Dems hit GOP on pre-existing conditions at panel’s first policy hearing

The powerful House Ways and Means Committee used its first policy hearing of the new Congress to hammer Republicans on pre-existing conditions, an issue that helped propel Democrats into the majority during the 2018 midterm elections.
Democratic panel members highlighted actions by the Trump administration that they argue have hurt people with pre-existing conditions, like the expansion of non-ObamaCare plans that could draw healthy people from the markets, raising premiums for those left behind.
The administration has expanded access to association and short-term health plans, which cost less than ObamaCare plans but cover fewer services. Republicans say they provide an off-ramp for consumers who can’t afford ObamaCare plans.
The witness invited by Republicans, Rob Robertson with the Nebraska Farm Bureau, said its newly developed association health plan “meets the needs of our members,” who can’t afford ObamaCare plans.
“We’re in this for the long term,” he told lawmakers. “We want to reduce costs, and the costs in the individual market are very, very high.”
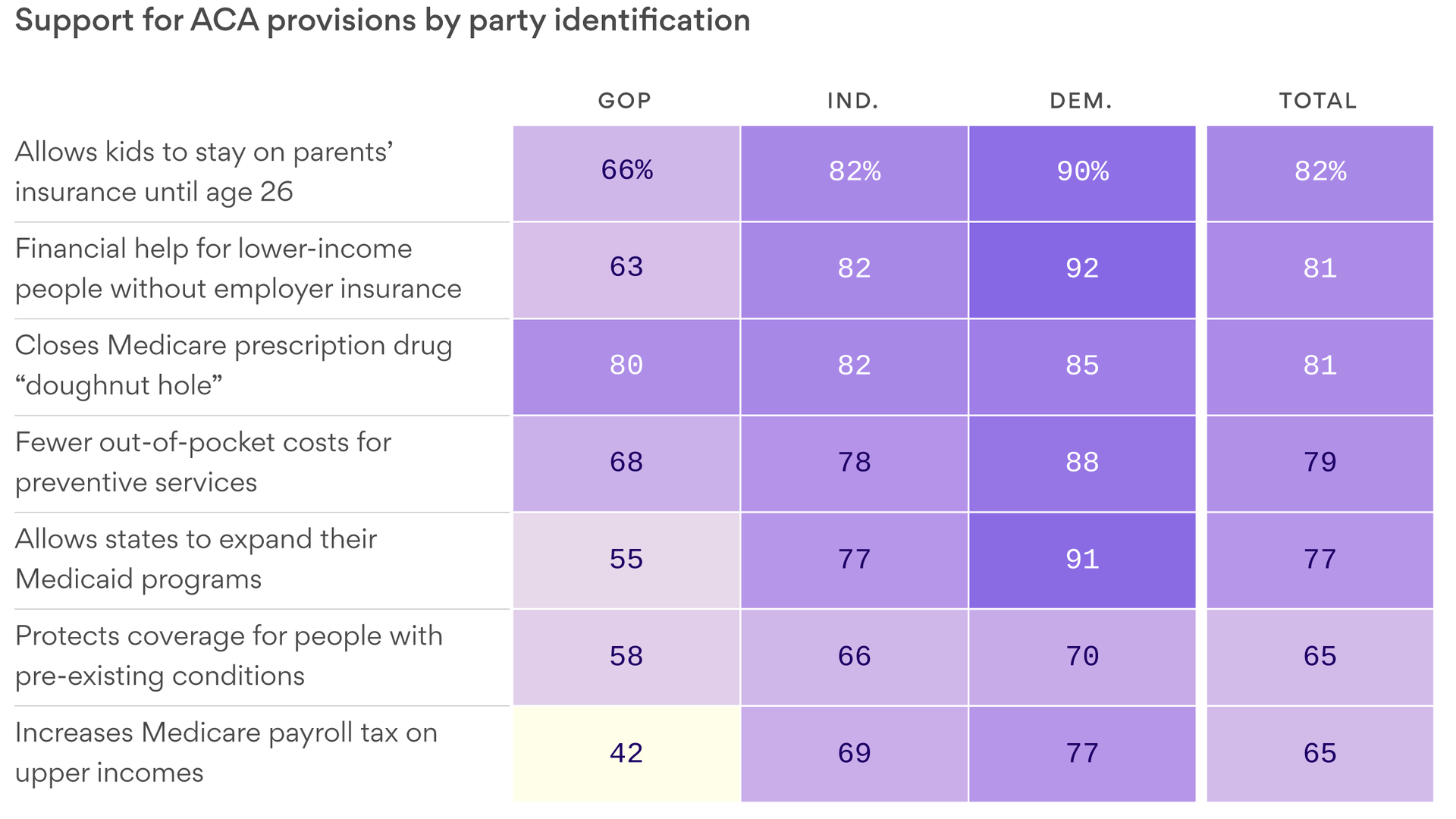
ObamaCare’s popular consumer protections became the centerpiece of the November midterms after 20 Republican-led states sued to overturn the 2010 health care law, known as the Affordable Care Act (ACA).
Democrats tied congressional Republicans to the lawsuit after the Trump administration declined to defend ObamaCare and argued that those protections are unconstitutional.
Republicans say there are different ways to cover people with pre-existing conditions, like high-risk pools, which were banned after ObamaCare was implemented. Some pools had caps on coverage and long-waiting lists.
GOP committee members called Tuesday’s hearing political theatre, arguing they also support pre-existing protections but want to lower ObamaCare’s costs.
“Everyone up here wants protections for people with pre-existing conditions. Always have, always will,” said Rep. Devin Nunes (R-Calif.), ranking member of the health subcommittee. “We should be careful that we’re not stoking fear that someone is going to lose their health insurance. We have a responsibility to come up with a better health care system because ObamaCare is not the solution.”
Democrats on Tuesday said the GOP proposals aren’t serious.
Republicans have “political amnesia” and have “forgotten what it was like before the ACA,” said Rep. Lloyd Doggett (D-Texas), chairman of the health subcommittee. “Those with a diagnosis of a serious disease would also get a diagnosis of financial ruin. There were no protections for them before the ACA.”
Some Democratic panel members appealed to the emotional side of the health care debate, with one lawmaker announcing her cancer diagnosis at the hearing.
“This is a cancer I will live with for the rest of my life, but, because of my high-quality healthcare and insurance coverage, it is not a cancer I will die from,” said Rep. Gwen Moore (D-Wis.), 67.
Tensions ran high at times during Tuesday’s hearing, with members re-litigating the 2010 passage of ObamaCare and repeated GOP efforts to repeal it.
“Not one Republican up here supports pre-existing protections for the American people,” said Rep. Brian Higgins (D-N.Y.), who at times pounded his fist on the dais.
That drew a testy response from Rep. Tom Reed (R-Pa.), who said Republicans “heard the voices and the fear” from voters in the 2018 midterms when “this issue became the centerpiece.”
“We listened to this American people, as Republicans,” he said.