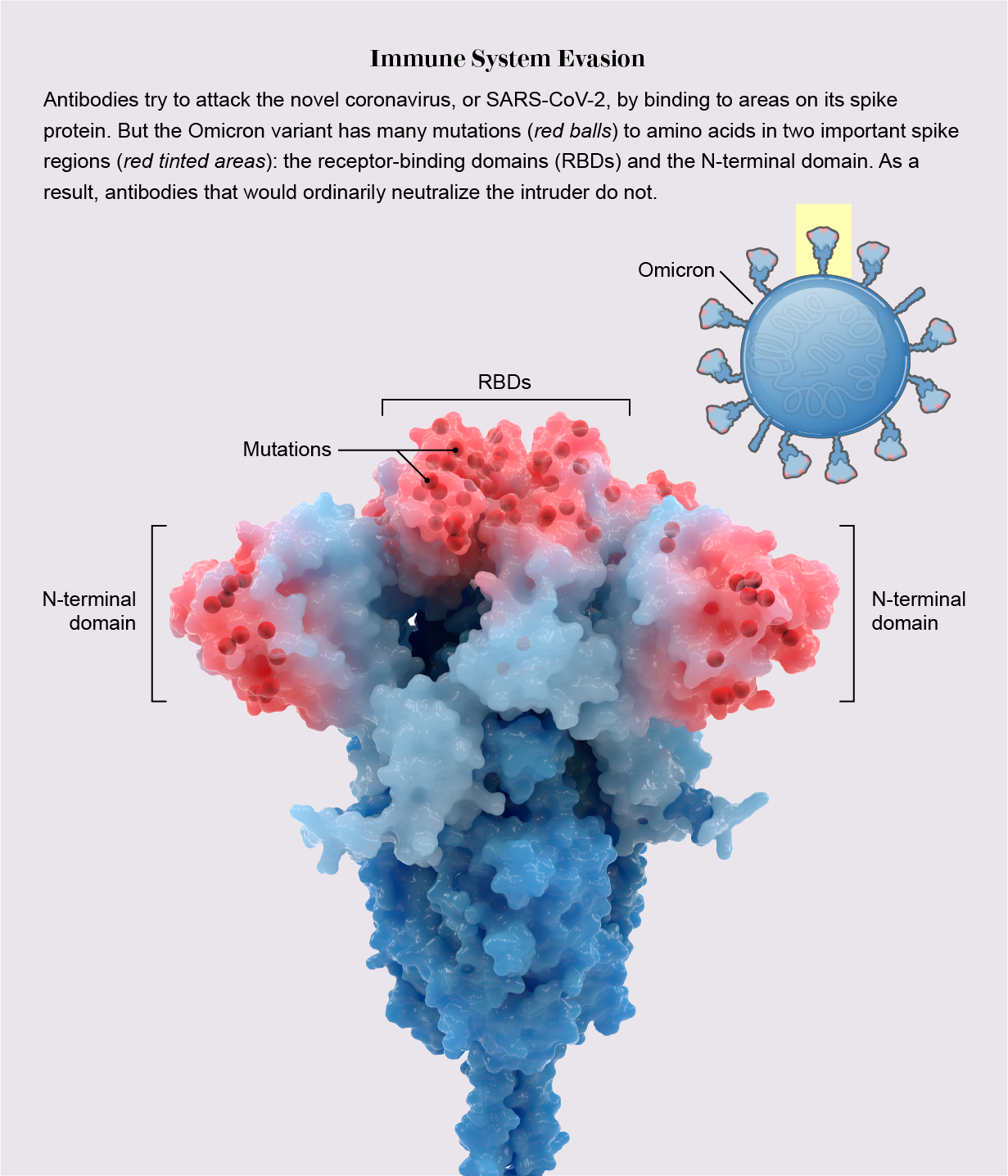
The COVID-19 vaccine strategy for the fall remains beset with unanswered questions after an FDA expert panel on Tuesday spent hours debating how and whether to update the shots.
Why it matters: Time is running short to develop a game plan with existing vaccines losing effectiveness against new variants and more than half of Americans still without a booster dose.
