

Cartoon – Our Financial Picture







The federal government has penalized 774 hospitals for having the highest rates of patient infections or other potentially avoidable medical complications. Those hospitals, which include some of the nation’s marquee medical centers, will lose 1% of their Medicare payments over 12 months.
The penalties, based on patients who stayed in the hospitals anytime between mid-2017 and 2019, before the pandemic, are not related to covid-19. They were levied under a program created by the Affordable Care Act that uses the threat of losing Medicare money to motivate hospitals to protect patients from harm.
On any given day, one in every 31 hospital patients has an infection that was contracted during their stay, according to the Centers for Disease Control and Prevention. Infections and other complications can prolong hospital stays, complicate treatments and, in the worst instances, kill patients.
“Although significant progress has been made in preventing some healthcare-associated infection types, there is much more work to be done,” the CDC says.
Now in its seventh year, the Hospital-Acquired Condition Reduction Program has been greeted with disapproval and resignation by hospitals, which argue that penalties are meted out arbitrarily. Under the law, Medicare each year must punish the quarter of general care hospitals with the highest rates of patient safety issues. The government assesses the rates of infections, blood clots, sepsis cases, bedsores, hip fractures and other complications that occur in hospitals and might have been prevented. The total penalty amount is based on how much Medicare pays each hospital during the federal fiscal year — from last October through September.
Hospitals can be punished even if they have improved over past years — and some have. At times, the difference in infection and complication rates between the hospitals that get punished and those that escape punishment is negligible, but the requirement to penalize one-quarter of hospitals is unbending under the law. Akin Demehin, director of policy at the American Hospital Association, said the penalties were “a game of chance” based on “badly flawed” measures.
Some hospitals insist they received penalties because they were more thorough than others in finding and reporting infections and other complications to the federal Centers for Medicare & Medicaid Services and the CDC.
“The all-or-none penalty is unlike any other in Medicare’s programs,” said Dr. Karl Bilimoria, vice president for quality at Northwestern Medicine, whose flagship Northwestern Memorial Hospital in Chicago was penalized this year. He said Northwestern takes the penalty seriously because of the amount of money at stake, “but, at the same time, we know that we will have some trouble with some of the measures because we do a really good job identifying” complications.
Other renowned hospitals penalized this year include Ronald Reagan UCLA Medical Center and Cedars-Sinai Medical Center in Los Angeles; UCSF Medical Center in San Francisco; Beth Israel Deaconess Medical Center and Tufts Medical Center in Boston; NewYork-Presbyterian Hospital in New York; UPMC Presbyterian Shadyside in Pittsburgh; and Vanderbilt University Medical Center in Nashville, Tennessee.
There were 2,430 hospitals not penalized because their patient complication rates were not among the top quarter. An additional 2,057 hospitals were automatically excluded from the program, either because they solely served children, veterans or psychiatric patients, or because they have special status as a “critical access hospital” for lack of nearby alternatives for people needing inpatient care.
The penalties were not distributed evenly across states, according to a KHN analysis of Medicare data that included all categories of hospitals. Half of Rhode Island’s hospitals were penalized, as were 30% of Nevada’s.
All of Delaware’s hospitals escaped punishment. Medicare excludes all Maryland hospitals from the program because it pays them through a different arrangement than in other states.
Over the course of the program, 1,978 hospitals have been penalized at least once, KHN’s analysis found. Of those, 1,360 hospitals have been punished multiple times and 77 hospitals have been penalized in all seven years, including UPMC Presbyterian Shadyside.
The Medicare Payment Advisory Commission, which reports to Congress, said in a 2019 report that “it is important to drive quality improvement by tying infection rates to payment.” But the commission criticized the program’s use of a “tournament” model comparing hospitals to one another. Instead, it recommended fixed targets that let hospitals know what is expected of them and that don’t artificially limit how many hospitals can succeed.
Although federal officials have altered other ACA-created penalty programs in response to hospital complaints and independent critiques — such as one focused on patient readmissions — they have not made substantial changes to this program because the key elements are embedded in the statute and would require a change by Congress.
