If a picture is worth a thousand words, a video, if done well, can be worth thousands more.
Regular readers of HEALTH CARE un-covered know we have published lots of words about the barriers health insurance companies have erected that make it harder and harder for patients to get the care their doctors know they need.
It’s a perfect example of how something that was designed to protect patients from inappropriate and unnecessary care has been weaponized by health insurers to pad their bottom lines.
Prior authorization in today’s world all too often serves as a bureaucratic barrier, requiring patients and their doctors to obtain approval in advance from insurers before certain treatments, medications, or procedures will be covered.
While insurance companies argue that prior authorization helps control costs and ensure appropriate care, the reality is far grimmer.
Both patients and their health care providers suffer the consequences. Patients frequently face delays in receiving necessary treatments or medications, exacerbating their health conditions and causing unnecessary stress and anxiety. Many forgo needed care altogether due to the complexities and frustrations of navigating the prior authorization process. This practice not only undermines patients’ trust in their health care providers but also compromises their health, often leading to worsened conditions and, tragically, sometimes irreversible harm.
The burden of prior authorization falls heavily on clinicians and their office staff who must spend valuable time and resources navigating the bureaucratic red tape imposed by insurers. This administrative burden not only detracts from patient care but also contributes to physician burnout, dissatisfaction and moral crisis, according to many doctors.
Ultimately, the health insurance industry’s prioritization of profit over patient well-being is evident in its insistence on maintaining these barriers to care, perpetuating a system that defaults to financial gain at the expense of human lives.
The New York Times video cuts to the chase. Prior authorization, as practiced today by insurance companies, is “medical injustice disguised as paperwork.”
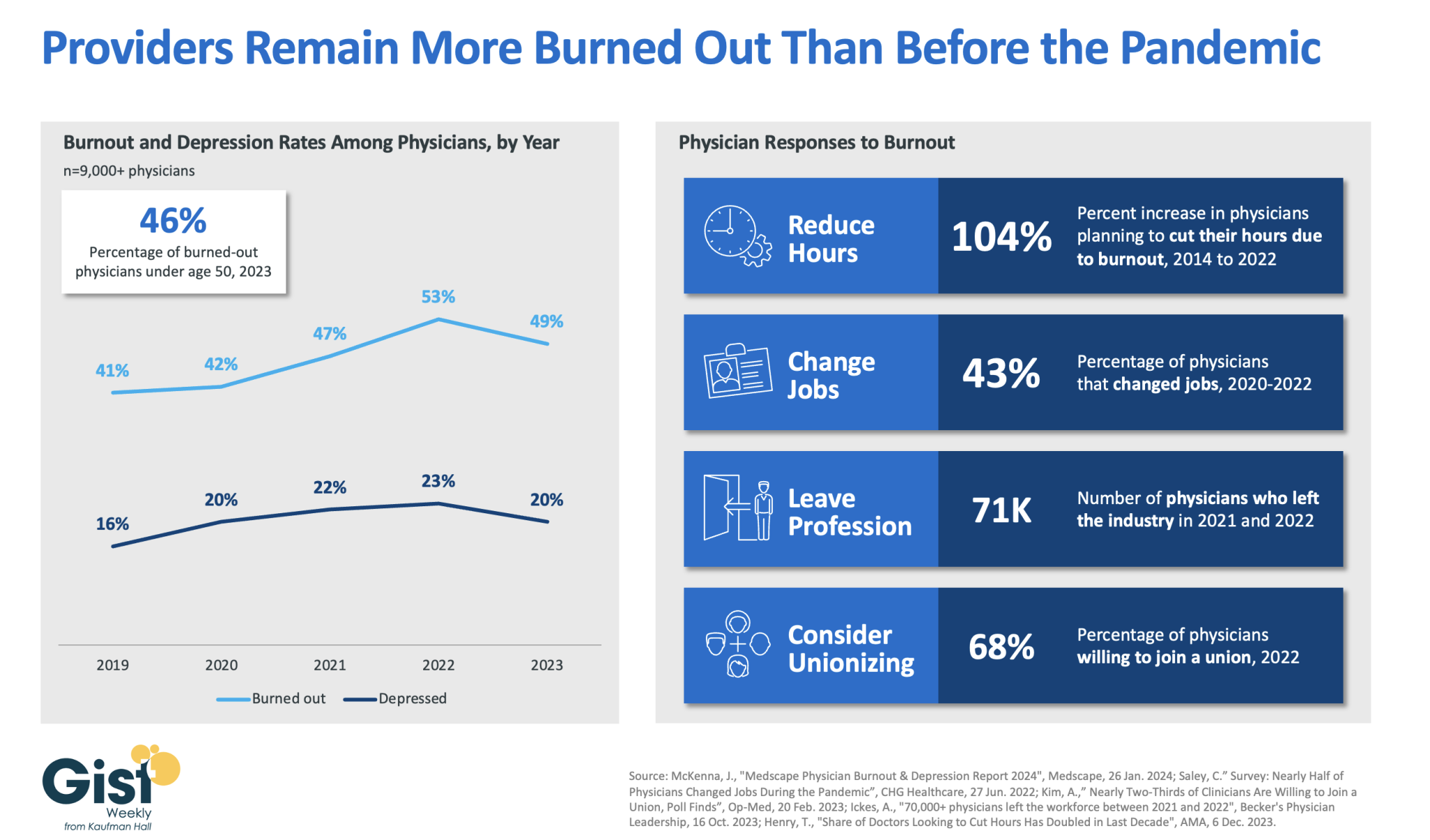
In 2023, nearly half of physicians reported feeling burned out, and a fifth reported feeling depressed. Although this does represent a drop from 2022’s peak, physicians remain more distressed than they were before the pandemic.
These numbers reveal some of the toll that the continued labor shortages, financial challenges, and payment changes of the past few years have taken on providers. In response to feeling burned out, an increased number of physicians say they are planning to cut their hours and over a third say they actually have changed jobs. Many have left the industry all together and the majority now say they are willing to join a union.
Health systems have long prioritized addressing provider burnout, but tighter operating margins have heightened both the challenge and the importance of helping to relieve it.