Driving the news: The Vaccines and Related Biological Products Advisory Committee voted 19-2 to recommend an Omicron-specific update to COVID-19 booster vaccines expected to be rolled out within the next few months.
But key questions were left unanswered:
The panel didn’t formally decide whether to update shots with the prevalent Omicron strain in circulation, currently the fast-spreading BA.4 and BA.5 subvariants, or the BA.1 lineage that emerged late last year, as the World Health Organization recommended.
The consensus appeared to be for a bivalent, or combination, booster combining the original COVID-19 strain that emerged in late 2019 with BA.4 and BA.5.
The FDA will continue to evaluate what to do about the primary series of vaccines for the fall.
Experts were split on whether there was enough data to recommend the updated shots for kids, or whether more studies are needed on dosage and possible side effects.
There also were concerns about what effect an updated vaccine would have on developing nations’ willingness to use older COVID shots to inoculate their populations.
And above all, it’s unclear whether all the questions about who gets which shot when will add to public confusion and apathy that’s dogged the vaccination effort in recent months.
What they’re saying: “None of us has a crystal ball and we’re trying to use every last ounce of what we can from predictive modeling and data that’s emerging to try to get ahead of a virus that’s very crafty,” said top FDA vaccine regulator Peter Marks.
“Unfortunately, looking in the past doesn’t help us a great deal to look in the future for [a] virus that has baffled a lot of us and made predictions almost irrelevant,” said acting panel chairman Arnold Monto, a University of Michigan epidemiologist.
The timetable: Pfizer-BioNTech said an updated mRNA vaccine could be ready in October if regulatory uncertainties are ironed out. Moderna said it could have large amounts ready in late October or early November. Novavax is still awaiting emergency use authorization for its protein-based shot, but said it could have an updated vaccine by the fourth quarter.
Leukemia Lymphoma Society (LLS) supports actions that regulate or prohibit “junk insurance” plans that discriminate against people with pre-existing conditions, offer no meaningful coverage in the case of a cancer diagnosis or neglect to cover essential healthcare services like prescription drugs
The problem
LLS advocate Sam Bloechl thought he was doing everything right. After experiencing back pain that wouldn’t go away, he spoke to an insurance broker about upgrading his insurance plan to better cover any treatment he might need. Sam’s broker insisted she had the perfect plan for him. It wasn’t.
A month later, Sam was diagnosed with non-Hodgkin lymphoma. After chemotherapy and radiation, Sam achieved remission. But his health plan refused to cover the bill, leaving Sam with more than $800,000 in medical debt. It turns out he was sold a short-term, limited-duration plan—a type of “junk insurance.”
Sam isn’t alone. Patients with pre-existing conditions are penalized by low-quality policies, known as “junk insurance” Because such plans are exempt from important consumer protections, they can leave patients vulnerable when they most need timely access to quality, affordable care.
The patient impact
Most short-term, limited-duration plans leave patients on the hook for thousands of dollars if they face serious health problems—much more than they’d face if they had traditional health insurance, a recent Milliman study funded by LLS reveals. The plans often rely on misleading marketing and are misunderstood by consumers who buy them. And patients have no right to appeal plan decisions.
Moreover, junk plans drive up more than a patient’s out-of-pocket costs—they threaten prices across the health insurance market. As younger and healthier individuals choose these cheaper “junk plans” over comprehensive insurance, premiums for comprehensive insurance are expected to rise.
Solutions
LLS supports actions that regulate or prohibit “junk insurance” plans that discriminate against people with pre-existing conditions, offer no meaningful coverage in the case of a cancer diagnosis or neglect to cover essential healthcare services like prescription drugs. These plans include:
• Short-term, limited-duration insurance • Health care sharing ministries • Farm Bureau plans • Grandfathered plans • Multiple employer welfare arrangements and association health plans • Spurious single-employer self-insured group health plans • Minimum essential coverage-only plans • Excepted benefit plans
A report published by 30 patient organizations, including LLS, explains these types of plans in depth—and details how state and federal lawmakers can help protect patients and consumers from these dangerous plans.