Boston’s Beth Israel Deaconess said in a statement that “we employ a broad range of patient care quality efforts and use reports such as those from the Centers for Medicare & Medicaid Services to identify and address opportunities for improvement.”
UCSF Health said its hospital has made “significant improvements” since the period Medicare measured in assessing the penalty.
“UCSF Health believes that many of the measures listed in the report are meaningful to patients, and are also valid standards for health systems to improve upon,” the hospital-health system said in a statement to KHN. “Some of the categories, however, are not risk-adjusted, which results in misleading and inaccurate comparisons.”
Cedars-Sinai said the penalty program disproportionally punishes academic medical centers due to the “high acuity and complexity” of their patients, details that aren’t captured in the Medicare billing data.
“These claims data were not designed for this purpose and are typically not specific enough to reflect the nuances of complex clinical care,” the hospital said. “Cedars-Sinai continually tracks and monitors rates of complications and infections, and updates processes to improve the care we deliver to our patients.”
President Joe Biden has an unexpected opening to cut deals with red states to expand Medicaid, raising the prospect that the new administration could extend health protections to millions of uninsured Americans and reach a goal that has eluded Democrats for a decade.
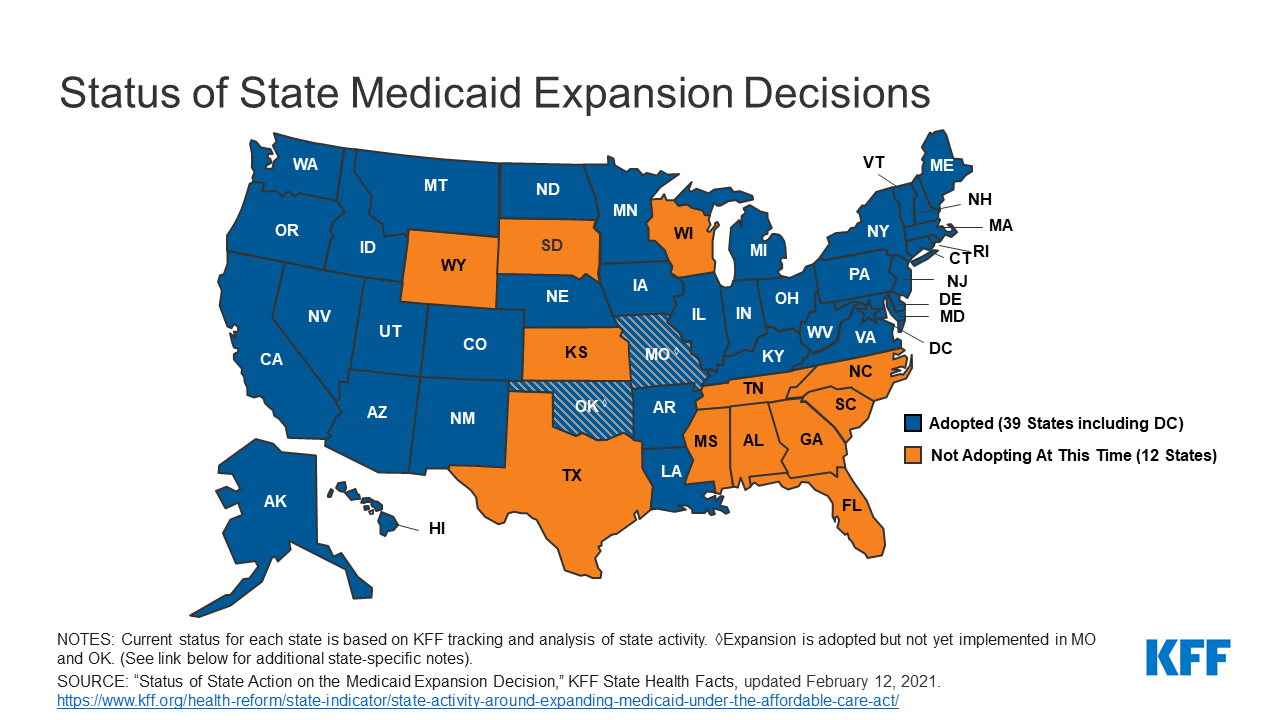
The opportunity emerges as the covid-19 pandemic saps state budgets and strains safety nets. That may help break the Medicaid deadlock in some of the 12 states that have rejected federal funding made available by the Affordable Care Act, health officials, patient advocates and political observers say.
