The U.S. health system’s future is uncertain but outside forces will define its direction.
9 structural changes appear necessary to a transformed system of health that’s affordable, comprehensive and effective.
Last week, I had a 27-hour stay in a hospital emergency room waiting for an open bed and a morning at the food pantry loading boxes in anticipation of a possible SNAP program suspension surge. It wasn’t the week I expected. So much for plans!
Such is the case for health insurance coverage for millions in the U.S. as the federal government shutdown enters Week 6. Democrats are holding out for continuation of Affordable Care Act (ACA) insurance subsidies that enable 22 million to “buy” insurance cheaper, and Republicans are holding out for federal spending cuts reflected in the One Big Beautiful Act (July 2025) that included almost a trillion reduction in Medicaid appropriations thru 2036.
ACA subsidies at the heart of the shutdown successfully expanded coverage in tandem with Medicaid expansion but added to its costs and set in motion corporatization and consolidation in every sector of the health system. The pandemic exposed the structural divide between public health programs and local health systems, and insurance premium increases and prior authorization protocols precipitated hostility toward insurers and blame games between hospitals, insurers and drug companies for perpetual cost increases.
Having mediated discussions between the White House and industry trade groups as part of the ACA’s design (2009), I witnessed first hand the process of its development into law, the underlying assumptions on which it is based and the politics before and after its passage in March 2010. Its hanging chads were obvious. Its implementation stalled. Its potential to lower costs and improve quality never realized. It was a Plan disabled by special interests that rightly exploited its flaws and political brinksmanship that divided the country. But more fundamentally, it has failed to lower costs and improve affordability because it failed to integrate outside considerations—private capital, employers, technologies, clinical innovations and consumer finances—in its calculus.
Sixteen years later, healthcare is once again the eye of the economic storm. Insiders blame inconsistent regulatory enforcement and lack of adequate funding as root causes. Outsiders blame lack of cost controls. consolidation and disregard for affordability. Thus, while attention to subsidized insurance coverage and SNAP benefits might temporarily calm public waters, they’re not the solution.
All parties and all sides seem to agree the health system broken. For example, in my trustee surveys before planning sessions with Boards of health systems, medical groups and insurers, the finding is clear:
92% says the future of the U.S. health system in 7-10 years is fundamentally changed and not repeat of its past.
84% say their organizations are not prepared because short-term issues limit their ability to long-term planning.
Republicans think market forces will fix it. Democrats think federal policy will fix it. The public thinks it’s become Big Business that puts its interests before theirs. And the industry’s trade groups—AMA, AHA, AHIP, PhRMA, Adame, APHA, et al—face intense pressure from members adversely impacted by unwanted regulatory policies.
Few enjoy the luxury of long-term planning. That doesn’t excuse the need to address it. If a clear path to the system’s future is not built, incrementalism will enable its inevitable insolvency and forced re-construction.
What’s the solution? When comparing the U.S. health system to high performing systems in other high-income countries, these findings jump out:
All spend less on healthcare services and more on social services than the U.S.
All include government and privately-owned operators
All fund their systems primarily through a combination of federal appropriations and private payments by employers and citizens.
All pursue clinical standardization based on evidence.
All are dealing with funding constraints as their governments address competing priorities.
All are transitioning from episodic to chronic health as their populations age and healthiness erodes.
All are focused on workforce modernization and technologic innovations to lower costs and reduce demand for specialty services.
All enable private investment in their systems to increase competition and stimulate innovation.
All facilitate local/regional regulatory oversight to address distinctions in demand and resources.
All face with growing public dissatisfaction.
All are expensive to operate.
No system is perfect. None offers a copy-paste solution for U.S. taxpayers. And even if one seemed dramatically better, it would be a generational surge rooted in futility that welcome it.
What’s the answer? At the risk of oversimplicity, the future seems most likely built on these 9 structural changes:
Integrate social services (public health) with delivery.
Create comprehensive primary and preventive health gatekeeping inclusive of physical and behavioral health, nutrition, prophylactic dentistry and consumer education.
Rationalize specialty services and therapies to high value providers.
Incentivize responsible health behaviors across the entire population.
Increase private capital investments in healthcare.
Modernize the workforce.
Fund the system strategically.
Define and disclose affordability, quality and value systemically.
Facilitate technology-enabled self-care.
This will not happen quickly nor result from current momentum: the inertia of the status quo leans substantially toward protectionism not because it’s unaware. The risks are high. And while the majority of Americans are frustrated by its performance, there’s no referent to which look as a better mousetrap.
I anticipated last week would be pretty uneventful. It wasn’t. My Plan didn’t work out due, in part, to circumstances I didn’t foresee or control.
Healthcare’s the same. Outside forces seen or not will impact its future dramatically. Plans have to be made though Black Swans like the pandemic are inevitable. But long-term planning built on plausible bets are necessary to every healthcare organization’s future.
America’s health care system is neither healthy, caring, nor a system.
– Walter Cronkite
Healthcare policy in America is too short-sighted and vulnerable to party-politics. We need a system that’s built to last.
As open enrollment through the ACA marketplace begins November 1, millions of Americans will soon discover their health insurance rates going up in 2026 as the direct result of ACA tax subsidies expiring because party politicians in charge of the Senate refuse to budge. If you know how much your rates will be increasing in 2026, please share so I can see the impact that this inaction will have on regular folks.
Career politicians like my opponent Mike Rounds aren’t willing to stray from the party line to make sure Americans and their families get affordable healthcare, and in the process they are causing innumerable harm to not just those Americans on ACA, but also all the furloughed federal employees and families on SNAP. Something needs to change.
As an Independent candidate who supports pragmatic solutions, I will not claim my proposals are the best or only choices, but I will claim just about anything will be overall less expensive and more effective than the status quo. The bottom line is that our dysfunctional politics have us fighting over half-measure solutions to today’s problems instead of complete solutions to tomorrow’s.
Overhauling American healthcare is a complex challenge, but that cannot let it deter us. Americans deserve access to affordable, quality care. According to a KFF analysis, healthcare accounted for 27% of federal spending in fiscal year 2024. The U.S. spends far more per person on healthcare than any of the other 37 members of the Organization for Economic Co-operation and Development (OECD). Despite spending nearly twice as much per person as similar wealthy countries, we still rank poorly on key health outcomes.
America does, however, hold a commanding lead in medical debt, accounting for between 50% and 66% of annual personal bankruptcies. Other wealthy countries clearly understand better how to set up a healthcare system that is both less expensive and produces the same or better outcomes.
Considering the immense costs and mediocre outcomes, I am reminded of the famous observation from Dr. Amos Wilson: “If you want to understand any problem in America, you need to look at who profits from that problem, not at who suffers from that problem.” Having done so, I support an incremental reinvention of the American healthcare system that doesn’t just solve immediate problems such as premium hikes, expiring ACA subsidies, or Medicare cuts, but also secures a stable and healthy future for the American people.
My plan for America’s healthcare system has three basic steps, ensuring folks can get the care they need, now and in the future.
Stage 1: Fixing the Supply Side: Regulate Healthcare Companies, Lower Drug Prices, & Encourage Preventive Care
The healthcare industry (from insurers to providers) is a functional monopoly, especially at the local/regional level, similar to electric, gas, and telecommunications companies. It deserves to be treated the same way. Drawing from how the South Dakota Public Utilities Commission (and similar entities in other states) regulate utility companies to ensure that they provide “reliable service” and “reasonable rates,” creating a regulatory framework for healthcare companies (including insurers) is a good first step in adapting our current system into one that considers the needs of regular folks. Providers shouldn’t have to butt heads with insurers to provide the services that patients need, so creating a more transparent and regulated system would benefit every level of the process.
Pharmaceutical companies have the highest profit margins in the healthcare industry. According to a RAND report, Americans pay 278% higher prescription drug prices than similar countries where the government negotiates drug pricing. The common-sense solution is for the federal government to negotiate pricing for all drugs. Doing so will yield much greater savings for both the government and consumers.
To offset reduced pharmaceutical company profits and also help more consumers, the U.S. should negotiate a treaty with the European Union and other G7 countries to establish a pharmaceutical common market based on uniform drug development/approval standards enabling the elimination of trade barriers for drugs.
RFK Jr.’s “Make America Healthy Again” (MAHA) agenda includes multiple nonsensical proposals that are likely to do the opposite, but there are a handful of beneficial ideas. A MAHA focus on preventive care that strengthens primary care, expands access to screenings, and incentivizes healthy lifestyles will lower long-term healthcare spending the same way that keeping up routine maintenance on your car prevents big repair bills in the future.
Investing in community health centers, mobile clinics, and telehealth services will make preventive care more accessible, particularly in underserved rural and urban areas. Similarly, reducing reliance on highly processed foods and ensuring government nutrition assistance programs incentivize and enable healthy foods would also pay dividends.
Many states approve the rates that insurers charge consumers, but these rates increase as the base cost of providing healthcare services increases. Holding healthcare companies, providers and insurers alike, to uniform standards and making information transparently available for comparison will remove the various pressures driving up the cost of care, keeping rates down for consumers.