Continuing to find solutions to reduce administrative tasks, enhance team-based care models, and empower providers in decision-making processes are as important as ever for provider organizations today.
In Sunday’s Axios’ AM, Mike Allen observed “Republicans know immigration alone could sink Biden. So, Trump and House Republicans will kill anything, even if it meets or exceeds their wishes. Biden knows immigration alone could sink him. So he’s willing to accept what he once considered unacceptable — to save himself.”
Mike called this a “truth Bomb” and he’s probably right: the polarizing issue of immigration is tantamount to a bomb falling on the political system forcing well-entrenched factions to re-think and alter their strategies.
In 2024, in U.S. healthcare, three truth bombs are in-bound. They’re the culmination of shifts in the U.S.’ economic, demographic, social and political environment and fueled by accelerants in social media and Big Data.
Truth bomb: The regulatory protections that have buoyed the industry’s growth are no longer secure.
Despite years of effectively lobbying for protections and money, the industry’s major trade groups face increasingly hostile audiences in city hall, state houses and the U.S. Congress.
The focus of these: the business practices that regulators think protect the status quo at the public’s expense. Example: while the U.S. House spent last week in their districts, Senate Committees held high profile hearings about Medicare Advantage marketing tactics (Finance Committee), consumer protections in assisted living (Special Committee on Aging), drug addiction and the opioid misuse (Banking) and drug pricing (HELP). In states, legislators are rationalizing budgets for Medicaid and public health against education, crime and cybersecurity and lifting scope of practice constraints that limit access.
Drug makers face challenges to patents (“march in rights”) and state-imposed price controls. The FTC and DOJ are challenging hospital consolidation they think potentially harmful to consumer choice and so. Regulators and lawmakers are less receptive to sector-specific wish lists and more supportive of populist-popular rules that advance transparency, disable business relationships that limit consumer choices and cede more control to individuals. Given that the industry is built on a business-to-business (B2B) chassis, preparing for a business to consumer (B2C) time bomb will be uncomfortable for most.
Truth bomb: Affordability in U.S. is not its priority.
The Patient Protection and Affordability Act 2010 advanced the notion that annual healthcare spending growth should not exceed more than 1% of the annual GDP. It also advanced the premise that spending should not exceed 9.5% of household adjusted gross income (AGI) and associated affordability with access to insurance coverage offering subsidies and Medicaid expansion incentives to achieve near-universal coverage. In 2024, that percentage is 8.39%.