Any breakthrough will require a delicate political balancing act. New Medicaid compromises could leave some states with safety-net programs that, while covering more people, don’t insure as many as Democrats would like. Any expansion deals would also need to allow Republican state officials to tell their constituents they didn’t simply accept the 2010 health law, often called Obamacare.
“Getting all the remaining states to embrace the Medicaid expansion is not going to happen overnight,” said Matt Salo, executive director of the nonpartisan National Association of Medicaid Directors. “But there are significant opportunities for the Biden administration to meet many of them halfway.”
Key to these potential compromises will likely be federal signoff on conservative versions of Medicaid expansion, such as limits on who qualifies for the program or more federal funding, which congressional Democrats have proposed in the latest covid relief bill.
But any deals would bring the country closer to fulfilling the promise of the 2010 law, a pillar of Biden’s agenda, and begin to reverse Trump administration efforts to weaken public programs, which swelled the ranks of the uninsured.
“A new administration with a focus on coverage can make a difference in how these states proceed,” said Cindy Mann, who oversaw Medicaid in the Obama administration and now consults extensively with states at the law firm Manatt, Phelps & Phillips.
Medicaid, the half-century-old health insurance program for the poor and people with disabilities, and the related Children’s Health Insurance Program cover more than 70 million Americans, including nearly half the nation’s children.
Enrollment surged following enactment of the health law, which provides hundreds of billions of dollars to states to expand eligibility to low-income, working-age adults.
However, enlarging the government safety net has long been anathema to most Republicans, many of whom fear that federal programs will inevitably impose higher costs on states.
And although the GOP’s decade-long campaign to “repeal and replace” the health law has largely collapsed, hostility toward it remains high among Republican voters.
That makes it perilous for politicians to embrace any part of it, said Republican pollster Bill McInturff, a partner at Public Opinion Strategies. “A lot of Republican state legislators are sitting in core red districts, looking over their shoulders at a primary challenge,” he said.
Many conservatives have called instead for federal Medicaid block grants that cap how much federal money goes to states in exchange for giving states more leeway to decide whom they cover and what benefits their programs offer.
Many Democrats and patient advocates fear block grants will restrict access to care. But just before leaving office, the Trump administration gave Tennessee permission to experiment with such an approach.
“It’s a frustrating place to be,” said Tom Banning, the longtime head of the Texas Academy of Family Physicians, which has labored to persuade the state’s Republican leaders to drop their opposition to expanding Medicaid. “Despite covid and despite all the attention on health and disparities, we see almost no movement on this issue.”
Some 1.5 million low-income Texans are shut out of Medicaid because the state has resisted expansion, according to estimates by KFF. (KHN is an editorially independent program of KFF.)
An additional 800,000 people are locked out in Florida, which has also blocked expansion.
Two million more are caught in the 10 remaining holdouts: Alabama, Georgia, Kansas, Mississippi, North Carolina, South Carolina, South Dakota, Tennessee, Wisconsin and Wyoming.
Advocates of Medicaid expansion, which is broadly popular with voters, believe they may be able to break through in a handful of these states that allow ballot initiatives, including Mississippi and South Dakota.
Since 2018, voters in Idaho, Nebraska, Utah, Oklahoma and Missouri have backed initiatives to expand Medicaid eligibility, effectively circumventing Republican political leaders.
“The work that we’ve done around the country shows that no matter where people live — red state or blue state — there is overwhelming support for expanding access to health care,” said Kelly Hall, policy director of the Fairness Project, a nonprofit advocacy group that has helped organize the Medicaid measures.