LLS works to stop policy proposals that would allow insurers to reinstitute lifetime limits, eliminate the current cap on patient cost-sharing and cover fewer essential services for cancer patients.
Political will seems to be growing to reshape the increasingly popular Medicare Advantage program.
At a House Energy and Commerce committee hearing on Tuesday, lawmakers on both sides of the aisle called for more oversight of MA following watchdog reports that found impediments to receiving covered care, including improper denials of prior authorization requests, and plans gaming the system in exchange for more funding from Medicare.
“Medicare Advantage is an important tool for helping seniors and we want it to succeed. We’re going to continue to conduct the oversight necessary,” said Oversight and Investigations Subcommittee Chair Diana DeGette, D-Colo.
Witnesses at the hearing — officials from the Government Accountability Office, HHS Office of Inspector General and congressional advisory board MedPAC — also pointed to higher rates of beneficiary disenrollment in their last year of life and opaque plan data, which can complicate oversight efforts.
Surveys have shown MA remains extremely popular with beneficiaries, attracted by lower co-pays and supplemental benefits like vision coverage and telehealth. In the program, Medicare pays private plans a capitated monthly rate to provide care for their beneficiaries based on the severity of their beneficiaries’ needs.
The hearing comes amid inflamed industry debate over the future of MA.
For-profit hospital lobby Federation of American Hospitals submitted a letter for the record sharing concerns over some MA plans denying patient care and having inadequate care networks.
Meanwhile, MA trade group Better Medicare Alliance sent a letter to the CMS on Monday urging the agency to safeguard the program as Congress mulls changes to Medicare.
But as Medicare’s hospital benefit — part of which funds MA — limps towards insolvency, lawmakers appear poised to target the growing MA program in a bid to crack down on improper payments and care denials.
“This is something that I think is very much bipartisan,” said Rep. Gary Palmer, R-Ala.
Coverage delays and denials
It’s not the first time lawmakers have zeroed in on MA oversight as a strategy to save Medicare money: In a Senate hearing on Medicare insolvency in February, Sen. Elizabeth Warren, D-Mass., said “the Medicare system is hemorrhaging money on scams and frauds” due to insurers taking advantage of the program’s rules to increase profits.
Even amid rising congressional criticism of MA, lawmakers on Tuesday reiterated their support for the program overall, which covered roughly 27 million Americans in 2021.
That’s more than a third of all Medicare beneficiaries, though MA is expected to swell to cover half of all Medicare members by 2030.
But lawmakers said they are increasingly concerned about disparities in the quality of coverage offered by Medicare Advantage plans compared to traditional Medicare plans, along with unscrupulous practices in the program resulting in higher reimbursement for MA organizations.
A GAO report found MA beneficiaries in their last year of life disenroll from MA in favor of traditional Medicare at a rate two times higher than other MA members, suggesting the plans may not support high-cost and specialized care, testified Leslie Gordon, GAO’s acting director for healthcare.
Gordon called it a “red flag” for the program that requires more scrutiny from CMS.
In addition, an HHS OIG report published April found MA organizationswrongly denied members care, with plans turning down 18% of payment requests that should have been approved.
Erin Bliss, OIG assistant inspector general in the Office of Evaluation and Inspection, testified plans sometimes use internal critical criteria that are not required by Medicare. In one example, an MA plan denied a medically necessary CT scan to diagnose a serious disease, citing that the patient hadn’t yet received an x-ray, Bliss said.
When appealed, plan denials were reversed 75% of time, a rate DeGette called “alarmingly high.”
“We are concerned that patients are receiving the timely care they need in those situations,” Bliss said.
OIG also found plans denied 13% of prior authorization requests that would have been approved under traditional Medicare.
Rep. Michael Burgess, R-Texas, suggested policymakers consider requiring insurers to forego prior authorization for doctors with a consistent track record of submitting accurate data. That strategy, called “gold carding,” is already used in some states, including Texas and West Virginia, to pare back on prior authorization delays.
