

Cartoon – A Motion has been made

The former CFO of Huntsville (Texas) Memorial Hospital is suing the hospital for breach of contract and defamation, according to the SE Texas Record.
In his complaint, filed Aug. 28, Guy Gros claims he was hired as Huntsville Memorial’s CFO in February 2013. He was initially given a two-year contract and then a three-year contract with automatic renewals, according to the lawsuit.
Under the contract, the hospital could terminate Mr. Gros’s employment for cause. On Dec. 2, 2016 he was terminated for alleged cause. However, Mr. Gros asserts that he was fired for raising concerns about the hospital’s finances.
Mr. Gros further alleges his reputation was damaged by false statements made by the hospital’s then CEO, who allegedly told a board member that Mr. Gros “did something illegal, something he should not have.”
Mr. Gros is seeking past and future wages, lost employment benefits and compensatory damages.
https://www.modernhealthcare.com/hospitals/critical-steps-hospital-turnaround
The challenges many community hospitals face have become so unrelenting as to threaten long-term financial viability. It’s important that this threat be met with prompt action and operational changes that can improve the immediate situation as well as sustainability. A formal turnaround plan includes analyses and actions, and becomes a roadmap to redirect hospitals and help them stay on track to serve as community resources for years to come.
JK: Leaders from ailing community hospitals sometimes don’t recognize the severity of their problems or that certain indicators call for quick, corrective action. Some common alarm signals that leaders may tune out at first include a downward trend of days cash on hand, shifts in patient volume across the delivery spectrum, medical staff dissatisfaction or defection, and even bond covenant concerns. Recognizing that problems need to be addressed and changes must be made is the first step toward improvement.
JK: Typically, the process starts with an operational assessment to evaluate strategy, operations, supply chain, revenue cycle and leadership with the aim of reducing costs and increasing revenue—the tried-and-true formula for financial solvency. The analysis includes a review of data and documents, as well as interviews with board, executive and physician leaders. The process reveals any organizational problems or vulnerabilities that aren’t immediately apparent, and it forms the basis for a turnaround plan, including a detailed action plan. An open mind and fresh perspective are important to be able to see options to go beyond operations as they have always been.
JK: Almost every hospital has room to improve staff productivity. Labor is a hospital’s greatest expense, so optimizing productivity by having the right number and mix of staff can make a big impact. Community hospitals that do not have a productivity tool to achieve and maintain the right staffing levels can typically find savings of 15 to 20 percent in salaries and benefits by implementing a tool. In those hospitals where there’s already some productivity monitoring, implementing a more effective tool or improving processes can result in 5 to 10 percent savings. After labor, supply costs are the second highest expense for a hospital, so that’s another key focus area for cost reduction and savings. Industry benchmarks show that many community hospitals have an opportunity to reduce supply costs by as much as 20 percent.
Assessing revenue cycle is also imperative to help identify, monitor and collect every dollar a hospital is due. Gains can be made in this area by renegotiating health plan contracts, streamlining billing for faster payment, auditing medical record coding and reviewing the chargemaster.
JK: Hospitals can potentially identify significant cost-saving opportunities by comparing themselves to hospitals of similar size and volume. Comparing clinical, operational and financial data also identifies areas for improvement and where to allocate time and money for improvement initiatives. For example, a CHC-managed hospital that recently underwent a successful turnaround had discovered through benchmarking that its staff ratios were higher and its benefits were more expensive compared to similar hospitals. This information prompted leaders to take a closer look at the hospital’s situation, and they found it made sense from a sustainability perspective to downsize staff and bring benefit packages to competitive levels. These actions slashed the hospital’s annual expenses by $5.3 million.
JK: It’s a collaborative process requiring the participation of the board of trustees, executive leaders, physician leaders, and in many cases an outside management firm to evaluate the situation and develop a specific plan of action. As we discussed, leaders of struggling hospitals usually see the need for improvement but don’t recognize the severity of their situation. Because of that blind spot, it’s often external stakeholders or bondholders who set corrective action in motion by seeking outside assistance.
https://www.healthleadersmedia.com/strategy/ceo-kevin-spiegel-leaves-erlanger-amid-physicians-rancor