But most of the holdout states, including Texas, don’t allow citizens to put initiatives on the ballot without legislative approval.
And although Florida has an initiative process, mounting a ballot campaign there is challenging, as political advertising is expensive. Unlike in many states, Florida’s leading hospital association hasn’t backed expansion.
Another route for expansion: compromises that could win over skeptical Republican state leaders and still get the green light from the Biden administration.
The Obama administration approved conservative Medicaid expansion in Arkansas, which funneled enrollees into the commercial insurance market, and in Indiana, which forced enrollees to pay more for their medical care.
Money is a major focus of current talks in several states, according to health officials, advocates and others involved in efforts across the country.
The health law at first fully funded Medicaid expansion with federal money, but after the first three years, states had to begin paying part of the tab. Now, states must come up with 10% of the cost of expansion.
Even that small share is a challenge for states, many of which are reeling from the economic downturn caused by the pandemic, said David Becker, a health economist at the University of Alabama-Birmingham who has assisted efforts to expand Medicaid in that state.
“The question is: Where do we get the money?” Becker said, noting that some Republicans may be open to expanding Medicaid if the federal government pays the full cost of the expansion, at least for a year or two.
Other efforts to find ways to offset state costs are underway in Kansas and North Carolina, which have Democratic governors whose expansion plans have been blocked by Republican state legislators. Kansas Gov. Laura Kelly this month proposed using money from the sale and taxation of medical marijuana.
Some Democrats in Congress are pushing to revise the health law to provide full federal funding to states that expand Medicaid now. Separately, in the stimulus bill unveiled last week, House Democrats proposed an additional boost in total Medicaid aid to states that expand.
Other Republicans have signaled interest in partly expanding Medicaid, opening the program to people making up to 100% of the federal poverty level, or about $12,900, rather than 138%, or $17,800, as the law stipulated.
The Obama administration rejected this approach, but the idea has gained traction in several states, including Georgia.
It’s unclear what kind of compromises the new administration may consider, as Biden has yet to even nominate someone to oversee the Medicaid program.
Some Democrats say it’s time to give up the search for middle ground with Republicans on Medicaid.
A better strategy, they say, is a new government insurance plan, or public option, for people in non-expansion states, a strategy Biden endorsed on the campaign trail.
“Democrats can no longer countenance millions of Americans living in poverty without insurance,” said Chris Jennings, a Democratic health care strategist who worked in the White House under Presidents Bill Clinton and Barack Obama and served on Biden’s transition team.
“This is why the Biden public option or other new ways to secure affordable, meaningful care should become the order of the day for people living in states like Florida and Texas.”

The latest analysis from the think tank provides a fuller picture of how the COVID-19 pandemic influenced admission trends throughout 2020.
Overall, total admissions bottomed out in April and March but have remained near normal, or above 90% of expected admissions since June, according to electronic medical record data from the Epic Health Research Network, which pools information from 20 million patients across 97 hospitals in the U.S.
However, while total admissions — which includes those sick with COVID-19 — remained near normal, the pattern differed when zeroing in on non-COVID-19 admissions, or those admitted who did not have the virus.
Non-COVID-19 admissions started to fall again in November and by Dec. 5 they fell to 80% of expected volume, which is likely to put financial pressure on hospitals, particularly those with smaller reserves of cash on hand, Kaiser noted.
The decline was steepest in the Midwest and West, dropping to about 76% of expected volume between early November and December.
Researchers fear the drop in non-COVD-19 admissions may have long-term consequences.
“The levels of non-COVID-19 admissions seen in the fall of 2020 suggest that people may be delaying care in ways that could be harmful to their long-term health,” according to the study.
Insurers observed similar patterns of depressed volume in the fourth quarter.
Humana, which largely covers seniors in Medicare plans, noted non-COVID-19 volume dropped the last two months of the quarter after previously returning to near normal. It led Humana to report a loss in the fourth quarter as COVID-19 testing and treatment accelerated. Centene, which reported a Q4 loss, echoed a similar pattern.