MA payment reform
Along with coverage restrictions, lawmakers at Tuesday’s hearing asked witnesses about the scope and severity of improper MA payments in a bid to zero in on specific solutions Congress and the CMS can enact.
Though MA has potential to save the Medicare program money, “the current incentives for MA plans are not adequately aligned with the Medicare program,” said James Mathews, MedPAC executive director.
“Substantial reforms are urgently needed,” especially in light of Medicare’s “profound” financial problems, Mathews said.
In 2022, the average MA plan bid was 85% of fee-for-service spending, Mathews said. However, Medicare pays plans 104% of fee-for-service costs.
That imbalance is partially due to plans making patients appear sicker than they are to get extra payments from the government, witnesses said. The practice, called “coding intensity,”resulted in an estimated $12 billion in excess Medicare spending in 2020, according to MedPAC data.
Methods include chart reviews, where plans identify and add patient diagnoses that aren’t included in the service record, and health risk assessments, where plans contract with vendors to visit beneficiaries homes and conduct assessments, finding new diagnoses that often aren’t backed up by other records, according to Bliss.
GAO estimates that roughly a tenth of Medicare payments to MA plans in 2021 were improper, Gordon said.
To try to tamp down on coding intensity, the CMS should conduct targeted oversight of MA plans that routinely use these tools, and reassess whether chart reviews and in-home assessments are allowed to be sole sources of diagnoses for payment purposes, witnesses said. In addition, MA should improve care coordination for enrollees who receive health risk assessments.
The CMS should also consider replacing the quality bonus program and change its approach to calculating MA benchmarks, Mathews said.
In addition, the agency should require and validate data for completeness and accuracy before risk-adjusting payments through methods like medical record reviews, Gordon said.
Gordon also suggested the agency conduct more timely audits, as the CMS is currently missing out on recouping hundreds of millions of dollars in improper payments.
Policymakers appeared open witnesses’ suggestions to ensure MA is running as smoothly as possible, with Rep. Frank Pallone, D-N.J., calling for an additional hearing on the matter.
“This is bipartisan … You can be assured that we’re going to be following up,” DeGette said.
Here are 19 health systems with strong operational metrics and solid financial positions, according to reports from Fitch Ratings, Moody’s Investors Service and S&P Global Ratings.
1. Morristown, N.J.-based Atlantic Health System has an “Aa3” rating and stable outlook with Moody’s. The health system has strong operating performance and liquidity metrics, Moody’s said. The credit rating agency expects Atlantic Health System to sustain strong performance to support capital spending.
2. Banner Health has an “AA-” rating and stable outlook with Fitch. The Phoenix-based health system’s core hospital delivery system and growth of its insurance division combine to make it a successful highly integrated delivery system, Fitch said. The credit rating agency said it expects Banner to maintain operating EBITDA margins of about 8 percent on an annual basis, reflecting the growing revenues from the system’s insurance division and large employed physician base.
3. Clearwater, Fla.-based BayCare has an “AA” rating and stable outlook with Fitch. The 14-hospital system has excellent liquidity and operating metrics, which are supported by its leading market position in a four-county area, Fitch said. The credit rating agency expects strong revenue growth and cost management to sustain BayCare’s operating performance.
4. CentraCare has an “AA-” rating and stable outlook with Fitch. The St. Cloud, Minn.-based system has a leading market position and solid operating margins, Fitch said. The credit rating agency said it expects CentraCare’s operating platform to remain strong.
5. Greensboro, N.C.-based Cone Health has an “AA” rating and stable outlook with Fitch. The health system has a leading market share and a favorable payer mix, Fitch said. The health system’s broad operating platform and strategic capital investments should enable it to return to stronger operating results, the credit rating agency said.
6. Franciscan Alliance has an “AA” rating and stable outlook with Fitch. The Mishawaka, Ind.-based health system has a very strong cash position and maintains leading market shares in seven of its nine defined primary service areas, Fitch said. The health system benefits from a good payer mix, the credit rating agency said.