The top executive of Erlanger Health System, based in Chattanooga, Tennessee, has left the organization after months of smoldering conflict with some of the nonprofit’s physicians.
President and CEO Kevin Spiegel’s departure was immediate, according to a statement released Wednesday by board chairman Mike Griffin, who offered his well-wishes to the departing leader.
Spiegel, who had been on the job more than six years, reportedly said his separation from the organization was a mutual decision.
“We’re still working out the details, and hopefully that’ll be complete by the board meeting in two weeks,” Spiegel told the Times Free Press‘ Elizabeth Fite. “This is a great hospital, and it’s a great organization, and it’s only going to do better and better things.”
Erlanger’s board is expected to pick Spiegel’s successor in two weeks, at its regularly scheduled board meeting, according to Griffin’s statement.
Spiegel’s exit comes less than two weeks after the board held a special public meeting to talk about physicians’ concerns and criticism of Erlanger’s senior leadership team.
Spiegel is the third high-ranking Erlanger executive to leave since Fite reported in June on a letter from the Medical Executive Committee explaining its reasons for a unanimous vote of “no confidence” in the current executive leadership team. The other two were Executive Vice President and Chief Operating Officer Rob Brooks and Vice President of Patient Safety and Quality Pam Gordon.
Spiegel has been credited with leading Erlanger out of choppy financial waters, but he has also been caught up in a number of controversies, as the Times Free Press reported.

For some hospital chains and health insurers, CEO departures are anything but a clean break. Employment agreements outline long, expensive goodbyes that compensation experts say may be designed in part to enforce noncompete agreements.
Investor-owned companies like HCA Healthcare and health insurer Anthem have contracts in place with current and recently departed CEOs outlining the terms of paid consulting gigs they step into once their tenures as the top executive end. The contracts ensure leadership will continue to be paid handsomely for scaled-back workloads.
Even though Joseph Swedish retired from Anthem’s top spot in November 2017, the company pays him $4.5 million per year plus benefits to serve as a consultant and senior adviser to the CEO, currently Gail Boudreaux. The contract, which runs until May 2020, doesn’t spell out specific time commitments, but says he’ll perform duties assigned to him by the CEO “from time to time.” Anthem didn’t respond to requests for an explanation about the agreement.
Former HCA CEO R. Milton Johnson, who stepped down at the end of 2018, will make up to $3 million in base pay, stock awards and bonus pay in calendar 2019 plus benefits for his role as executive adviser. He also served as HCA’s board chairman through April 26. The agreement requires he work 20% of his average level of service in the three years before stepping down.
It’s not clear how common it is for companies to keep former CEOs on their payrolls as consultants. Modern Healthcare’s analysis was limited to large publicly traded health systems and insurers, but the practice could also take place at private and not-for-profit healthcare companies, although those contracts would not be publicly available.
Such deals may be struck in part to add teeth to noncompete agreements that preclude those CEOs from working at similar companies in the years immediately following their employment, said David McMillan, managing principal of strategy and integration at consultancy PYA. Noncompete agreements tend to be difficult to enforce, and adding pay into the mix strengthens them, he said.
“This might be a nice workaround to say, ‘I have you under contract and I’m compensating you. As part of that contract, you can’t compete with me,’ ” McMillan said. “In essence, I’ve just monetized the noncompete and created more enforceability so I don’t lose intellectual property.”
Several of the CEOs with consulting agreements also have noncompete agreements. HCA’s Johnson, for example, can’t engage in any work that competes with HCA for two years after his advisory role ends.
Dallas-based hospital chain Tenet Healthcare Corp.’s employment agreement with its current CEO, Ron Rittenmeyer, ends June 30, 2021. In each of the two years that follow, Tenet will pay Rittenmeyer $750,000 for working a maximum of eight days per month as a consultant. Rittenmeyer is also covered under a noncompete agreement that lasts for one year after he steps down as CEO.
A Tenet spokeswoman said post-employment consulting is a common way to ensure smooth transitions from one leadership team to another.
Franklin, Tenn.-based Community Health Systems’ former chief financial officer, Larry Cash, retired in May 2017, but still makes $300,000 a year working as a consultant for the investor-owned hospital chain. His employment agreement, which runs through March 2020, bars him from working for any CHS competitors, affiliates or suppliers during his time as a consultant.
The agreement with Cash gives CHS access to his 20 years of historical knowledge of company matters, CHS spokeswoman Tomi Galin wrote in an email.
Beyond enforcing noncompete agreements, there are other operational benefits to keeping former CEOs on the payroll. It adds continuity during the CEO transition period, with the former CEO acting as a sounding board for the new one, said Allen Reed, a partner in Odgers Berndtson’s healthcare and life sciences practices.
Deb Bilak, a partner with human resources consultancy Mercer, said companies sometimes transition the outgoing CEO to a consulting role when that executive has not yet completed a strategic initiative that was launched during his or her tenure. While the practice happens in other industries, it may be more common in healthcare given ongoing transformation in the sector.
“There’s so much going on in healthcare and health plans as far as consolidation and transformation that we are seeing that they want to retain that knowledge for a period of time,” Bilak said.
Compensation for consulting is typically based on what the executive was making as CEO and the time commitment required, Bilak said.
The consulting gigs, while high-paying, don’t pay the executives at the levels they made as CEO.
HCA’s Johnson made about $21.4 million in total compensation in 2018. Tenet’s Rittenmeyer made nearly $15 million in total compensation that year. Anthem CEO Swedish, meanwhile, made about $18.6 million in total compensation in 2017, his last year in that role.
Consulting agreements carry the potential downside of undermining the incoming CEO, especially if that person was recruited externally and there’s no established relationship between the new CEO and the organization, Paul Bohne, managing partner and healthcare practice leader with WittKieffer, wrote in an email. Staff members, directors and physicians are accustomed to the former CEO making decisions, and it can be tough to break those habits.
“Even with the best intentions, it is difficult to decondition others in the ways they were accustomed to working with the outgoing CEO,” Bohne said.
Not all outgoing CEOs become consultants. Organizations that want to retain the CEO’s knowledge may opt to put the executive on the board of directors instead.
After Michael Neidorff retires as CEO of Medicaid managed-care insurer Centene Corp. in 2023, for example, he’ll stay on as executive chairman of the board for a year before becoming non-executive board chairman, according to a February 2019 amendment to Neidorff’s employment agreement.
The agreement doesn’t detail compensation, but states that “for the remainder of his life,” Neidorff will have access to a full-time administrative assistant and an office at the company’s headquarters. During his time as chairman and for five years after, Centene will require he use the company’s aircraft for all air travel.
Longtime DaVita CEO Kent Thiry will make up to $2 million in base and bonus pay for serving as executive chairman of the company’s board for one year following his retirement, which was effective June 1. That’s a far cry from his $32 million in total compensation in 2018, but much more than DaVita’s director salaries that year, which ranged from about $323,000 to $445,000.
Thiry continues to provide counsel and is active in the company’s policy efforts to deliver integrated kidney care, DaVita spokeswoman Courtney Culpepper wrote in an email.
The difference in pay could spell problems if fellow directors protest the disparity, Reed said.
“That’s probably where it would be more favorable to have a consulting engagement,” he said.
On the other hand, directors have a legal and fiduciary responsibility to the company, McMillan said.
“The additional value the organization is getting is the duty of care that comes along with a board position,” he said.
https://www.jpmorgan.com/commercial-banking/insights/healthcare-mixed-outlook

