Last week, California’s legislature passed a bill establishing the Distressed Hospital Loan Program, which will dole out $150M in interest-free emergency loans to struggling nonprofit hospitals in the state which meet specific eligibility criteria, including operating in an underserved area and serving a large share of Medicaid beneficiaries. A combination of state agencies will establish a specific methodology for selection, but hospitals that are part of a health system with more than two separately licensed hospital facilities will be ineligible.
Hospitals receiving loans must provide a plan for how they will use the loans to achieve financial sustainability, and must pay back the money within six years.
The Gist: With twenty percent of the state’s hospitals at risk of shuttering, California lawmakers are hoping to provide the most vulnerable hospitals an alternative to either closure or consolidation, an example other states may follow. But unlike the Paycheck Protection Program loans that shored up businesses through the pandemic’s initial disruption, the outlook for small, struggling, independent hospitals isn’t expected to improve in coming years, even if the economy recovers.
Whether these loans provide lifelines or merely serve as Band-Aids on an untenable situation will depend on whether recipient hospitals can use them to restructure their operating models to absorb increased labor costs amid stagnating volumes and commercial reimbursement.
If these loans aren’t used for transformation, they will only delay the inevitable: more closures, and more mergers to find shelter in scale.
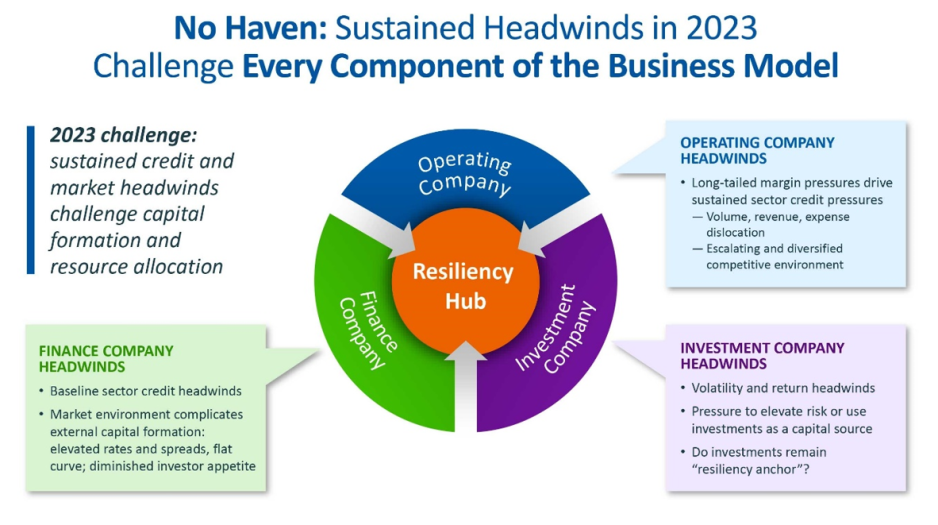
For the first time in recent history, we saw all three functions of the not-for-profit healthcare system’s financial structure suffer significant and sustained dislocation over the course of the year 2022 (Figure above).
The headwinds disrupting these functions are carrying over into 2023, and it is uncertain how long they will continue to erode the operating and financial performance of not-for-profit hospitals and health systems.
The Operating Function is challenged by elevated expenses, uncertain recovery of service volumes, and an escalating and diversified competitive environment.
The Finance Function is challenged by a more difficult credit environment (all three rating agencies
now have a negative perspective on the not-forprofit healthcare sector), rising rates for debt, and a diminished investor appetite for new healthcare debt issuance. Total healthcare debt issuance in 2022 was $28 billion, down sharply from a trailing two-year average of $46 billion.
The Investment Function is challenged by volatility and heightened risk in markets concerned with the Federal Reserve’s tightening of monetary policy and the prospect of a recession. The S&P 500—a major stock index—was down almost 20% in 2022. Investments had served as a “resiliency anchor” during the first two years of the pandemic; their ability to continue to serve that function is now in question.
A significant factor in Operating Function challenges is labor: both increases in the cost of labor and staffing shortages that are forcing many organizations to run at less than full capacity. In Kaufman Hall’s 2022 State of Healthcare Performance Improvement Survey, for example, 67% of respondents had seen year-over-year increases of more than 10% for clinical staff wages, and 66% reported that they had run their facilities at less-than-full capacity because of staffing shortages.