Stage 2: Fixing the Demand Side: Create a Public Option, Streamline Administration, Increase Residency Slots
Profits are up 230% for the top 5 health insurance companies since the Affordable Care Act (ACA) was adopted, while family premiums have also skyrocketed. While I think it was a step in the right direction to provide folks with healthcare, it isn’t a viable permanent solution. Creating a broadly available public option would enable Americans to buy into a health insurance plan administered by the government.
A public option like this wouldn’t have a profit motive, so it would be able to offer lower-cost plans, creating a baseline for other companies to compete with. Increased competition would drive down premiums and improve quality of service across the market, even amongst private for-profit insurers.
Technology can also help lower costs by reducing the complicated bureaucracy healthcare administrators must navigate. Healthcare providers currently spend enormous time and money dealing with insurance paperwork, eligibility verification, and billing disputes. Universally interoperable electronic health records (EHRs) and streamlined billing systems would significantly reduce costs. Uniform standards for these processes and better technology infrastructure would free up providers’ time to focus more on patient care.
By 2036, the U.S. is projected to need 86,000 more physicians than it will have. The primary cause of the growing shortage is a 1997 law freezing federal support for Medicare-funded residency positions. Limiting the number of doctors in training also fosters misallocation of training slots across the country, creating a mismatch between where they train and where they are needed most. Correcting this self-inflicted shortage is essential to maximizing access.
On the subject of innovative approaches to providing healthcare, fee-for-service payment models reward volume over value, encouraging unnecessary tests and procedures. Transitioning to value-based care, where providers are paid based on patient outcomes, can lead to better health outcomes at a lower cost. Accountable Care Organizations (ACOs), bundled payments, and capitation models (in which providers receive a fixed fee per patient for a specific time period regardless of services delivered) have shown promise in reducing spending while maintaining or improving quality.
Stage 3: Use The Foundation To Build a Better System
While I believe that our leaders today should be looking towards the future with long-lasting solutions rather than scrambling for band-aid policies, I also know that we shouldn’t put the cart before the horse. I believe that Stages 1 and 2 lay the foundation for a healthier America and a more streamlined healthcare system. Stage 3 of my plan is geared towards keeping our options open for the future of American healthcare.
All OECD countries with lower per-person healthcare spending provide universal or near-universal coverage to their citizens. Various universal healthcare systems seem to be an effective way to improve access and reduce systemic costs. In particular, I think that looking to our allies such as Canada (with a single-payer system) and Germany (with a multi-payer system) would be a good place to start. In both systems, the government negotiates prices directly with providers and pharmaceutical companies, leading to significant cost savings for consumers.
Conclusion
In summary, the American healthcare system doesn’t suffer from a lack of resources but rather anti-competitive profit-seeking, inefficiency, and a lack of imagination. Creative solutions lie in addressing the supply and demand side of the healthcare industry, continuously blending technological innovation, community-based delivery, and incentivizing healthier living.
No single policy will fix the U.S. healthcare system overnight, but a combination of reforms can dramatically improve access and lower costs. Providing a public option is a foundational step that keeps options open for other innovations. In tandem, reforms such as drug price negotiation, investment in preventive care, value-based payments, and administrative simplification can deliver a more efficient and equitable healthcare system. Political will and public support are crucial, but the long-term benefits for individuals, businesses, and the broader economy make these changes not only possible but necessary.
The path forward is not and cannot be a purely partisan choice of public versus private. It must be guided solely by a simple question: What is most effective at making healthcare cheaper, faster, and more accessible for everyone? At this point, I believe a robust public option is essential, but I remain unsure whether a single-payer or a refined version of a multi-payer universal system is warranted. I’m keeping an open mind.
I am sure that Washington politicians shouldn’t be screwing over regular Americans by making their healthcare inaccessible or more expensive. As South Dakota’s Independent senator, I would be empowered to break through party-first politics to make sure people always come first.
The American healthcare is complicated, so this article leans on the longer side to try and do it justice. Thank you for reading.
For four years, people buying health care on the Affordable Care Act (ACA) marketplace have benefited from government subsidies that made their plans more inexpensive, and thus more accessible.
Now, those subsidies have become a key point of contention between Democrats and Republicans in a government shutdown that went into effect on Oct. 1 after both sides failed to reach a deal.
Democrats want Congress to extend the enhanced premium tax credits first added in 2021; without an extension, the tax credits expire at the end of 2025 and experts say premium prices could double in 2026.
“They know they’re screwed if this debate turns into one about healthcare. And guess what? That’s just what we’re doing. We are making this debate a debate on healthcare,” said U.S. Senator Chuck Schumer, a Democrat from New York, hours before the government shut down.
Republicans say that Democrats want to extend free health care for unauthorized immigrants, a talking point that is not true but that has nevertheless been repeated many times by GOP politicians. (Democrats want to reverse health policy changes that the GOP’s tax law enacted, including limits to federal funding for health care for “lawfully present” immigrants.)
Neither side appears ready to budge, which means that as of right now, people who buy health care on the Affordable Care Act (ACA) marketplace are about to be in for some sticker shock. Monthly out-of-pocketcosts are set to jump as much as 75% for 2026 because of the disappearance of federal subsidies and higher rates from insurers.
“Most enrollees are going to be facing a double whammy of both higher insurance bills and losing the subsidies that lower much of the cost,” says Matt McGough, a policy analyst at KFF for the Program on the ACA and the Peterson-KFF Health System Tracker.
KFF recently calculated that the median rate increase proposed by insurers is 18%, more than double last year’s 7% median proposed increase. But the actual blow to patients is going to be much higher. That’s because enhancements to premium tax credits are set to expire at the end of 2025.
Around 93% of marketplace enrollees—19.3 million people—received the enhanced premium tax credits, according to the Center on Budget and Policy Priorities, saving them $700 yearly on average. For some people, the tax credits meant that they wouldn’t have to pay an insurance premium if they chose certain plans. For others, it meant getting hundreds of dollars off a health plan they otherwise wouldn’t have been able to afford.
Premium tax credits helped people afford plans on the Affordable Care Act marketplaces between 2014 and 2021. Then, in 2021, enhancements to those premium tax credits went into effect with the American Rescue Plan. Before 2021, premium tax credits were only available to people making between 100-400% of the federal poverty limit—so between $25,8200 and $103,280 for a family of three in 2025. The enhanced tax credits were expanded to households with incomes over 400% of the federal poverty limit, and were also made more generous for everyone. That wide range meant they subsidized coverage for people who otherwise would not have gotten any break on their premiums.
The enhancements to the premium tax credits, which are set to expire at the end of 2025, significantly boosted enrollment in Affordable Care Act marketplace plans. More than 20 million people enrolled in marketplace coverage in 2024, according to the Center on Budget and Policy Priorities, up from 11.2 million in February 2021, before the enhancements to the tax credits.
With costs being lowered by half, individuals and families decided, ‘OK, maybe this is financially worthwhile,’” says McGough. “Whereas previously, they thought that they didn’t utilize that much health care, so it wasn’t worth it to purchase health care on the marketplaces.”
Why insurers want to increase rates
Every year, health insurers submit filings to state regulators that detail how much they need to change rates for their ACA-regulated health plans. KFF analyzed 312 insurers across 50 states and the District of Columbia; they found that insurers are requesting the largest rate changes since 2018.
They are requesting the median 18% increase for a few reasons, including rising health care costs, tariffs, and the expiration of the premium tax credit enhancements, KFF found. Health care costs have been rising for years, but insurers say that the cost of medical care is up about 8% from last year. They say that tariffs may put upward pressure on the costs of pharmaceuticals and that growing demand for GLP-1 drugs such as Ozempic and Wegovy is driving up their expenses.
Worker shortages are also driving health care costs up, according to the KFF analysis. It also found that consolidation among health care providers was leading to higher prices because those providers had more market power.
Everyone’s bottom line could be affected
When they went into effect, the enhanced premium tax credits pushed some people into the marketplace who might otherwise have been uncertain about whether to get health insurance. The tax credits were graduated so that people with the lowest incomes got the most help, but they also reached people with slightly higher incomes.
Many people don’t know that those enhancements to the premium tax credits are going away, says Jennifer Sullivan, director of health coverage access for the Center on Budget and Policy Priorities (CBPP). Her organization has been talking to people across the country about how they may be affected if Congress does not extend the enhancements, and has found that even increases of $100 or $200 a month may be enough to force some people out of the marketplace.
“It’s a huge increase in anyone’s budget, particularly at a time when groceries are up and the cost of housing is up and so is everything else,” Sullivan says.
There are other reasons the ACA marketplace may see fewer enrollees, she says. A handful of policies passed by Congress require more verification to enroll in ACA plans and cut immigrant eligibility, for example.
Fewer enrollees are bad news for everyone else. The people who are likely to drop coverage are those who don’t need it for lifesaving treatment or medicine. That means the pool of people who are still covered by ACA plans will be sicker and more expensive to care for.
