Cartoon – Lying or Perfecting the Truth?






https://one.npr.org/?sharedMediaId=968920752:968920754
Employers — including companies, state governments and universities — purchase health care on behalf of roughly 150 million Americans. The cost of that care has continued to climb for both businesses and their workers.
For many years, employers saw wasteful care as the primary driver of their rising costs. They made benefits changes like adding wellness programs and raising deductibles to reduce unnecessary care, but costs continued to rise. Now, driven by a combination of new research and changing market forces — especially hospital consolidation — more employers see prices as their primary problem.
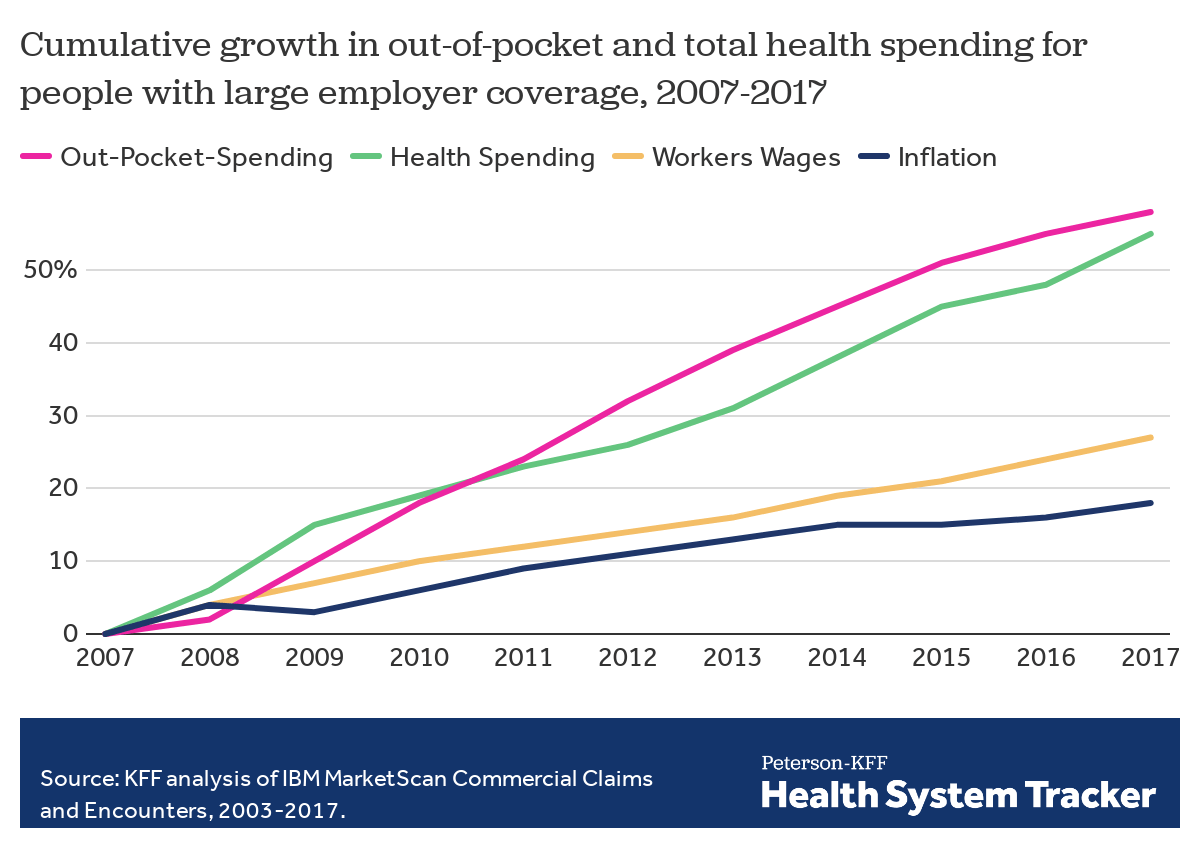
The prices employers pay hospitals have risen rapidly over the last decade. Those hospitals provide inpatient care and increasingly, as a result of consolidation, outpatient care too. Together, inpatient and outpatient care account for roughly two-thirds of employers’ total spending per employee.
By amassing and analyzing employers’ claims data in innovative ways, academics and researchers at organizations like the Health Care Cost Institute (HCCI) and RAND have helped illuminate for employers two key truths about the hospital-based health care they purchase:
Data show that providers charge private payers very different prices for the exact same services — even within the same geographic area.