These are long-term challenges,
dependent in part on increasing the pipeline of new talent entering healthcare professions, and they will not be quickly resolved. Recovery of returns from the Investment Function is similarly uncertain. Ideally, not-for-profit health systems can maintain a one-way flow of funds into the Investment Function, continuing to build the basis that generates returns. Organizations must now contemplate flows in the other direction to access
funds needed to cover operating losses, which in many cases would involve selling invested assets at a loss in a down market and reducing the basis available to generate returns when markets recover.
The current situation demonstrates why financial reserves are so important:
many not-for-profit hospitals and health systems will have to rely on them to cover losses until they can reach a point where operations and markets have stabilized, or they have been able to adjust their business to a new, lower margin environment. As noted above, relief funding and the MAAP program helped bolster financial reserves after the initial shock of the pandemic. As the impact of relief funding wanes and organizations repay remaining balances under the MAAP program, Days Cash on Hand has begun to shrink, and the need to cover operating losses is hastening this decline. From its highest
point in 2021, Days Cash on Hand had decreased, as of September 2022, by:
29% at the 75th percentile, declining from 302 to 216 DCOH (a drop of 86 days)
28% at the 50th percentile, declining from 202 to 147 DCOH (a drop of 55 days)
49% at the 25th percentile, declining from 67 to 34 DCOH (a drop of 33 days)
Financial reserves are playing the role for which they were intended; the only question is whether enough not-for-profit hospitals and health systems have built sufficient reserves to carry them through what is likely to be a protracted period of recovery from the pandemic.
KEY TAKEAWAYS
All three functions of the not-for-profit healthcare system’s financial structure—operations, finance, and investments—suffered significant and sustained dislocation over the course of 2022.
These headwinds will continue to challenge not-forprofit
hospitals and health systems well into 2023.
Days Cash on Hand is showing a steady decline, as the impact of relief funding recedes and the need to cover operating losses persists.
Financial reserves are playing a critical role in covering operating losses as hospitals and health systems struggle to stabilize their operational and financial performance.
Conclusion
Not-for-profit hospitals and health systems serve many community needs. They provide patients access to healthcare when and where they need it. They invest in new technologies and treatments that offer patients and their families lifesaving advances in care. They offer career opportunities to a broad range of highly skilled professionals, supporting the economic health of the communities they serve.
These services and investments are expensive and cannot be covered solely by the revenue received from providing care to patients.
Strong financial reserves are the foundation of good financial stewardship for not-for-profit hospitals and health systems.
Financial reserves help fund needed investments in facilities and technology, improve an organization’s debt capacity, enable better access to capital at more affordable interest rates, and provide a critical resource to meet expenses when organizations need to bridge periods of operational disruption or financial distress. Many hospitals and health systems today are relying on the strength of their reserves to navigate a difficult
environment; without these reserves, they would not be able to meet their expenses and would be at risk of closure.
Financial reserves, in other words, are serving the very purpose for which they are intended—ensuring that hospitals and health systems can continue to serve their communities in the face of challenging operational and financial headwinds.
When these headwinds have subsided, rebuilding these reserves should be a top priority to ensure that our not-for-profit hospitals and health systems can remain a vital resource for the communities they serve.
For large capital projects—construction of a new cancer treatment center, for example, or replacement of an aging facility—issuance of municipal debt is one of the most affordable ways for not-for-profit hospitals and health system to finance the project.
The affordability of that debt is, however, partly contingent on the organization’s ability to maintain a strong credit rating, and financial reserves—again measured as Days Cash on Hand—are a significant component of that credit rating.
There are two basic forms of municipal debt:
General obligation bonds are backed by the full taxing power of the issuing municipal authority and are considered relatively low risk. Hospitals that are owned by a city or county can be funded by general obligation bonds, although there are practical limitations on their ability to issue these bonds, including in many instances the need to obtain voter or county commissioner approval. Organizations
without municipal ownership—including most not-for-profit hospitals and health systems— cannot issue general obligation bonds.
Revenue-backed municipal bonds are backed by the ability of the organization borrowing the debt to meet its obligation to make principal and interest payments through the revenue it generates over the life of the bond. Because revenues can be disrupted by any range of factors, revenue-backed bonds are higher risk for investors. Most healthcare bonds are revenue-backed municipal bonds.
When determining whether to invest in revenue-backed municipal healthcare bonds, investors will look to the credit rating of the hospital or health system that is borrowing the debt. Credit ratings—issued by one or more of the three major credit rating agencies (Fitch Ratings, Moody’s Investors Service, and S&P Global Ratings)—provide an assessment of the probability
that the hospital or health system will be able to meet the terms of the debt obligation. These ratings are tiered. A credit rating in the AA tier is better than a credit rating in the A tier, which is better than a rating in the BBB tier. Ratings below the BBB tier are considered sub-investment grade.