“The people who are left are statistically more likely to be people with higher health care needs,” says Sullivan, with CBPP. “Those are the folks that are going to jump through extra hoops, whether it’s more paperwork or higher premiums or higher out-of-pocket costs, because they absolutely know they need the coverage.”
There are other society-wide effects to people dropping their health insurance coverage. Many uninsured people end up in emergency rooms for care because that’s their only option, and sometimes, they can’t pay. That increases the cost of health care for everyone else, says Sullivan.
Amy Bielawski, 60, is one of the people who is going to look at her options when rates for marketplace plans are listed in October and decide whether or not to enroll. Bielawski, an entrepreneur and entertainer who performs belly dancing at parties, has spent much of her life without health care.
She finally signed up for an ACA plan in 2019, and was able to go to a doctor and diagnose her hypothyroidism and uterine fibroids. Last year, because of the enhanced premium tax credits, she paid $0 a month in premiums—which will almost certainly go up.
“I’m afraid, I’m very afraid,” says Bielawski, who lives in Georgia. “I can’t wrap my head around it because there are so many things that can go wrong with my health.”
Where politicians stand now
Addressing this uncertainty is one key reason the Affordable Care Act passed in the first place in 2010. It has dramatically improved health coverage for Americans; nearly 50 million people, or one in seven U.S. residents, have been covered by health insurance plans through ACA marketplaces since they first launched in late 2013.
But it has also faced numerous challenges, and Republicans have long said that weakening or revamping the law is a high priority.
It’s unclear if the hassle of a government shutdown will make them change their tune. In September, Senate Majority Leader John Thune, a Republican from South Dakota, said he was open to addressing the expiration of the subsidies, but that he did not want to tie any of those policy changes to government funding measures. Sen. Mike Rounds, also a Republican of South Dakota, has suggested a one-year extension to the subsidies, after which the tax credits return to pre-pandemic levels.
Many Republicans appear determined to end the subsidies eventually, and their insistence on scaling back spending on health care policy seems to be having an impact.
Sullivan, with the CBPP, says that the changes to the Affordable Care Act and looming cuts to Medicaid have the potential to dramatically reduce the number of people able to afford regular medical care in the country. These cuts come at a time when key indicators like infant mortality rates and life expectancy rates are worsening.
“We are seeing a real weakening of that safety net that we spent the last 10-15 years fortifying,” she says.
After a long career as a nurse, Lisa Bower, now 61, retired, started working as a part-time nanny, and, in 2021, realized she needed health insurance. The Illinois resident took to the Internet to sign up for a plan on the Affordable Care Act (ACA) marketplace.
But something went wrong and she somehow ended up on another website that looked a lot like a health insurance marketplace. She entered her phone number and soon started getting calls and texts from people who wanted to help her get health insurance.
Within a few minutes, she was registered for a plan that she thought was ACA-compliant. But Bower had instead signed up for what’s called a fixed indemnity plan, which is not actually health insurance and which just pays a small amount for covered services. She didn’t realize that she didn’t have proper health insurance until the fall of 2025, when her son was looking for a tax form that proved she had marketplace insurance and, unable to find it, started digging into her health care paperwork.
Over three years, he found, she’d paid about $16,000 to the fixed indemnity company while receiving very little benefit. During this time, she’d paid out of pocket for costs like doctor’s appointments and medications. Had she gotten an ACA-compliant plan, she probably wouldn’t have had to pay much in premiums at all, her son says, because her low income would have qualified her for subsidies.
“I did think at the time that it was less painful to sign up than I thought it would be,” says Bower. “I just chose what I thought was a cheap plan and didn’t think much about it.”
Bower’s son, Jack, says that Illinois’s real health care marketplace found evidence of Lisa starting to sign up in 2021, but says that she did not complete the application. Instead, he guesses, she got lured away by Google ads and ended up somewhere else.
“I think she holds a third of the blame, and another third of the blame goes to this company that knowingly does this marketing to get people to pay for things they don’t actually want,” Jack says. “But the other third of the blame goes to our health care system, which is so complicated that companies just thrive in the confusion and an astute person can’t make heads or tails of it.”
The Bowers’ experience is not particularly unusual. Confusion about navigating insurance writ large and the Affordable Care Act marketplace in particular has led many people to end up with plans that they think are health insurance which in fact are not health insurance. They mistakenly click away from healthcare.gov, the website where people are supposed to sign up for ACA-compliant plans, and end up on a site with a misleading name that may provide them with an ACA-compliant plan but also might not.
Experts are predicting that this will happen to a larger degree when ACA open enrollment begins in most states on November 1. Because Congress did not extend enhanced premium tax credits, prices for ACA plans are going up an average of 75%. This may spur more people to search for less expensive plans and end up with something that is not health insurance, whether they know it or not.
“There’s no question that more people will end up with these kinds of plans if the premium tax credits are not extended,” says Claire Heyison, senior policy analyst for health insurance and marketplace policy at the Center on Budget and Policy Priorities, a research and policy institute.
Under the Affordable Care Act, health insurance must cover 10 essential benefits, including outpatient services, emergency services, maternity and newborn care, behavioral health treatment, prescription drugs, and pediatric services. But if people stray from the ACA marketplace, they can end up with plans that don’t cover some—or any—of these essential health benefits. People may end up with short-term plans that don’t last for a full year, or with the type of fixed indemnity plan that Bower got. Others may end up in health care sharing ministries, in which people pitch in for other peoples’ medical costs, but which sometimes do not cover preexisting conditions.
These non-insurance products “have increasingly been marketed in ways that make them look similar to health insurance,” Heyison says. To stir further confusion, some even deploy common insurance terms like PPO (preferred provider organization) or co-pay in their terms and conditions. But people will pay a price for using them, Heyison says, because they can charge higher premiums than ACA-compliant plans, deny coverage based on pre-existing conditions, impose annual or lifetime limits on coverage, and exclude benefits like prescription drug coverage or maternity care.
Often, the websites where people end up buying non-ACA compliant insurance have the names and logos of insurers on them. Sometimes, they are lead-generation sites—like the one Lisa Bower mistakenly visited—that ask for a person’s name and phone number and then share that information with brokers who get a commission for signing up people for plans, whether they are health insurance or not.
“This can definitely happen if someone starts Googling and clicks on the first thing they see,” says Louise Norris, health policy analyst at healthinsurance.org, an independent site providing information about insurance plans. “People might not realize that what they’re seeing isn’t real health insurance.”
These mistakes are enabled by a legal gray area in which websites can imply that they can help people sign up for health insurance and then actually sign them up for something else. Brokers, who often work for particular health insurance companies, can often sign people up for both ACA-compliant plans and non-ACA compliant plans. But they typically get more money signing up someone for a non-ACA compliant plan than an ACA-compliant plan, says Heyison.
Non-ACA compliant plans can spend more on administration costs like brokers and marketing because they aren’t regulated in the same way as ACA-compliant plans and have more cash to spare.
Health insurance is complicated, and brokers exist to help walk people through the process of signing up for health insurance. But they sometimes don’t have consumers’ best interest at heart, says Emma Freer, senior policy analyst for the American Economic Liberties Project. “It’s just very predatory because people clearly want information and guidance,” she says, “but many middlemen are incentivized to operate with their own financial interest in mind, not the consumer’s.”
There has been some legal action against companies who have represented what they’re selling as health insurance, even though it’s not. In May 2025, the U.S. Attorney’s Office for the Eastern District of Pennsylvania charged four businessmen and two companies with conspiracy and wire fraud offenses, alleging they had executed a national telemarketing fraud scheme in which they collected tens of millions of dollars by “systematically deceiving and misleading consumers seeking health insurance through bait-and-switch sales tactics.” And in August 2025, two companies agreed to pay a total of $145 million to settle Federal Trade Commission charges that they deceived consumers into purchasing health care plans that did not provide the comprehensive coverage that was promised.
But because many of these companies are actually offering products that are legal—they just aren’t comprehensive health insurance—it can usually be difficult for people to recover any money, or to even get out of the plans. People who discover they signed up for the wrong plan during their state’s open enrollment period should still be able to cancel the plan and sign up for real health insurance, says Heyison, of CBPP. But those who don’t find out for months—or years—that they signed up for non-ACA compliant plans may have a harder time.
“It is definitely a situation where people need to pay close attention now, because in most cases you don’t get a do-over,” says Norris, of healthinsurance.org.
Brandon A., a 27-year-old Maryland resident, didn’t have a lot of experience signing up for health insurance because he’d been in the military and gotten health insurance there. When he went to research plans on the ACA marketplace in mid-October, he searched online for Maryland Health Connection, the state’s marketplace, but ended up on marylandhealthcoverage.org instead.
After entering his zip code and some personal information like his social security number, he got a quote for a plan. He also started getting bombarded with texts and phone calls from people who wanted to sign him up for health insurance. He chose a plan that was just a $300 deposit and $100 a month afterwards. After a few days, and checking with some friends, something seemed off to him, so he called the company back to cancel. They argued with him, telling him it was “the best healthcare nationwide,” he says, but eventually allowed him to cancel the plan.