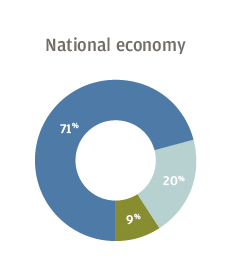
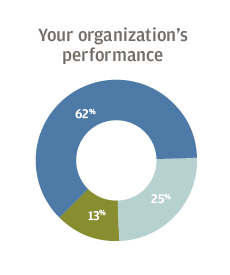
In a recent survey of healthcare leaders, most were confident about their own organizations going into the new year. But respondents expressed concern about a range of evolving industry-wide challenges, including costs, technology and talent.
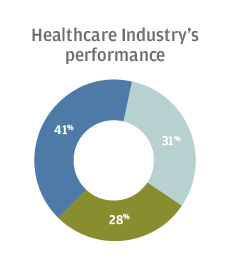
A majority of US healthcare executives surveyed by J.P. Morgan said they were optimistic about the financial performance of their own organizations going into 2019, as well as the national and local economies. But most were less positive about the outlook for the industry as a whole, with 28 percent expressing pessimism and another 31 percent merely neutral.



Respondents to the survey, conducted Oct. 16 to Nov. 2 of 2018, said their biggest concerns were revenue growth, rising expenses and labor costs. The executives said their organizations plan to invest the most in information technology and physician recruitment.
The pessimism about the industry likely stems, in part, from regulatory uncertainty and an ongoing shift from a fee-for-service model toward a value-based payment system, said Will Williams, Senior Healthcare Industry Executive within J.P. Morgan’s Commercial Banking Healthcare group. “Healthcare is going through the most transition of any industry in the country right now,” he said. Amid this upheaval, healthcare organizations face a combination of challenges, including lower reimbursement rates for Medicaid and Medicare patients, increased competition, and higher costs for labor, pharmaceuticals and technology investments.
The optimism that executives feel about their own hospital or healthcare group may come from a sense that an individual organization can adapt to industry changes, said Jenny Edwards, Commercial Banker in the healthcare practice at J.P. Morgan. “You can control certain factors, and make adjustments to compensate for the headwinds.”