For example, HCCI found the price of a C-section delivery in the San Francisco Bay Area varies between hospitals by as much as:$24,107
Research also shows that facilities with higher prices do not necessarily provide higher quality care.
Data show that hospitals charge employers and private insurers, on average, roughly twice what they charge Medicare for the exact same services. A recent RAND study analyzed more than 3,000 hospitals’ prices and found the most expensive facility in the country charged employers:4.1xMedicare
Hospitals claim this price difference is necessary because public payers like Medicare do not pay enough. However, there is a wide gap between the amount hospitals lose on Medicare (around -9% for inpatient care) and the amount more they charge employers compared to Medicare (200% or more).
A small but growing group of companies, public employers (like state governments and universities) and unions is using new data and tactics to tackle these high prices. (Learn more about who’s leading this work, how and why by listening to our full podcast episode in the player above.)
Note that the employers leading this charge tend to be large and self-funded, meaning they shoulder the risk for the insurance they provide employees, giving them extra flexibility and motivation to purchase health care differently. The approaches they are taking include:
Some employers are implementing so-called tiered networks, where employees pay more if they want to continue seeing certain, more expensive providers. Others are trying to strongly steer employees to particular hospitals, sometimes know as centers of excellence, where employers have made special deals for particular services.
Purdue University, for example, covers travel and lodging and offers a $500 stipend to employees that get hip or knee replacements done at one Indiana hospital.
There is a movement among some employers to renegotiate hospital deals using Medicare rates as the baseline — since they are transparent and account for hospitals’ unique attributes like location and patient mix — as opposed to negotiating down from charges set by hospitals, which are seen by many as opaque and arbitrary. Other employers are pressuring their insurance carriers to renegotiate the contracts they have with hospitals.
In 2016, the Montana state employee health plan, led by Marilyn Bartlett, got all of the state’s hospitals to agree to a payment rate based on a multiple of Medicare. They saved more than $30 million in just three years. Bartlett is now advising other states trying to follow her playbook.
In 2020, several large Indiana employers urged insurance carrier Anthem to renegotiate their contract with Parkview Health, a hospital system RAND researchers identified as one of the most expensive in the country. After months of tense back-and-forth, the pair reached a five-year deal expected to save Anthem customers $700 million.
Some employer coalitions are advocating for more intervention by policymakers to cap health care prices or at least make them more transparent. States like Colorado and Indiana have passed price transparency legislation, and new federal rules now require more hospital price transparency on a national level. Advocates expect strong industry opposition to stiffer measures, like price caps, which recently failed in the Montana legislature.
Other advocates are calling for more scrutiny by state and federal officials of hospital mergers and other anticompetitive practices. Some employers and unions have even resorted to suing hospitals like Sutter Health in California.
Employers face a few key barriers to purchasing health care in different and more efficient ways:
Hospitals tend to have much more market power than individual employers, and that power has grown in recent years, enabling them to raise prices. Even very large employers have geographically dispersed workforces, making it hard to exert much leverage over any given hospital. Some employers have tried forming purchasing coalitions to pool their buying power, but they face tricky organizational dynamics and laws that prohibit collusion.
Employers can attempt to lower prices by renegotiating contracts with hospitals or tailoring provider networks, but the work is complicated and rife with tradeoffs. Few employers are sophisticated enough, for example, to assess a provider’s quality or to structure hospital payments in new ways. Employers looking for insurers to help them have limited options, as that industry has also become highly consolidated.
Employers say they primarily provide benefits to recruit and retain happy and healthy employees. Many are reluctant to risk upsetting employees by cutting out expensive providers or redesigning benefits in other ways. A recent KFF survey found just 4% of employers had dropped a hospital in order to cut costs.
Employers play a unique role in the United States health care system, and in the lives of the 150 million Americans who get insurance through work. For years, critics have questioned the wisdom of an employer-based health care system, and massive job losses created by the pandemic have reinforced those doubts for many.
Assuming employers do continue to purchase insurance on behalf of millions of Americans, though, focusing on lowering the prices they pay is one promising path to lowering total costs. However, as noted above, hospitals have expressed concern over the financial pressures they may face under these new deals. Complex benefit design strategies, like narrow or tiered networks, also run the risk of harming employees, who may make suboptimal choices or experience cost surprises. Finally, these strategies do not necessarily address other drivers of high costs including drug prices and wasteful care.

The complexity of Medicare Advantage (MA) physician networks has been well-documented, but the payment regulations that underlie these plans remain opaque, even to experts. If an MA plan enrollee sees an out-of-network doctor, how much should she expect to pay?