In retrospect, Brandon, who didn’t want his last name used because he’s embarrassed about his error, saw that in the website’s fine print at the very bottom, in very small text, it says it is not a federal or state health insurance marketplace. “It seems too easy for these sites to pose as real marketplaces,” he says.
Marylandhealthcoverage.org is operated by NextGen Leads, a lead-generation site that collects the information of people looking for health insurance and then charges companies for that information. It has more than 100 complaints on the Better Business Bureau of San Diego, where the company’s website says it is based. Many of the people filing these complaints say that they thought they were signing up for marketplace health insurance in states like Maryland and Georgia, entered their personal information on a site owned by NextGen Leads—often with a domain name ending in .org— and then got spammed with hundreds of calls and texts from people trying to sell them health insurance products. “Their fraudulent website to mimic a health marketplace for [redacted] resulted in selling my information where now I received so many calls from spammers that I literally can not use my phone due to the insane amount of calls,” one person wrote, in January 2025. The company did not reply to TIME’s request for comment.
Experts recommend that people who are stuck in plans that they didn’t mean to buy contact their state insurance commissioner to report the problem. They should also contact a health care navigator or assister—federally funded individuals who exist solely to provide unbiased information—to see if they might qualify to sign up for a comprehensive health insurance plan through a special enrollment period because of a qualifying life event.
Navigators and assisters are also helpful for those seeking new insurance, rather than engaging with brokers. Healthcare.gov is the best place for people to sign up for health insurance who want to do it on their own. Though about 20 states run their own marketplaces that use a different URL, healthcare.gov will direct them to the state marketplaces. It can also direct them to local assisters and navigators.
Signing up for a plan on the true ACA marketplace should not lead consumers to get bombarded with texts or calls—if this happens to you, it probably means you ended up on a lead-generation site instead of on the real marketplace.
Heyison, of CBPP, recommends that consumers never rely on verbal promises that someone selling health insurance gives over the phone, they should instead ask for the plan documents. They should avoid companies offering an upfront gift for signing up, and ones that say that a certain price will only last a few days. Consumers should also spend a few days researching a plan, rather than buying the first thing they see, Heyison says. They should be looking for a plan on healthcare.gov and one that is ACA-compliant.
Some states are attempting to further regulate brokers and non-ACA compliant plans, Heyison says. In California, for instance, agents and brokers are required to assess people for Medicaid and the ACA’s premium tax credit because they enroll them in health care sharing ministries, which could save them money by signing them up for government health insurance instead of a product that is not health insurance. And some states, including California, Illinois, and Massachusetts, prohibit the underwriting of short-term health insurance coverage, making it nearly impossible to sell non-ACA compliant plans in those states.
But most other states haven’t taken action, leaving people like Lisa Bower out of luck. Her son Jack tried to call the company that issued her indemnity plan and get a refund, but he knows he likely has no legal recourse. She should have read the paperwork more closely, they both admit. This year, they’re ready for open enrollment—and are determined not to look anywhere but healthcare.gov, the official Affordable Care Act marketplace.
We learned yesterday that the average cost of a family health insurance policy through an employer reached nearly $27,000 this year, 6% higher than what it cost in 2024. As if that weren’t alarming enough, researchers are predicting that the total likely will soar toward $30,000 next year because of rising medical costs and the unrelenting pressure insurers are under from Wall Street to increase their profits. Small businesses will be hit the hardest.
Despite repeated assurances from insurers that we can count on them to hold down the cost of health care – and consequently the premiums they charge – there are now many years of evidence – from researchers like KFF, which tracks annual changes in employer-sponsored coverage – that they have not and cannot deliver on their promises.
Nevertheless, Big Insurance is doing just fine financially as they force America’s employers and workers to shell out increasingly absurd amounts of money for policies that actually cover less than they did ten years ago. A health insurance policy today is generally less valuable than it was a decade ago because families have to spend more and more money out of their own pockets every year before their coverage kicks in. In addition, they are far more likely to be notified that their insurers will not cover the care their doctors say they need.
When you look at KFF’s reports over time, you’ll see that the cost of a family policy has increased 60% since 2014 when it cost an average of $16,834. That is a rate of increase much higher than general inflation and also higher than medical inflation.
Not only has the total cost of an employer-sponsored plan skyrocketed, so has the share of premiums workers must pay. This year, employers deducted an average of $6,850 from their workers’ paychecks for family coverage, up from $4,823 in 2014, a 42% increase.
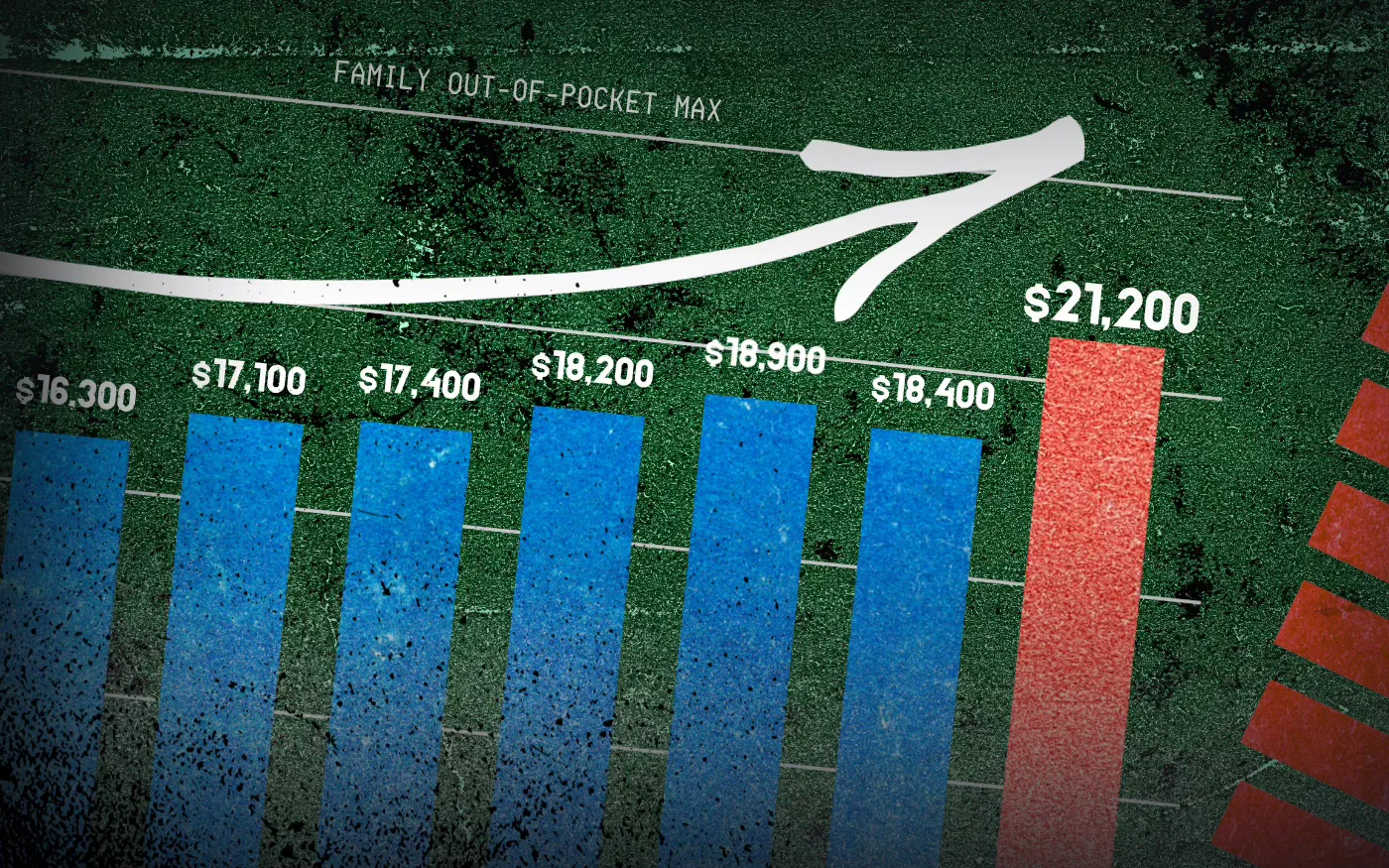
And as premiums have risen, so has the amount of money workers and their dependents are required to spend out of their pockets in deductibles, copayments and coinsurance. The Affordable Care Act, to its credit, instituted a cap on out-of-pocket expenses in 2014, but that cap has been increasing annually along with premiums. (The U.S. Department of Health & Human Services sets the out-of-pocket max every year, pegging it to the average increase in premiums.)
In 2014 the out-of-pocket cap for a family policy was $12,700. Next year, it will rise to $21,200 – a 67% increase. And keep in mind that the cap only applies to in-network care. If you go out of your insurer’s network or take a medication not covered under your policy, you can be on the hook for hundreds or thousands more. While most employer-sponsored plans have caps that are considerably lower, many individuals and families reach the legal max every year.