7. Gundersen Health System has an “AA-” rating and stable outlook with Fitch. The La Crosse, Wis.-based health system has strong balance sheet metrics and a leading market position and expanding operating platform in its service area, Fitch said The credit rating agency expects the health system to return to strong operating performance as it emerges from disruption related to the COVID-19 pandemic.
8. Falls Church, Va.-based Inova Health System has an “Aa2” rating and stable outlook with Moody’s. The health system has a consistently strong operating cash flow margin and ample balance sheet resources, Moody’s said. Inova’s financial excellence will remain undergirded by its favorable regulatory and economic environment, the credit rating agency said.
9. Vineland, N.J.-based Inspira Health Network has an “AA-” rating and stable outlook with Fitch. The health system has strong operating performance, a leading market position in a stable service area and a growing residency program, Fitch said. The credit rating agency expects the system’s growing outpatient footprint and an increase in patient volumes to support its operating stability.
10. Oakland, Calif.-based Kaiser Permanente has an “AA-” rating and stable outlook with Fitch. The health system has a strong financial profile, and the system’s operating platform is “arguably the most emulated model” for nonprofit healthcare delivery in the U.S., Fitch said. By revenue base, Kaiser is the largest nonprofit health system in the U.S., and it is the most fully integrated healthcare delivery system in the country, according to the credit rating agency.
11. Mass General Brigham has an “Aa3” rating and stable outlook with Moody’s and an “AA-” rating and stable outlook with S&P. The Boston-based health system has an excellent clinical reputation, good financial performance and strong balance sheet metrics, Moody’s said. The credit rating agency said it expects Mass General Brigham to maintain a strong market position and stable financial performance.
12. Rochester, Minn.-based Mayo Clinic has an “Aa2” rating and stable outlook with Moody’s. The credit rating agency said Mayo Clinic’s strong market position and patient demand will drive favorable financial results. The health system “will continue to leverage its excellent reputation and patient demand to continue generating favorable operating performance while maintaining strong balance sheet ratios,” Moody’s said.
13. Methodist Health System has an “Aa3” rating and stable outlook with Moody’s. The Dallas-based system has strong operating performance, and investments in facilities have allowed it to continue to capture more market share in the fast-growing Dallas-Fort Worth, Texas, area, Moody’s said. The credit rating agency said it expects Methodist Health System’s strong operating performance and favorable liquidity to continue.
14. Traverse City, Mich.-based Munson Healthcare has an “AA” rating and stable outlook with Fitch. The health system has a strong market position, a good payer mix and robust cash-to-adjusted debt levels, Fitch said. The credit rating agency expects the system to weather an expected period of weakened operating cash flow margins.
15. Albuquerque, N.M.-based Presbyterian Healthcare Services has an “Aa3” rating and stable outlook with Moody’s and an “AA” rating and stable outlook with Fitch. Presbyterian Healthcare Services is the largest health system in New Mexico, and it has strong revenue growth and a healthy balance sheet, Moody’s said. The credit rating agency said it expects the health system’s balance sheet and debt metrics to remain strong.
16. Chicago-based Rush Health has an “AA-” rating and stable outlook with Fitch. The health system has a strong financial profile and a broad reach for high-acuity services as a leading academic medical center, Fitch said. The credit rating agency expects Rush’s services to remain profitable over time.
17. Stanford (Calif.) Health Care has an “AA” rating and stable outlook with Fitch. The health system has extensive clinical reach in a competitive market and its financial profile is improving, Fitch said. The health system’s EBITDA margins rebounded in fiscal year 2021 and are expected to remain strong going forward, the crediting rating agency said.
18. University of Chicago Medical Center has an “AA-” rating and stable outlook with Fitch. The credit rating agency said it expects University of Chicago Medical Center’s capital-related ratios to remain strong, in part because of its broad reach of high-acuity services.
19. University of Iowa Hospitals and Clinics has an “Aa2” rating and stable outlook with Moody’s. The Iowa City-based health system, the only academic medical center in Iowa, has strong patient demand and excellent financial management, Moody’s said. The credit rating agency said it expects the health system to continue to manage the pandemic with improved operating cash flow margins.