The answer, like much of the American healthcare system, is complicated. We’ve consulted experts and scoured nearly inscrutable government documents to try to find it. In this post we try to explain what we’ve learned in a much more accessible way.
Medicare Advantage Basics
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third of the 60+ million Americans covered by Medicare are enrolled in MA plans. These plans, subsidized by the government, are governed by Medicare rules, but, within certain limits, are able to set their own premiums, deductibles, and service payment schedules each year.
Critically, they also determine their own network extent, choosing which physicians are in- or out-of-network. Apart from cost sharing or deductibles, the cost of care from providers that are in-network is covered by the plan. However, if an enrollee seeks care from a provider who is outside of their plan’s network, what the cost is and who bears it is much more complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers, which constitute about 97% of all physicians in the U.S., accept Medicare Fee-For-Service (FFS) rates for full payment of their services. These are the rates paid by TM. These doctors are subject to the fee schedules and regulations established by Medicare and MA plans.
Non-participating providers (about 2% of practicing physicians) can accept FFS Medicare rates for full payment if they wish (a.k.a., “take assignment”), but they generally don’t do so. When they don’t take assignment on a particular case, these providers are not limited to charging FFS rates.
Opt-out providers don’t accept Medicare FFS payment under any circumstances. These providers, constituting only 1% of practicing physicians, can set their own charges for services and require payment directly from the patient. (Many psychiatrists fall into this category: they make up 42% of all opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So, if an MA beneficiary goes to see an out-of-network doctor, by whom does the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member willingly seeks care from an out-of-network provider, the member assumes full liability for payment. That is, neither the HMO plan nor TM will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies, and must be disclosed to the patient before any services are administered. If the provider is participating with Medicare (in the sense defined above), they charge the patient no more than the standard Medicare FFS rate for their services. Non-participating providers that do not take assignment on the claim are limited to charging the beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states further restrict this. In New York State, for instance, the maximum is 105% of Medicare FFS payment.) In these cases, the provider charges the patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare, there are no limits to what they can charge for their services. The provider and patient enter into a private contract; the patient agrees to pay the full amount, out of pocket, for all services.
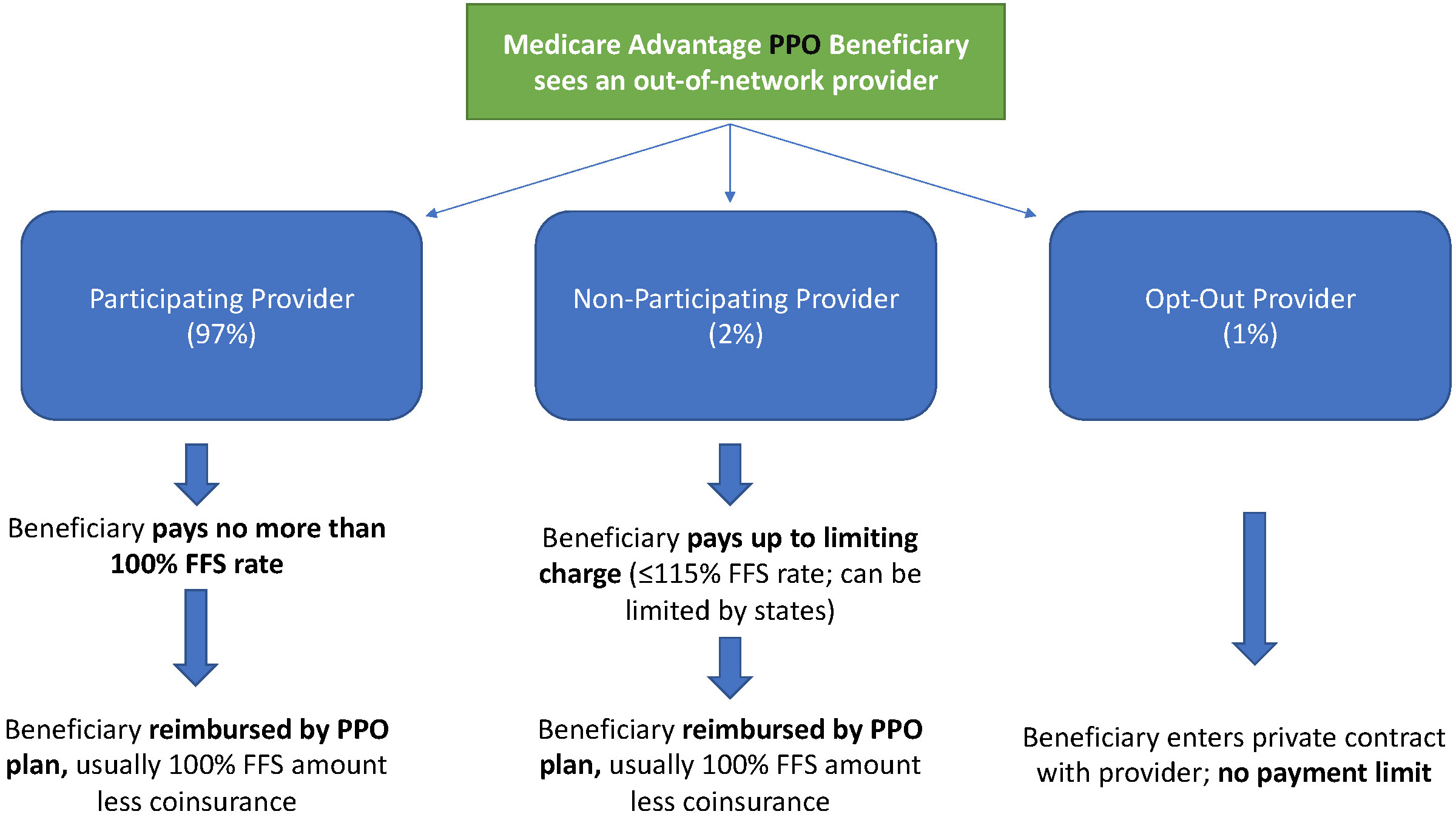