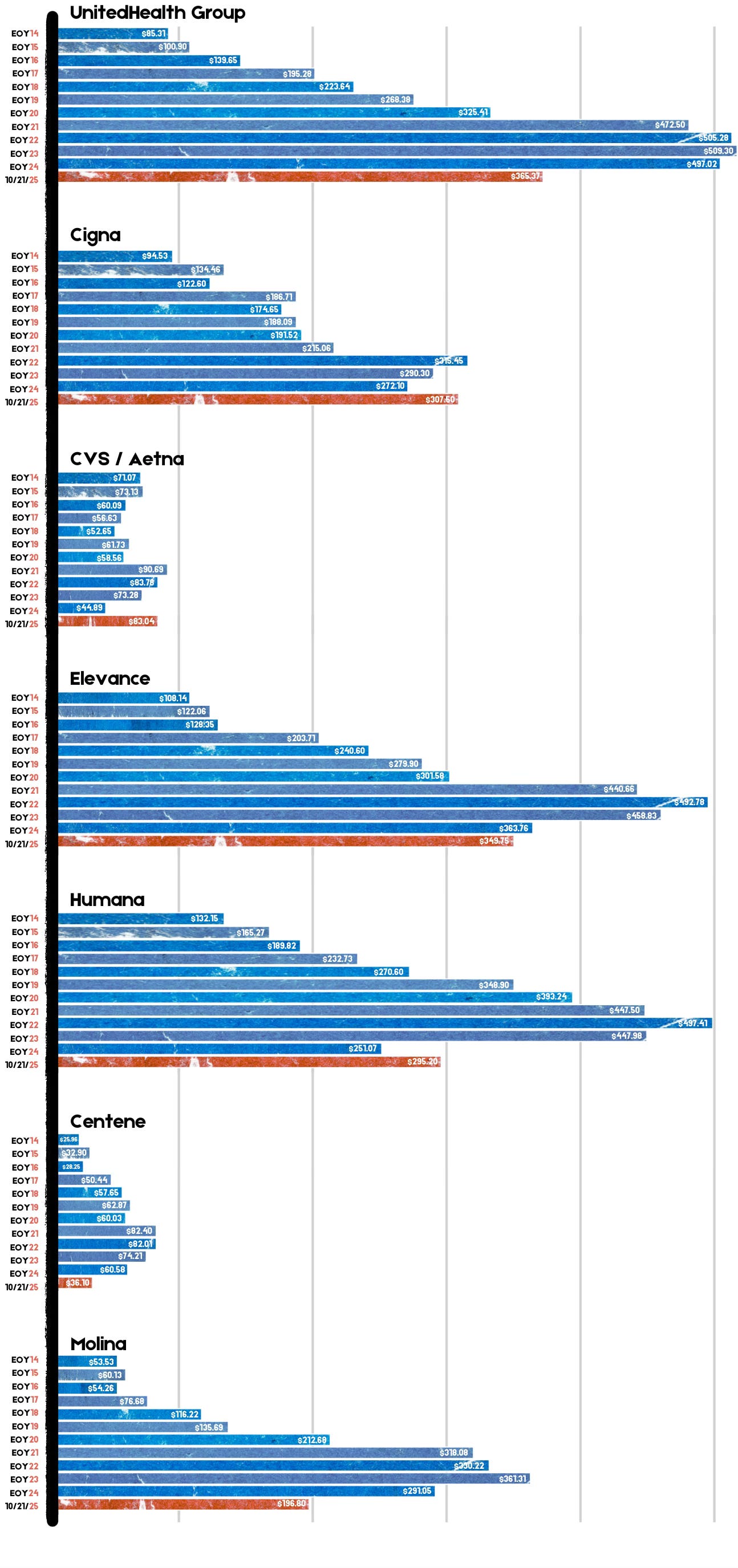
Meanwhile, the seven biggest for-profit health insurers have made hundreds of billions in profits since 2014 as they have jacked up premiums and out-of-pocket requirements and erected numerous barriers, including the aggressive use of prior authorization, that make it more difficult for Americans to get the care and medications they need. Collectively, those seven companies made $71.3 billion in profits last year alone. That was up slightly from $70.7 billion in 2023. Insurers said their 2024 profits were somewhat depressed because more of their health plan enrollees went to the doctor and picked up their prescriptions last year. Investors were furious that insurers couldn’t keep that from happening, as you’ll see in the charts below. Many of them sold some or all of their shares, sending insurers’ stock prices down. But overall, the stock prices of the big insurance conglomerates have increased steadily over the years as we and our employers have had to spend more for policies that cover less.
For example, UnitedHealth Group, the biggest of the seven, saw its stock price increase 483% between 2014 and 2024 – from $85.31 a share on Dec. 31, 2014, to $497.02 on Dec. 31, 2024. Most of the other companies saw similar growth in their shares over that time period.
By contrast, the Dow Jones Industrial Average increased 139% (from $17,823.07 to $42,544.22), and the S&P 500 increased 186% (from $2,058.90 to $5,881.63) during the same period.
Back to those premiums and out-of-pocket requirements. While the KFF numbers pertain to employer-sponsored coverage, people who have to buy health insurance on their own – mostly through the ACA (Obamacare) marketplace – have experienced similar increases. Most Americans who buy their insurance there could not possibly afford it if not for subsidies provided by the federal government on a sliding scale, which is based on income. The most generous subsidies have been available since 2014 to people with income up to 150% of the federal poverty level (FPL). During the pandemic, Congress expanded – or “enhanced” – the subsidies to make them available to people with incomes up to 400% of FPL. Those enhanced subsidies are scheduled to expire at the end of this year. Whether to let them expire or extend them is at the center of the ongoing government shutdown. Most Democrats are insisting they be extended while most Republicans want them to end. It’s important to note that the federal money goes to insurance companies, not to people enrolled in their health plans.
If the enhanced subsidies do end, millions of Americans who get their health insurance through the ACA marketplace will drop their coverage because the premiums will be unaffordable for them and their families. In Pennsylvania where I live, premiums for policies bought on the state’s insurance exchange are expected to increase 102% next year because of the anticipated end of the subsidies and premium inflation.
More than 24 million Americans now get their coverage through the ACA marketplace, primarily because their employers cannot offer health insurance as an employee benefit anymore. Over the past several years, a growing number of small businesses have stopped offering subsidized coverage to their workers because of the expense. Just slightly more than half of U.S. businesses are still in the game. The rest simply can’t afford the premiums. Small businesses can expect an average increase of 11% next year with some of them facing increases of 32%.
It is becoming more clear every passing year that the U.S. has one of the most insidious ways of rationing care. It is rationed based on a person’s ability to pay far more than on a person’s need for care. And among those most disadvantaged by the current system are hard-working low- and middle-income Americans with chronic conditions and those who suddenly get sick or injured.
While the Affordable Care Act prohibited insurers from charging people with pre-existing conditions more than healthier people, insurers have figured out a back door way to discriminate against them: by making them pay hundreds or thousands of dollars out of their own pockets every year – in addition to their premiums – and also by refusing to cover treatments and medications their doctors say they need.