Like many elements of the ACA, these constructs fell short: coverage became its focus; affordability secondary.
The ranks of the uninsured shrank to 9% even as annual aggregate spending increased more than 4%/year. But employers and privately insured individuals saw their costs increase at a double-digit pace: in the process, 41% of the U.S. population now have unpaid medical debt: 45% of these have income above $90,000 and 61% have health insurance coverage. As it turns out, having insurance is no panacea for affordability: premiums increase just as hospital, drug and other costs increase and many lower- and middle-income consumers opt for high-deductible plans that expose them to financial insecurity. While lowering spending through value-based purchasing and alternative payments have shown promise, medical inflation in the healthcare supply chain, unrestricted pricing in many sectors, the influx of private equity investing seeking profit maximization for their GPs, and dependence on high-deductible insurance coverage have negated affordability gains for consumers and increasingly employers. Benign neglect for affordability is seemingly hardwired in the system psyche, more aligned with soundbites than substance.
Truth bomb: The effectiveness of the system is overblown.
Numerous peer reviewed studies have quantified clinical and administrative flaws in the system. For instance, a recent peer reviewed analysis in the British Medical Journal concluded “An estimated 795 000 Americans become permanently disabled or die annually across care settings because dangerous diseases are misdiagnosed. Just 15 diseases account for about 50.7% of all serious harms, so the problem may be more tractable than previously imagined.”
The inadequacy of personnel and funding in primary and preventive health services is well-documented as the administrative burden of the system—almost 20% of its spending. Satisfaction is low. Outcomes are impressive for hard-to-diagnose and treat conditions but modest at best for routine care. It’s easier to talk about value than define and measure it in our system: that allows everyone to declare their value propositions without challenge.
Truth bombs are falling in U.S. healthcare. They’re well-documented and financed. They take no prisoners and exact mass casualties.
Most healthcare organizations default to comfortable defenses. That’s not enough. Cyberwarfare, precision-guided drones and dirty bombs require a modernized defense. Lacking that, the system will be a commoditized public utility for most in 15 years.
PS: Last week’s report, “The Holy War between Hospitals and Insurers…” (The Keckley Report – Paul Keckley) prompted understandable frustration from hospitals that believe insurers do not serve the public good at a level commensurate with the advantages they enjoy in the industry. However, justified, pushback by hospitals against insurers should be framed in the longer-term context of the role and scope of services each should play in the system long-term. There are good people in both sectors attempting to serve the public good. It’s not about bad people; it’s about a flawed system.
Medicare Advantage provides health coverage to more than half of the nation’s seniors, but a growing number of hospitals and health systems nationwide are pushing back and dropping the private plans altogether.
Among the most commonly cited reasons are excessive prior authorization denial rates and slow payments from insurers. Some systems have noted that most MA carriers have faced allegations of billing fraud from the federal government and are being probed by lawmakers over their high denial rates.
“It’s become a game of delay, deny and not pay,” Chris Van Gorder, president and CEO of San Diego-based Scripps Health, told Becker’s.
“Providers are going to have to get out of full-risk capitation because it just doesn’t work — we’re the bottom of the food chain, and the food chain is not being fed.”
In late September, Scripps began notifying patients that it is terminating Medicare Advantage contracts for its integrated medical groups, a move that will affect more than 30,000 seniors in the region. The medical groups, Scripps Clinic and Scripps Coastal, employ more than 1,000 physicians, including advanced practitioners.
Mr. Van Gorder said the health system is facing a loss of $75 million this year on the MA contracts, which will end Dec. 31 for patients covered by UnitedHealthcare, Anthem Blue Cross, Blue Shield of California, Centene’s Health Net and a few more smaller carriers. The system will remain in network for about 13,000 MA enrollees who receive care through Scripps’ individual physician associations.
“If other organizations are experiencing what we are, it’s going to be a short period of time before they start floundering or they get out of Medicare Advantage,” he said. “I think we will see this trend continue and accelerate unless something changes.”
Bend, Ore.-based St. Charles Health System has taken it a step further and is not only considering dropping all Medicare Advantage plans, but is also encouraging its older patients not to enroll in the private Medicare plans during the upcoming enrollment period in October.
The health system’s president and CEO, CFO and chief clinical officer cited high rates of denials, longer hospital stays and overall administrative burden for clinicians.