MA PPO plans operate slightly differently. By nature of the PPO plan, there are built-in benefits covering visits to out-of-network physicians (usually at the expense of higher annual deductibles and co-insurance compared to HMO plans). Like with HMO enrollees, an out-of-network Medicare-participating physician will charge the PPO enrollee no more than the standard FFS rate for their services. The PPO plan will then reimburse the enrollee 100% of this rate, less coinsurance. (See Figure 2.)
In contrast, a non-participating physician that does not take assignment is limited to charging a PPO enrollee 115% of the Medicare FFS amount, which can be further limited by state regulations. In this case, the PPO enrollee is also reimbursed by their plan up to 100% (less coinsurance) of the FFS amount for their visit. Again, opt-out physicians are exempt from these regulations and must enter private contracts with patients.
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare) and the provider happens to be out-of-network for the MA plan (regardless of HMO/PPO status), the plan must cover the services at their established in-network emergency services rates.
The second caveat is in regard to the declared public health emergency due to COVID-19 (set to expire in April 2021, but likely to be extended). MA plans are currently required to cover all out-of-network services from providers that contract with Medicare (i.e., all but opt-out providers) and charge beneficiaries no more than the plan-established in-network rates for these services. This is being mandated by CMS to compensate for practice closures and other difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside of the pandemic and emergency situations, knowing how much you’ll need to pay for out-of-network services as a MA enrollee depends on a multitude of factors. Though the vast majority of American physicians contract with Medicare, the intersection of insurer-engineered physician networks and the complex MA payment system could lead to significant unexpected costs to the patient.
The Affordable Care Act (ACA) made historic strides in expanding access to health insurance coverage by covering an additional 20 million Americans. President Joe Biden ran on a platform of building upon the ACA and filling in its gaps. With Democratic majority in the Senate, aspects of his health care plan could move from idea into reality.
The administration’s main focus is on uninsurance, which President Biden proposes to tackle in three main ways: providing an accessible and affordable public option, increasing tax credits to help lower monthly premiums, and indexing marketplace tax credits to gold rather than silver plans.
However, underinsurance remains a problem. Besides the nearly 29 million remaining uninsured Americans, over 40% of working age adults are underinsured, meaning their out-of-pocket cost-sharing, excluding premiums, are 5-10% of household income or more, depending on income level.
High cost-sharing obligations—especially high deductibles—means insurance might provide little financial protection against medical costs beneath the deductible. Bills for several thousand dollars could financially devastate a family, with the insurer owing nothing at all. Recent trends in health insurance enrollment suggest that uninsurance should not be the only issue to address.