Now you know why Big Insurance is doing so well while the rest of us are getting
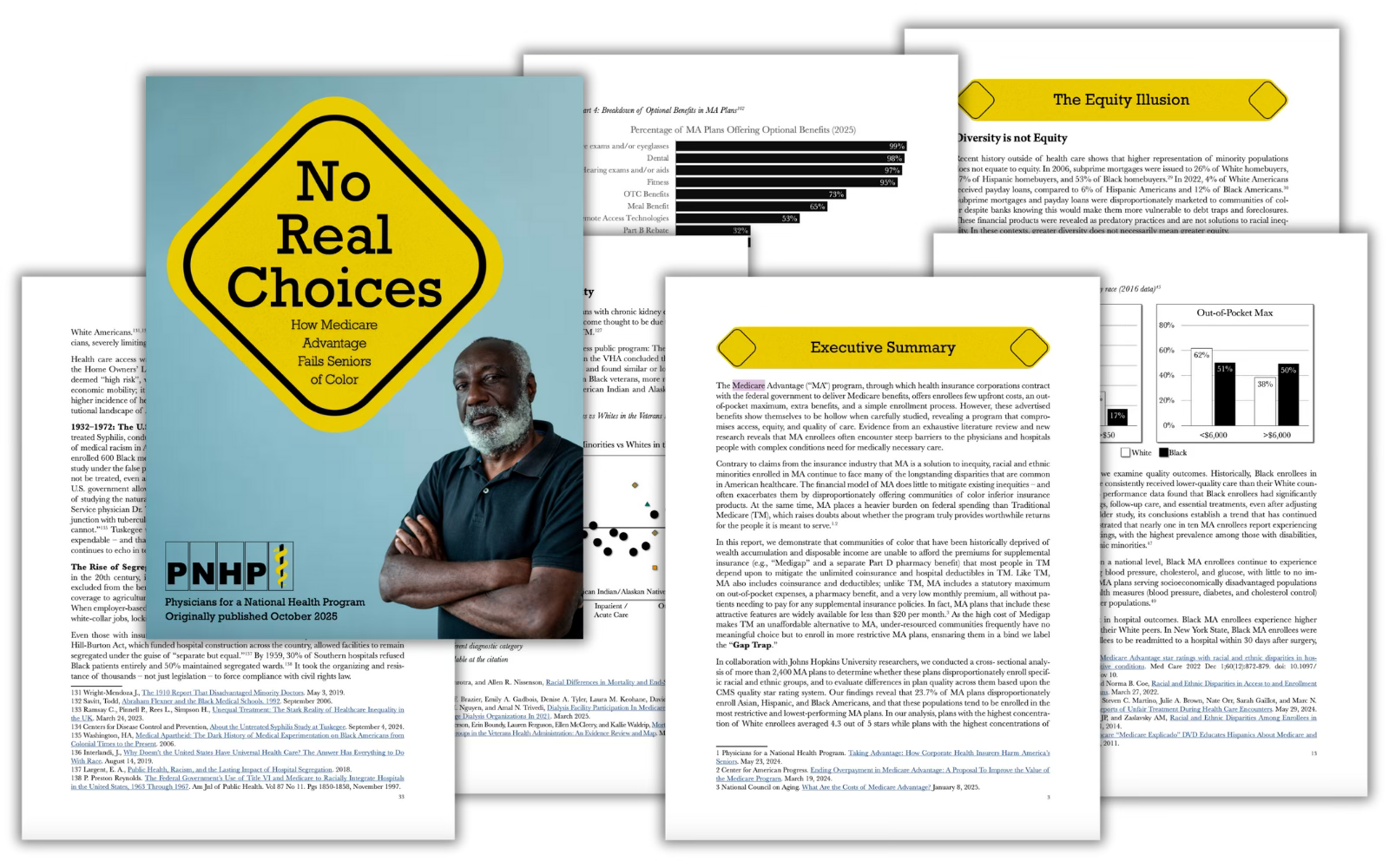
Physicians for a National Health Program (PNHP) — in collaboration with Johns Hopkins University researchers — just released a report titled “No Real Choices: How Medicare Advantage Fails Seniors of Color”. It confirms that the handover of public programs like Medicare Advantage (MA) to Big Insurance doesn’t close racial, ethnic and economic health gaps — it deepens them.
Read Physician for a National Health Program’s report, No Real Choices: How Medicare Advantage Fails Seniors of Color, here.
PNHP’s researchers found that communities of color are being steered into MA plans not because they’re better — but because they’re cheaper upfront. This dynamic, dubbed the “Gap Trap,” means that affordability is driving people into coverage that often denies care, delays treatment and locks them into narrow networks.
“Medicare Advantage squanders billions, harms seniors and exacerbates racial inequities,” Dr. Diljeet K. Singh, gynecologic oncologist and president of Physicians for a National Health Program, said. “Americans need universal health Care which removes profit-motivated conflicts of interest, abolishes co-pays and deductibles, ends prior authorization burdens and guarantees protection from medical bankruptcy.”
HEALTH CARE un-covered is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.
Medicare Advantage is the health care equivalent of the subprime mortgage crisis — except the fine print here is costing Americans’ lives and depleting the Medicare Trust Fund.
The equity illusion
When Big Insurance boasts about “diverse” enrollment in MA, this report reminds us: “Diversity” is often just a buzzword used for PR reasons and has nothing to do with seniors receiving the care they deserve — especially when it is used as cover for a business model that profits from inequity.
Black, Hispanic and Asian/Asian-American beneficiaries are disproportionately concentrated in MA plans that score lowest on quality ratings, while white beneficiaries are more likely to live in counties served by higher-quality plans.
One study found that MA prior authorization requests were denied 23% of the time for Black seniors vs. 15% for their white counterparts.
Despite industry claims to the contrary, racial and ethnic health disparities in the United States are not being reduced by Medicare Advantage.
Studies show that Black enrollees are more likely than white enrollees to choose a 5-star MA plan when offered one. They’re just not offered them as often.
Racial minority enrollees in MA suffer from worse clinical outcomes and face barriers accessing best quality care because of restrictive networks and misaligned financial incentives. Black MA enrollees experience higher rates of hospital readmission compared to their white peers.
The MA paperwork burden isdriving doctors out of practice, worsening access for everyone — but especially in already underserved communities.
MA’s restrictive payment practices aren’t just harming patients — they’re pushing hospitals, especially those serving rural and minority communities, toward the edge of closure. Under-payment or delay of claims by MA insurers causes cascading financial harm in these vulnerable systems.
The big picture
As a reminder, even with the racial and ethnic issues aside, Medicare Advantage already severely restricts seniors’ access to providers, imposes unnecessary prior authorization hurdles that often result in deadly delays and denials — and cost taxpayers at least$84 billionmoreeach year than original Medicare. Meanwhile, original, traditional Medicare does not even have networks; almost all doctors participate and few treatments are subject to prior authorization.
PNHP’s report shows that despite insurers’ endless “health equity” pledges and glossy diversity campaigns, MA remains a rigged game that leaves millions of seniors — disproportionately people of color — with worse access, inferior care and fewer real choices.
Big Insurance’s MA plans are shaped by the same market incentives that have long rewarded exclusion and sorting risk, and – if history tells us anything – sorting has always leaned on racial dimensions. As the report sums it up:
“Regardless of the reasons, any system that traps and harms people — particularly in ways that map onto centuries of racial injustice — cannot be a solution to health inequity.”
Average annual premiums for single health coverage
A grouped column chart comparing average annual premiums for single coverage from 2018 to 2025 for ACA benchmark plans and employer-sponsored plans. Both plan types have increased in cost since 2018. In 2024, ACA benchmark plans were $5.7k annually while employer-sponsored plans were almost $9k on average. No data is available for employer-sponsored plans in 2025.
Something big isbeing missed in the congressional showdown over enhanced Affordable Care Act subsidies: Health insurance premiums are eye-wateringly expensive for the average person without some kind of subsidy.
Why it matters:
Health care in the U.S. is expensive, we know, we’ve all heard it a million times. But most of us don’t really feel its full expense, which removes a lot of the urgency to truly address health care costs.
Whether it’s through government tax credits or employer premium assistance, most Americans with private health insurance don’t pay the entirety of their premium.
But we’re all paying the freight one way or another, either through taxes or paycheck deductions.
State of play:
The past few weeks have been full of dire warnings from Democrats and their allies about what will happen if the enhanced ACA subsidies from the pandemic era are allowed to expire at year’s end.
The gist is that millions of Americans will have sticker shock when they’re exposed to more or all of the premium cost, and many will ultimately opt out of buying coverage. That’s all probably true.
Of course, allowing the enhanced subsidies to expire would just make the law’s structure revert to its original state.
And that’s why some savvy Republican-aligned commenters are asking if that means the ACA is broken, or if the original version was unworkable.
Reality check:
Premiums have gone up — a lot, in some cases. But that’s not unique to the ACA marketplace, and premiums are even pricier in the employer market.
By the numbers:
This year, the average premium for a benchmark ACA plan is $497 a month, or nearly $6,000 a year, according to KFF.
The average employer-employee premium for single coverage was $8,951 last year, also according to KFF.
The average premium for family coverage was a whopping $25,572.
Let’s do some math.
Without any form of subsidization, a single person making $60,000 would spend 10% of pretax income on an ACA plan, and 15% on an employer plan.
Now let’s say that $60,000 income is supporting a family of four. The average premium without subsidies would cost that family 43% of its pretax income.
The median U.S. family income, according to the Census Bureau, was $83,730 in 2024. Health insurance premiums would be 31% of pretax income.
Between the lines:
The definition of “affordable” is obviously very subjective, but it seems safe to say that some of these numbers — especially for families — aren’t meeting it.
What we’re watching:
Open enrollment is coming, and people with ACA coverage aren’t the only ones facing premium increases.
Health benefit costs are expected to increase 6.5% per employee in 2026, according to Mercer. Many employers are planning to limit premium increases by raising out-of-pocket costs for employees.
On average, ACA marketplace plans are raising premiums about 20% in 2026, according to KFF.
How much of that increase gets passed on to enrollees will depend on whether the enhanced subsidies are extended, but the premium increases are partially due to insurers having accounted for the subsidy expiration.
The bottom line:
Policymakers have two broad options: They can keep fighting over who pays for what, or they can do bigger, systemwide reform.
If you’re waiting for the latter, don’t hold your breath!
The U.S. health industry revolves around a flawed presumption: individuals and families are dependent on the health system to make health decisions on their behalf. It’s as basic as baseball and apple pie in our collective world view.
It’s understandable. Consumers think the system is complex. They believe the science on which diagnostics and therapeutics are based requires specialized training to grasp. They think health insurance is a hedge against unforeseen bills that can wipe them out. And they think everything in healthcare is inexplicably expensive.