“We recognize changing insurance options may create a temporary burden for Central Oregonians who are currently on a Medicare Advantage plan, but we ultimately believe it is the right move for patients and for our health system to be sustainable into the future to encourage patients to move away from Medicare Advantage plans as they currently exist,” St. Charles Health CFO Matt Swafford said.
“I feel terrible for the patients in this situation; it’s the last thing we wanted to do, but it’s just not sustainable with these kinds of losses,” Mr. Van Gorder added. “Patients need to be aware of how this system works. Traditional Medicare is not an issue. With these other models, seniors need to be wary and savvy buyers.”
Here are six more recent examples of hospitals dropping Medicare Advantage contracts:
1. Adena Regional Medical Center is terminating its contract with Anthem BCBS’ Medicare Advantage and managed Medicaid plans in Ohio, effective Nov. 2. The flagship facility of Chillicothe, Ohio-based Adena Health System said rate negotiations between the organizations “have not been productive,” leading it to terminate its agreement with Anthem, whose parent company is Elevance Health.
2. Corvallis, Ore.-based Samaritan Health Servicesended its commercial and Medicare Advantage contracts with UnitedHealthcare. The five-hospital, nonprofit health system cited slow “processing of requests and claims” that have made it difficult to provide appropriate care to UnitedHealth’s members, which will be out of network with Samaritan’s hospitals on Jan. 9. Samaritan’s physicians and provider services will be out of network on Nov. 1, 2024.
3. Cameron (Mo.) Regional Medical Center stopped accepting Cigna’s MA plans in 2023 and plans to drop Aetna and Humana in 2024. It plans to continue Medicare Advantage contracts with UnitedHealthcare and BCBS, the St. Joseph News-Press reported in May. Cameron Regional CEO Joe Abrutz previously told the newspaper the decision stemmed from delayed reimbursements.
4. Stillwater (Okla.) Medical Centerended all in-network contracts with Medicare Advantage plans amid financial challenges at the 117-bed hospital. Humana and BCBS of Oklahoma were notified that their MA members would no longer receive in-network coverage after Jan. 1, 2023. The hospital said it made the decision after facing rising operating costs and a 22 percent prior authorization denial rate for Medicare Advantage plans, compared to a 1 percent denial rate for traditional Medicare.
5. Brookings (S.D.) Health System will no longer be in network with any Medicare Advantage plans in 2024, the Brookings Register reported. The 49-bed, municipally owned hospital said the decision was made to protect the financial sustainability of the organization.
6. Louisville, Ky.-based Baptist Health Medical Group went out of network with Humana’s Medicare Advantage and commercial plans on Sept. 22, Fox affiliate WDRB reported.
Published this week in the Harvard Business Review, this intriguing case study tells the story of how Hawaii Pacific Health, a four-hospital system based in Honolulu, worked with its providers to reduce the deluge of needless or low-value administrative tasks required each day by the system’s electronic health record (EHR) platform.
The system’s “Get Rid of Stupid Stuff” (GROSS) initiative created a simple, accessible submission form that allowed providers to flag EHR prompts and workflows ranging from inefficient (printing and scanning discharge papers patients had already signed electronically) to nonsensical (affirming adolescent patients had received proper care for their non-existent umbilical cords). Around 10 percent of suggestions submitted were for prompts that could be immediately eliminated, 15 percent caught gaps in communication and workflow, and the remaining 75 percent identified more complex opportunities for redesign. The GROSS initiative not only freed thousands of labor hours, but also boosted morale by engaging clinicians in the system’s efforts to improve operations.
The Gist: While Hawaii Pacific Health is far from the only system to have successfully engaged its providers in the mission of reducing administrative busywork, this case study provides an example of how sometimes the simplest approaches can be the most effective.
As systems now look to generative AI as the next frontier of bureaucratic efficiency, they will need to optimize workflow processes before automating them in order to avoid ingraining today’s inefficiencies.
The film “American Hospitals: Healing a Broken System” premiered in Washington, D.C., on March 29. This documentary exposes the inconvenient truths embedded within the U.S. healthcare system. Here is a dirty dozen of them:
Hospitals are largely unaccountable for poor clinical outcomes.
The cost of commercially insured care is multiples higher than the cost of government-insured care for identical procedures.