A high demand for low premiums
Enrollment in high deductible health plans (HDHP) has been on a meteoric rise over the past 15 years, from approximately 4% of people with employer-sponsored insurance in 2006 to nearly 30% in 2019, leading to growing concern about underinsurance. “Qualified” HDHPs, which come with additional tax benefits, generally have lower monthly premiums, but high minimum deductibles. As of 2020, the Internal Revenue Service defines HDHPs as plans with minimum deductibles of at least $1,400 for an individual ($2,800 for families), although average annual deductibles are $2,583 for an individual ($5,335 for families).
HDHPs are associated with delays in both unnecessary and necessary care, including cancer screenings and treatment, or skipped prescription fills. There is evidence that Black patients disproportionately experience these effects, which may further widen racial health inequities.
A common prescription has been to expand access to Health Savings Accounts (HSAs), with employer and individual contributions offsetting higher upfront cost-sharing. Employers often contribute on behalf of their employees to HSAs, but for individuals in lower wage jobs without such benefits or without extra income to contribute themselves, the account itself may sit empty, rendering it useless.
A recent article in Health Affairs found that HDHP enrollment increased from 2007 to 2018 across all racial, ethnic, and income groups, but also revealed that low-income, Black, and Hispanic enrollees were significantly less likely to have an HSA, with disparities growing over time. For instance, by 2018, they found that among HDHP enrollees under 200% of the federal poverty level (FPL), only 21% had an HSA, while 52% of those over 400% FPL had an HSA. In short, the people who could most likely benefit from an HSA were also least likely to have one.
If trends in HDHP enrollment and HSA access continue, it could result in even more Americans who are covered on paper, yet potentially unable to afford care.
Addressing uninsurance could also begin to address underinsurance
President Biden’s health care proposal primarily addresses uninsurance by making it more affordable and accessible. This can also tangentially tackle underinsurance.
To make individual market insurance more affordable, Biden proposes expanding the tax credits established under the ACA. His plan calls for removing the 400% FPL cap on financial assistance in the marketplaces and lowering the limit on health insurance premiums to 8.5% of income. Americans would now be able to opt out of their employer plan if there is a better deal on HealthCare.gov or their state Marketplace. Previously, most individuals who had an offer of employer coverage were ineligible for premium subsidies—important for individuals whose only option might have been an employer-sponsored HDHP.
Biden also proposes to index the tax credits that subsidize premiums to gold plans, rather than silver plans as currently done. This would increase the size of these tax credits, making it easier for Americans to afford more generous plans with lower deductibles and out-of-pocket costs, substantially reducing underinsurance.
The most ambitious of Biden’s proposed health policies is a public option, which would create a Medicare-esque offering on marketplaces, available to anyone. As conceived in Biden’s proposal, such a plan would eliminate premiums and having minimal-to-no cost-sharing for low-income enrollees; especially meaningful for under- and uninsured people in states yet to expand Medicaid.
Moving forward: A need to directly address underinsurance
More extensive efforts are necessary to meaningfully address underinsurance and related inequities. For instance, the majority of persons with HDHPs receive coverage through an employer, where the employer shares in paying premiums, yet cost-sharing does not adjust with income as it can in the marketplace. Possible solutions range from employer incentives to expanding the scope of deductible-exempt services, which could also address some of the underlying disparities that affect access to and use of health care.
The burden of high cost-sharing often falls on those who cannot afford it, while benefiting employers, healthy employees, or those who can afford large deductibles. Instead of encouraging HSAs, offering greater pre-tax incentives that encourage employers to reabsorb some of the costs that they have shifted on their lower-income employees could prevent the income inequity gap from widening further.
Under the ACA, most health insurance plans are required to cover certain preventative services without patient cost-sharing. Many health plans also exempt other types of services from the deductible – from generic drugs to certain types of specialist visits – although these exemptions vary widely across plans. Expanding deductible-exempt services to include follow-up care or other high-value services could improve access to important services or even medication adherence without high patient cost burden. Better educating employees about what services are exempt would make sure that patients aren’t forgoing care that should be fully covered.
Health insurance is complicated. Choosing a plan is only the start. More affordable choices are helpful only if these choices are fully understood, e.g., the tradeoff between an HDHP’s lower monthly premium and the large upfront out-of-pocket cost when using care. Investing in well-trained, diverse navigators to help people understand how their options work with their budget and health care needs can make a big difference, given that low health insurance literacy is related to higher avoidance of care.
The ACA helped expand coverage, but now it’s time to make sure the coverage provided is more than an unused insurance card. The Biden administration has the opportunity and responsibility to make progress not only on reducing the uninsured rate, but also in reducing disparities in access and patient affordability.