This view justifies the majority of capital investments, policy changes and competitive strategies by organizations geared to protecting traditional roles and profits. It justifies guardianship of scope of practice limits controlled by medical societies because patients trust doctors more than others. It justifies pushback by hospitals, insurers and drug companies against pro-price transparency regulations arguing out-of-pocket costs matter more. It justifies mainstream media inattention to the how the health system operates preferring sensationalism (medical errors, price sticker shock, fraud) over more complicated issues. And it justifies large and growing disparities in healthcare workforce compensation ranging from hourly workers who can’t afford their own healthcare to clinicians and executives who enjoy high six figure base compensation and rich benefits awarded by board compensation committees.
It’s a flawed presumption. It’s the unintended consequence of a system designed around sick care for the elderly that working age populations are obliged to fund. Healthcare organizations should pivot because this view is a relic of healthcare’s past. Consider:
Most consumers think the health system is fundamentally flawed because it prioritizes its business interests above their concerns and problems.
Most think technologies—monitoring devices, AI, et al– will enable them to own their medical records, self-diagnose and monitor their health independently.
And most –especially young and middle age consumers—think their healthcare spending should be predictable and prices transparent.
In response, most organizations in healthcare take cautious approaches i.e. “affordability” is opined as a concern but defined explicitly by few if any. “Value” is promised but left to vague, self-serving context and conditions. “Quality” is about affiliations, capabilities and processes for which compliance can be measured but results (outcomes, diagnostic accuracy, efficacy, savings, coverage adequacy, et al) — hardly accessible. And so on.
For starters, the industry must address its prices, costs and affordability in the broader context of household discretionary spending. Healthcare’s insiders are prone to mistaken notions that the household healthcare spend is somehow insulated from outside forces: that’s wrong. Household healthcare expenditures constitute 8.3% of the monthly consumer price index (CPI); housing is 35.4%, food is 13.6% and energy is 6.4%. In the last 12 months, the overall CPI increased 2.9%, healthcare services increased 4.2%, housing increased 3.6%, food increased 3.2% and energy costs increased only 0.2%. In that same period, private industry wages increased 1.0% and government wages increased 1.2%. Household financial pressures are real and pervasive. Thus, healthcare services costs are complicit in mounting household financial anxiety.
The pending loss of marketplace subsidies and escalating insurance premiums means households will be expected to spend more for healthcare. Housing market instability that hits younger and lower-middle income households hardest poses an even larger threat to household financial security and looms large in coming months. Utilization of healthcare products and services in households during economic downturns shrinks some, but discretionary spending for health services—visits, procedures, tests, premiums, OTC et al—shrinks substantially as those bills take a back seat to groceries, fuel, car payments, student loan debt, rent/mortgage payments and utilities in most households.
Healthcare organizations must rethink their orientations to patients, enrollees and users. All must embrace consumer-facing technologies that empower individuals and households to shop for healthcare products and services deliberately. In this regard, some insurers and employers seem more inclined than providers and suppliers, but solutions are not widely available. And incentives to stimulate households to choose “high value” options are illusory. Data show carrots to make prudent choices work some, but sticks seem to stimulate shopping for most preference-sensitive products and services.
The point is this: the U.S. economy is slowing. Inflation is a concern and prices for household goods and necessary services are going up. The U.S. health industry can ill-afford to take a business-as-usual approach to how our prices are set and communicated, consumer debt collection (aka “rev cycle”) is managed and how capital and programmatic priorities are evaluated.
Net Promoter Scores, Top 100 Recognition and Star Ratings matter: how organizations address household financial pressures impacts these directly and quickly. And, as never before, consumer sentiment toward healthcare’s responsiveness to their financial pressures is at an all-time low. It’s the imperative that can’t be neglected.
Recent analysis of spending data from five states with health care cost growth targets—Connecticut, Delaware, Massachusetts, Oregon, and Rhode Island—revealed an unexpected trend in 2023: Spending grew sharply in service categories that have historically increased more slowly. The most notable increase was in non-claims payments—payments made through financial arrangements between providers and health insurers that are not tied to individual claims. These payments rose by an average of 40.4 percent across the five states, driven largely by increases in Medicare Advantage non-claims spending.
Increases in non-claims payments are often seen as a positive sign. They suggest a shift away from fee-for-service payments toward alternative payment methods (APMs)—value-based payment models that incentivize care coordination, efficiency, and a focus on outcomes. However, it’s unclear what is included in these non-claims payments. A closer examination of this issue revealed a less visible but important concern: the role of insurer-provider vertical integration in potentially weakening the effectiveness of Medical Loss Ratio (MLR) requirements for insurers.
MLR Requirements
Medical Loss Ratio is a measure of the percentage of premium dollars that a health insurer spends on medical care and quality improvement activities—as opposed to administration, marketing, or profit. Since 2011, the Affordable Care Act has required insurers to maintain an MLR of at least 80 percent in the individual and small group markets, and 85 percent in the large group market. That is, for every dollar spent by an insurer, 80 cents or 85 cents—depending on the market—must go toward actual care and improvement. Insurers that don’t meet these required thresholds must pay a rebate to consumers for the premium dollars that were not spent on health care, less taxes, fees, and adjustments. In 2014, the Centers for Medicare and Medicaid Services instituted a requirement for Medicare Advantage and Part D plans; they must maintain an MLR of at least 85 percent or rebate any excess revenues to the federal government.
These MLR requirements aim to ensure that the majority of premium revenue is used to deliver or improve care. However, a significant loophole allows insurers that have “vertically integrated” with providers to inflate reported medical spending. This reduces their rebate liability while increasing held profits. Since the MLR provisions took effect in 2012, an estimated $13 billion in rebates have been issued—highlighting the strong incentive insurers have to minimize these payouts.
The MLR Loophole
A company is vertically integrated when it owns or controls more than one entity in the supply chain. For insurers, this means acquiring physician practices, outpatient clinics, and even entire health systems. As a result of this vertical integration, payments to these affiliated providers count as medical spending when calculating an MLR for the insurer. However, there is no MLR requirement for providers. This creates an incentive for the insurer to direct spending to these affiliated provider entities, which may charge inflated prices, allowing the insurer to increase its reported MLR without delivering more care or improving quality.
Consider a hypothetical scenario: Company X owns Health Insurer A and Clinic Y. There’s another health insurer, B, in the market, but it is not owned by Company X. It costs Clinic Y $300 to deliver a particular service.
When a patient covered by Health Insurer B receives this service at Clinic Y, Insurer B pays the clinic $300 for delivering the service. But when another patient covered instead by Health Insurer A receives the same particular service at Clinic Y, Health insurer A pays the clinic a lot more: $500. The full $500 is counted as medical spending in Health Insurer A’s MLR calculation, even though the additional $200 didn’t buy any more services or any better care. It just represents internal profit for the vertically integrated entity, Company X, that is captured on the provider side of the business, and not true care delivery (see exhibit 1 below).
Exhibit 1: Incentives for vertically integrated insurers to direct spending to these affiliated provider entities
Source: Authors’ analysis.
The structure of APMs exacerbates this problem by making it easier to mask price increases. In fee-for-service systems, a price increase shows up directly. However, in APM payments that are per capitation or per episode, providers receive lump-sum payments for a group of services or a population. There is no service breakdown for these APMs. These lump-sum payments can facilitate investment in population health improvement, but if vertically integrated entities are exploiting the MLR loophole by increasing internal payment rates, the use of APMs make such profit maximization easier to conceal.
This dynamic reveals a limitation of the MLR rules. When the insurer is also the provider, there is less transparency into how health care dollars are actually allocated. The vertically integrated insurer and provider entity can also artificially inflate prices for medical services, worsening the nation’s health care affordability problem.
Potential Impact
Currently, there is no standardized way to assess the extent to which insurers that own or are otherwise affiliated with clinics and health systems are taking advantage of this loophole, or how much the practice contributes to high health care prices. However, with the growing trend toward insurer-provider vertical integration, the potential cost implications are significant.
Insurers That Own Providers Capture A Significant Share Of Commercial And Medicare Advantage Enrollment
In the large-group commercial market, the three largest insurers—Kaiser Permanente, UnitedHealthcare, and Elevance—held a combined 39 percent of the national market share in 2023. In the Medicare Advantage market, the top five plans—UnitedHealthcare, Humana, CVS Health/Aetna, Elevance, and Centene—accounted for 68 percent of total enrollment in 2023.All of these insurers operate within larger parent companies that own or control a range of health care provider entities.
For example, UnitedHealth Group, UnitedHealthcare’s parent company, also owns OptumHealth, which employs or manages more than 90,000 physicians across the country. The recently released Sunlight Report on UnitedHealth Group shows that it grew more than 10 times its size over the past decade, and the company now consists of nearly 3,000 distinct legal entities.
UnitedHealth Group is not the only insurer pursuing this strategy of vertical integration. Elevance Health (formerly Anthem, Inc.) owns Carelon, a health services provider that claims to serve one in three people in the US. CVS Health encompasses retail pharmacy storefronts (CVS Pharmacy), a pharmacy benefits manager (CVS Caremark), a health insurer (Aetna), in-store clinics (MinuteClinic), and provider groups such as Oak Street Health and Signify Health. This high level of consolidation gives these companies significant control over how care is delivered, priced, and reported.