Customer service at hospitals is dreadful.
Frontline clinicians are overburdened and leaving the profession in droves.
Healthcare still operates the same way it has for the last one hundred years — delivering hierarchical, fragmented, hospital-centric, disease-centric, physician-centric “sick” care. Accordingly, healthcare business models optimize revenue generation and profitability rather than health outcomes. These factors explain, in part, why U.S. life expectancy has declined four of the five years and maternal deaths are higher today than a generation ago.
It’s hard to imagine that the devil itself could create a more inhumane, ineffective, costly and change-resistant system. Hospitals consume more and more societal resources to maintain an inadequate status quo. They’re a major part of America’s healthcare problem, certainly not its solution. Even so, hospitals have largely avoided scrutiny and the public’s wrath. Until now.
“American Hospitals” is now playing in theaters throughout the nation. It chronicles the pervasive and chronic dysfunction plaguing America’s hospitals. It portrays the devastating emotional, financial and physical toll that hospitals impose on both consumers and caregivers.
Despite its critical lens, “American Hospitals” is not a diatribe against hospitals. Its contributors include some of healthcare’s most prominent and respected industry leaders, including Donald Berwick, Elizabeth Rosenthal, Shannon Brownlee and Stephen Klasko. The film explores payment and regulatory reforms that would deliver higher-value care. It profiles Maryland’s all-payer system as an example of how constructive reforms can constrain healthcare spending and direct resources into more effective, community-based care.
The United States already spends more than enough on healthcare. It doesn’t need to spend more. It needs to spend more wisely. The system must downsize its acute and specialty care footprint and invest more in primary care, behavioral health, chronic disease management and health promotion. It’s really that simple.
My only critique of “American Hospitals” is many of its contributors expect too much from hospitals. They want them to simultaneously improve their care delivery and advance the health of their communities. This is wishful thinking. Health and healthcare are fundamentally different businesses. Rather than pivoting to population health, hospitals must focus all their efforts on delivering the right care at the right time, place and price.
If hospitals can deliver appropriate care more affordably, this will free up enormous resources for society to invest in health promotion and aligned social-care services. In this brave new world, right-sized hospitals deliver only necessary care within healthier, happier and more productive communities.
All Americans deserve access to affordable health insurance that covers necessary healthcare services without bankrupting them and/or the country. Let me restate the obvious. This requires less healthcare spending and more investments in health-creating activities. Less healthcare and more health is the type of transformative reform that the country could rally behind.
At issue is whether America’s hospitals will constructively participate in downsizing and reconfiguring the nation’s healthcare system. If they do so, they can reinvent themselves from the inside out and control their destinies.
Historically, hospitals have preferred to use their political and financial leverage to protect their privileged position rather than advance the nation’s well-being. Like Satan in Milton’s “Paradise Lost,” they have preferred to reign in hell rather than serve in heaven.
Pride comes before the fall. Woe to those hospitals that fight the nation’s natural evolution toward value-based care and healthier communities. They will experience a customer-led revolution from outside in and lose market relevance. Only by admitting and addressing their structural flaws can hospitals truly serve the American people.
A working paper published this week by the National Bureau of Economic Research found that prior authorization requirements reduced drug spending far more than they increased physicians’ administrative costs.
Using a random assignment of plans within Medicare Part D’s low-income subsidy program, the study determined that a prior authorization requirement decreased a drug’s utilization by just over 25 percent, with around half of denied beneficiaries opting for a comparable alternative and the other half receiving no drug at all. This generated $96 in per-beneficiary-per-year savings, which the authors estimate to be around 10 times greater than the administrative costs incurred.
The Gist: Physician groups have long despised prior authorization processes, listing it as their most burdensome regulatory issue. While studies like this are useful for demonstrating the returns from these processes and putting the tradeoffs in perspective, they fail to account for who is bearing the burden of the time spent, and who captures the cost savings: physicians bear the administrative costs, and payers capture the returns. Not to mention that worried patients, anxious to receive treatment, are often put in the position of “quarterbacking” a convoluted and bureaucratic appeals process.
Ongoing work should focus on streamlining authorizations, to lessen the impact on physicians’ time and satisfaction, and make navigating the process simpler for patients. An increasing array of technology options aims to solve this problem though automation, but the challenge remains for payers and providers to come together to deliver on that potential.