President Trump is expected to sign an executive order on Obamacare this week that would allow people to buy cheaper health insurance with fewer regulations, targeting healthcare goals that eluded congressional Republicans all year.
The full details of the executive order have not been released, but enough information has been reported to reveal its overall framework. Trump would direct the Departments of Labor, Treasury and Health and Human Services to make changes to regulations so more people could band together to buy “association health plans” which would allow individuals or small businesses to band together, such as members of a Chamber of Commerce, to buy plans sold across state lines. The order also would allow people to buy short-term health insurance plans for longer than the Obama administration allowed and would encourage the use of health savings accounts.
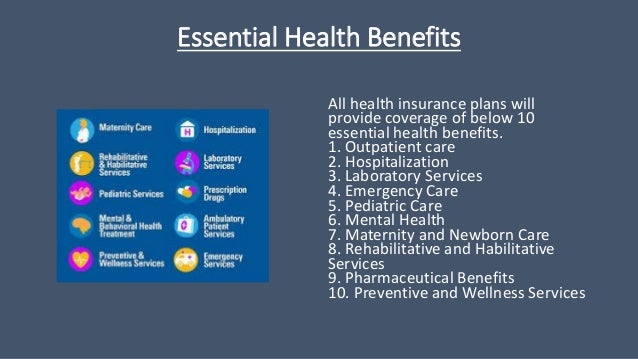
Both association health plans and short-term plans are less expensive than Obamacare plans because they offer limited coverage. They don’t guarantee same-cost coverage, or any coverage, for people with pre-existing illnesses and they do not cover a broad range of medical care, from addiction treatment to maternity care.
Critics have referred to the plans as “junk insurance,” warning that expanding access to them would take customers back to the days before the passage of Obamacare, formally known as the Affordable Care Act. They also warn that providing such options would peel more people from Obamacare’s exchanges, leaving an even sicker — and costly — population with Obamacare plans.
But people who don’t receive federal help paying for their premiums, meaning people who make more than $48,240 for an individual or $98,400 for a family of four, and who do not have a pre-existing illness, may look to use one of the options. Many of those customers are facing double-digit premium increases in 2018. The number of people who have unsubsidized health insurance is pegged at anywhere from 6 to 9 million people. Some will face insurance that is so expensive that under Obamacare they will not be required to pay the law’s penalty if they decide not to get coverage.
The executive order could offer an alternative, but it’s not clear how quickly the plans will become available to customers. Open enrollment for Obamacare begins Nov. 1 and runs through Dec. 15, and officials at the different agencies may not be able to change regulations in time for the start of 2018. The White House declined to provide details about the timeline for implementing the executive order.
Kathy Bakich, national health compliance practice leader at Segal Consulting, said the association health plan regulations may take longer than the short-term plans because the administration may have to propose new rules and take public comments, which could take months. The original rules took more than a decade to create, she said.
“There is a legitimate need in the marketplace for new types of systems to allow small employers to band together,” she said. “Whether this is the right way to do it is a tough question.”
It’s not clear how far the changes to the regulations can go. Depending on how they are written, they raise potential openings for fraud or for insolvency if claims exceed an association’s ability to pay them out, because states won’t be able to regulate plans that are sold elsewhere to crack down on problems or revoke licensing. Bakich raised the possibility of another option, known as reinsurance, that would inject federal funding into the exchanges so that higher-cost claims were paid for while others who have coverage would not see premium increases, but there is little appetite among most Republicans for such a proposal.
Instead, association health plans have been pushed even among House members, who passed a bill to allow more of them earlier this year.
“Unlike larger organizations, America’s small businesses are limited in their ability to negotiate for lower healthcare costs for their millions of employees,” said Rep. Virginia Foxx, R-N.C., chairwoman of the House Education and the Workforce Committee. “It’s time to level the playing field. That’s why the committee advanced and the House passed common-sense legislation to allow small businesses to band together through association health plans.”
Trump had been discussing the idea of association health plans with Sen. Rand Paul, R-Ky., for months. On Tuesday he said on Twitter that he was moving to act because Congress “can’t get its act together on healthcare.” Paul chimed in as well, sharing Trump’s tweet and calling it a “great plan” and a “big deal for millions of Americans.”
“Sen. Paul brought this idea to President Trump as a way to fix many problems in the individual market without more regulations and spending,” Doug Stafford, chief strategist for Paul’s political action committee, said in an email. “They have worked on this for quite some time now and are pleased it will be enacted soon.”
The association health plans could allow members of different industries to band together or allow individuals to join in. The proposal has been billed as one that would allow people to buy insurance across state lines because health plans could be located in states with fewer regulations, which would make them less expensive.
The proposal on short-term plans may be easier to tackle. The Obama administration changed the rules for short-term plans in fall 2016, saying they could be offered for only 90 days at a time, meaning that a customer’s deductible would renew if he were to purchase a plan again at a later date. Prior to that, insurers stretched the definition of “short-term,” with some providing coverage for as long as 364 days. It’s not clear what the difference in pricing will be, but in 2016 the average price for an Obamacare premium was $393 a month and short-term plans averaged about $124 a month. By 2017 unsubsidized premiums for mid-level Obamacare plans had risen across the country by an average of 22 percent and are expected to rise in the double-digits again next year.
Insurers have said that the increases are a result of uncertainty over how the Trump administration or Congress would change Obamacare, but also from incurring losses from selling the plans, which younger, healthier and cheaper enrollees haven’t flocked to.
Obamacare, Bakich said, left a gap in terms of dealing with people who don’t think they can afford the robust coverage and also say they don’t want a wide range of services.
“They just want to be protected from bankruptcy and buy the catastrophic plan and be protected from losing everything in a medical crisis,” she said.
Kev Coleman, head of research and data for HealthPocket, a website that helps consumers compare and buy health plans, said he is a proponent of allowing short-term plans to be used for a longer period, saying that industry data show people use them for about six months and that they are meant to be transitional.
Short-term plans and Obamacare plans have locked in rates with states for 2018 and that will not change the individual market, he said.
He also disputed that the short-term plans would be destabilizing to the Obamacare exchange, noting that the Obama-era regulations went into effect in April and that the number of people who used them previously were small. Data from 2015 peg customers at 148,100.
“This market has been around for decades and it hasn’t been a destabilizing force,” Coleman said.
Larry Levitt, senior vice president for special initiatives at the Kaiser Family Foundation, said on Twitter that people who don’t receive subsidies but who have pre-existing illnesses such as cancer or diabetes would be particularly vulnerable because the short-term and association plans wouldn’t cover their medical needs.
“Short-term insurance plans can offer inexpensive coverage to currently healthy people, but they would exclude people with pre-existing conditions,” he wrote. “If healthy people can enroll in short-term plans and avoid the individual mandate penalty, the ACA marketplaces could collapse. Anything that creates a parallel insurance market for healthy people will lead to unaffordable coverage for sick people.”
But Coleman said working within the existing Obamacare system hasn’t worked.
“Politicians interested in optimizing the health of ACA risk pools would be well-advised to work backwards from consumers’ insurance priorities in order to arrive at a compelling market solution,” Coleman said. “You can’t achieve healthy risk pools without a product that has broad appeal.”