Transactions Between Insurers And Their Affiliated Provider Entities Are Substantial And Growing
A 2022 analysis by the Brookings Institution suggests that in Medicare Advantage plans, internal transactions between affiliated insurers and providers can account for spending that ranges from about 20 percent to as much as 71 percent of the total. Cost growth target states’ reports on 2023 spending growth appear to confirm these trends within the Medicare Advantage market. Upon examination of the drivers behind the sharp increases in non-claims payments, a clear pattern emerged. In Connecticut, UnitedHealthcare launched a program that paid its affiliated provider group, which was then called OptumCare Network, a fixed percentage of Medicare Advantage premiums to cover care and care coordination. Oregon reported that the rise in Medicare Advantage non-claims payments was largely due to UnitedHealthcare shifting a significant share of its claims payments into non-claims spending through Optum.
These trends are not limited to Medicare Advantage, however. UnitedHealth and other major insurers such as Elevance and Aetna operate across multiple markets, raising concerns about similar dynamics in the commercial market. A recent analysis by Seth Glickman, a physician and former insurance executive, shows that in the past five years, UnitedHealth Group’s reported corporate “eliminations”—intercompany revenues reported in its consolidated financial statements that represent all books of business—more than doubled, increasing from $58.5 billion to $136.4 billion. At the same time, the share of Optum’s revenue derived from UnitedHealthcare, as opposed to unaffiliated entities, increased by nearly 50 percent.
Prices Of Health Care Services From Vertically Integrated Insurers And Providers Are Higher Than Prevailing Market Prices
Growing evidence also suggests that insurers are paying more for services provided through their affiliated entities than for those delivered by non-affiliated entities. A STAT News investigation revealed that UnitedHealth Group reimburses its own physician groups considerably more than other providers in the same markets for the same set of services. Similarly, a Wall Street Journal investigation showed how certain insurers and pharmacy benefit managers are generating substantial profits by overcharging for generic drugs within their own networks. The analysis found that for a selection of specialty generic drugs, Cigna and CVS’s prices were at least 24 times higher, on average, than the drug manufacturers’ prices.
Stronger Oversight Is Needed
The potential impact of these trends is so significant that policy makers are beginning to take notice. In 2023, Senators Elizabeth Warren (D-MA) and Mike Braun (R-IN) requested that the Department of Health and Human Services Office of Inspector General evaluate the extent to which vertical integration is increasing costs and allowing insurers to bypass federal MLR requirements. Earlier this year, Representatives Lloyd Doggett (D-TX) and Greg Murphy (R-NC) submitted a bipartisan request to the Government Accountability Office—Congress’s independent, nonpartisan oversight agency—urging an investigation into the same issue in Medicare Advantage. It is unclear whether these investigations have been initiated.
Some states—understanding the role that market consolidation plays in driving up health care prices—have made efforts to strengthen oversight. In 2024, 22 states passed laws related to health system consolidation and competition. However, historically, these efforts have largely focused on promoting competition, preventing monopolies, and limiting dominant providers’ ability to charge prices well above competitive levels. Little attention has been given to the MLR loophole and the ability of vertically integrated insurers to report profits as medical care.
As states pursue policies to slow cost growth, they must apply greater scrutiny of vertical integration arrangements—especially around internal financial transactions between affiliated entities. States should require insurers to report detailed information on transactions between related parties, including non-claims-based APMs to affiliated providers and the pricing methodology used to develop these APMs. This reporting could be integrated into states’ premium rate review processes, allowing regulators to assess whether such transactions reflect actual medical costs. States could then modify or deny rate increases where evidence points to gaming of MLR rules.
Policy makers should also reassess whether, given these market dynamics, current regulatory tools such as the MLR are adequate. Addressing these issues will be essential for maintaining the integrity of cost containment efforts and ensuring that health care dollars are spent on delivering meaningful care.
The Trump 2.0 administration is 8-months into its MAGA agenda. Summer has passed. Schools are open. Congress is in session. Campaign 2026 is underway. The economy is slowing and public sentiment is dropping.
For U.S. healthcare, it’s more bad news than good. The challenges are unprecedented. Most organizations—hospitals, medical groups, drug and device makers, infomediaries and solution providers, insurers, et al—are defaulting to lower risk bets since the long-term for the health system is unclear.
The good news is that the health system in the U.S. is big, fragmented, complex, expensive (5% CAGR spending increases thru 2034) and slow to change. It is highly regulated at local, state and federal levels, labor intense (20 million) and capital-dependent (government funding, private investment)—a trifecta nightmare for operators and goldmine for private investors who time the system for shareholders effectively. And it operates opaquely: business practices are hidden from everyday users and bona-fide measures of its effectiveness not widely applied or accepted.
The bad news is its long-term sustainability in its current form is suspect and its short-term success is dependent on adapting to key tenets in Trump Healthcare 2.0:
Trump Healthcare 2.0 is about reducing federal healthcare spending so federal deficits appear to be going down to voters in the mid-term election (November 3, 2026). Healthcare, which represents 27% of federal spending is an attractive target since a significant majority of all voters (especially MAGA Republicans) are dissatisfied with its performance and think is wasteful and inefficient. It views healthcare as a market where less government, more private innovation achieves more.
The effect of One Big Beautiful Bill Act cuts to Medicaid and marketplace subsidies and imposition of Make America Healthy Again dogma in CMS, CDC, FDA and FCC are popular in the MAGA base while problematic to states, hospitals, physicians and insurers whose business practices and clinical accountability will be more closely scrutinized.
The federal courts—SCOTUS, 13 circuit and 94 district courts– will support Trump Healthcare 2.0 policy changes in their decisions favoring state authority over federal rules, enabling White House executive orders and administrative actions against challenges and departmental directives that encourage competition, price transparency and cost reduction.
The FTC and DOJ will pro-actively pursue actions that reverse/disable collusion, horizontal and vertical consolidation in each sector deemed to raise prices and lower choices for consumers.
In the administration’s posturing for the mid-term election November 3, 2026, it’s assumed the economy and prices will be THE major issues to voters: healthcare affordability, housing costs and food prices will get heightened attention as a result. Thus, every healthcare organization board and leadership team should revisit short and long-term strategies, since traditional lag indicators re: utilization, regulations, structure, roles, responsibilities and funding are decreasingly predictive of the future.
Though every organization is different, there are 6 takeaways that merit particular attention as C suites and Boards re-evaluate strategies and timing:
Monitor the entire economy. The healthcare is 18% of the GDP; 82% of commerce falls outside its domain. Appropriations for healthcare compete with education, defense and public safety and health; household spending for healthcare competes with housing, food and transportation costs. The healthcare dollar is not insulated from competing priorities. If, as expected, the economy slows due to slowdowns in the job market and in housing, and if cuts to marketplace subsidies are enacted, healthcare spending will quickly and significantly drop though utilization will increase.
Follow clinical innovations carefully. Understand bench to bedside obstacles. The FDA will authorize 50-60 novel drugs and biologics and over 100 AI-enabled devices this year. Some will fundamentally alter care management processes; all will change costs and pricing. Those with short-term cost-reduction potential require consideration first. Given increased margin pressures, capital and operating budgets will reflect a more cautious and risk averse posture.
Manage fixed costs (more) aggressively and creatively. Direct costs reduction is not enough. Facilities and administrative functions are fair game and for outsourcing, partnerships and risk sharing with suppliers, vendors, advisors and even competitors.
Don’t underestimate price transparency. Prices matter. Consumers and regulator demand for price transparency from drugmakers, hospitals and insurers are inescapable. Justification and verification will be critical to trust and utilization.
Navigate AI strategically. The pace and effectiveness of Ai-enabled solutions will define winners and losers in each segment. And private capital—investors, partners—will bring those solutions to market.
Don’t discount public opinion. Consumer sentiment about the economy is low and dissatisfaction with the health system is high and increasing. Understanding root causes and initiating process improvement are starting points.
As I head back to DC today, the FY26 federal budget is in suspense as the GOP-controlled Senate and House debate a final version to avoid a shutdown next week. Physicians, public health and state officials will digest last week’s ACIP vaccine advisory recommendations and issue their own directives and insurers will file their plan revisions for 2026. That’s what lawmakers and trade groups will be watching.
But at the kitchen tables in at least 40% of America’s households, unpaid healthcare bills from hospitals, labs, doctor offices and set-aside cash for over-the-counter remedies and prescription drug co-pays are on the agenda. Student loan payments, escalating costs for groceries, housing, rent and child care and an unstable employment market are squeezing families. Budgeting for healthcare is more problematic for them than anything else because price are not accessible and charges are not known until after services are performed.
Trump Healthcare 2.0 is not transformational: it is transactional. It aims to simplify the system and facilitate changes certain to disrupt the status quo. Its locus of control, is Main Street USA. not Pennsylvania Ave, in DC.