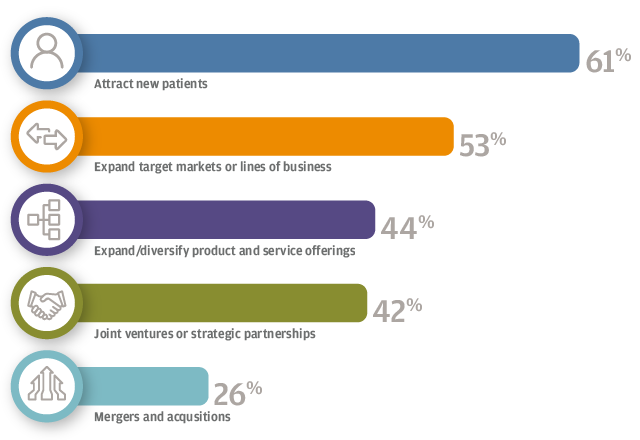
For 61 percent of respondents, the focus is on attracting new patients, followed by expanding target markets or lines of business (53 percent), and expanding or diversifying product and service offerings (44 percent). Hospitals, for example, have worked to add more patients to their broader healthcare system by opening clinics for urgent care or physical therapy, Edwards said.
As patient habits change, hospital systems have needed to become more consumer-focused, Edwards said. Patients are more likely to shop around for their care, expect transparent pricing and review healthcare workers on social media sites. This “retail-ization” trend in healthcare is accelerating, Edwards said. “You can shop for healthcare like you would a new pair of jeans.”
The talent shortage is top of mind for many healthcare executives, with 92 percent of survey respondents saying they were at least somewhat concerned with finding candidates with the right skill set. For 35 percent of respondents, the talent shortage is one of their top three challenges.
For those respondents who expressed concern, the most difficulty arises in filling positions for physicians (52 percent) and nurses (46 percent). To address the challenge, 76 percent said they expect to increase compensation of their staff over the next 12 months. According to 37 percent of respondents, the talent pool’s high compensation expectations factor into the shortage.





The talent shortage is an issue across the industry, Williams said, and burnout among doctors and nurses presents an ongoing problem. One contributing cause could be evolving changes in daily practice, with considerably more time today spent on electronic medical record entries and less on patient care. Williams said, “Doctors are getting frustrated. The problem is trying to replace those doctors as they quit practicing.”
Healthcare executives are particularly concerned about shortages of primary care professionals. “Rural communities already have these shortages,” said Brendan Corrigan, Vice Chair of the J.P. Morgan Healthcare Council.
Labor costs tend to be higher in healthcare than in other sectors, Williams said, as a hospital must have coverage for all of its major roles 24 hours a day. When asked where they struggle with workforce management, the survey respondents cite staff turnover and its associated cost (47 percent), the ability to flex staff based on patient volumes (41 percent), and the cost of overtime and premium labor (36 percent). These workforce issues not only represent specific challenges; they all contribute to labor costs, which, as noted above, rank in the top three challenges for 2019.
A majority (51 percent) of organizations plan to invest in IT over the next 12 months. Other areas for investment included physician recruitment (44 percent) and new or replacement facilities (36 percent).
Since healthcare organizations manage a large amount of private patient health information, data security remains a large part of IT expenditures. “It’s a huge focus—they’re spending a lot of time and money on preventing a breach,” Edwards said. She goes on to note that the transition to patient EMR systems brings another big IT expense—more than $1 billion for the largest healthcare systems.
Overall, the survey showed healthcare executives grappling with rising costs and structural changes that affect the entire industry. “Healthcare is trying to figure out how to fix themselves,” Williams said.
Click to access aha-2019-governance-survey-report_v8-final.pdf
https://www.healthleadersmedia.com/strategy/hospital-boards-seeing-low-turnover-rates-aha-finds

The boards of trustees governing U.S. hospitals and health systems have relatively low turnover rates in an industry that’s shifting rapidly, according to a survey report released Wednesday by the American Hospital Association.
The survey asked more than 1,300 CEOs of nonfederal community hospitals and health systems in the U.S. about their organizations’ governance structures and practices, then the AHA compared their responses to data collected in a similar survey five years ago.
The researchers found that the policies and norms in place for most healthcare organizations result in low levels of board turnover.
The report cited several related opportunities for improvement:
Luanne R. Stout, president of Stout Associates based in the Dallas/Fort Worth area and a retired Chief Governance Officer of Texas Health Resources, wrote in commentary included with the report that healthcare organizations have a number of options when trying to foster a healthy degree of board turnover.
“Term limits (usually three or four consecutive, three-year terms) are helpful in accomplishing board turnover; however, some boards are reluctant to adopt term limits for fear of losing highly valued board members,” Stout wrote. “Boards that annually review board member attendance, performance and contribution can achieve desired levels of rotation and competency enhancement without utilizing term limits.”
The AHA report also notes some positive trends around healthcare board governance, including the following:
“This year’s survey demonstrates how hospitals and health system boards are rising to meet tomorrow’s challenges through redefining roles, responsibilities and board structures,” said AHA President and CEO Rick Pollack in a statement. “These changes are not surprising given the continued transformation in where, how, when and from whom patients receive care.”