Organizations with a sub-investment grade rating can still access various forms of debt, but the amount of debt they can access generally will be lower, the cost of the debt will be higher, and the covenants that lenders require will be more stringent than for investment-grade rated organizations.
Financial reserves and credit ratings
Days Cash on Hand is one of the most important factors credit rating agencies use because it is an indicator of how long the rated organization could withstand serious disruption to its operations and cashflow. The rating agencies issue median values for the various metrics they use to determine credit ratings. Median
values for Days Cash on Hand increased significantly across most rating categories for all three agencies in 2020 and 2021; this reflects the temporary inflow of pandemic relief funding through, for example, the Coronavirus Aid, Relief, and Economic Security (CARES) Act.
We anticipate these medians will move closer to pre-pandemic levels as relief funds are exhausted and hospitals repay remaining balances on Medicare’s COVID-19 Accelerated and Advanced Payment (MAAP) program funds. But even before the pandemic, organizations in 2019 had a median Days Cash on Hand of 276 to 289 days at the AA level, 173 to 219 days at the A level, and 140 to 163 days at the BBB level.
In other words, the Days Cash on Hand benchmark for organizations seeking to maintain an investment-grade rating would be well over 100 Days Cash on Hand, and well over 200 Days Cash on Hand for organizations seeking to achieve a higher rating level. Again, these reserves are proportionate to the operating expenses of the individual hospital or health system.
Impact of credit ratings on access to capital
Organizations that can achieve a higher rating can also borrow money at more affordable interest rates. Figure 3 shows average interest rates for municipal bonds across a range of maturities as of mid-December 2022 (maturity is the term in years for repayment of the bond at the time the bond is issued). Lower-risk general obligation municipal bonds are shown as the baseline, with lines for AA, A, and BBB rated healthcare revenue-backed bonds above it. As a reminder, most hospitals and health systems cannot borrow money using general obligation bonds; instead, they use higher-risk revenue-backed bonds. Because revenue-backed bonds are a higher risk for investors than tax-based general obligation bonds,
even hospitals and health systems with a strong AA credit rating will pay a higher interest rate than would a city or county that could back repayment of the bond with tax revenues (see the line for AA rated Healthcare Revenue Bonds compared to the line for AAA rated General Obligation bonds). But there is also a significant gap between the interest rate a hospital with an AA credit rating would pay compared to the interest rate available to a hospital with a lower BBB rating. Here, the difference is approximately three-fourths of a full percentage point. When the amount borrowed for a major new hospital project can run into the hundreds of millions of dollars, that difference represents significant savings for organizations with a higher credit rating.
Financial reserves and debt capacity
Financial reserves and the funds they generate— including investment income—also help define an organization’s debt capacity: essentially, the amount of debt an organization can assume without jeopardizing its current credit rating. There are two key ratios here:
The first is total unrestricted cash and investments to debt. In general, the more favorable that ratio is, the more latitude a hospital or health system has to take on additional debt, especially if the organization is toward the middle to top end of its rating tier.
The second is the debt service coverage ratio, which measures the organization’s ability to make principal and interest payments with funds derived from both operating and non-operating (e.g., investment income) activity. A higher ratio here means the organization has more funds available to service debt.
The ability to assume additional debt is an important safety valve if, for example, an organization needs to mitigate poor financial performance to fund ongoing capital needs or strategic initiatives.
KEY TAKEAWAYS
Not-for-profit hospitals and health systems often borrow debt through revenue-backed municipal bonds, meaning that the debt obligations will be met by the revenue the organization generates over the life of the bond.
Because revenue-backed bonds are higher risk than general obligation bonds backed by a municipality’s taxing authority (revenues can be disrupted), investors seek assurance that an organization will be able to meet its obligations.
Credit ratings offer investors an assessment of an organization’s current and near-term ability to meet these obligations.
Days Cash on Hand is an important metric in assessing the organization’s credit rating, and a higher rating generally requires a higher number of Days Cash on Hand.
A higher credit rating allows organizations to borrow money at more affordable interest rates.
A higher level of financial reserves and investment income in relation to existing debt obligations also increases an organization’s debt capacity, creating an important safety valve if an organization has to borrow money to mitigate poor operating or investment performance.
Not-for-profit hospitals and health systems rely on three interdependent functions to contribute to the financial resilience of the organization: namely, the ability to withstand adverse changes to these core functions and continue to provide services to the community (Figure above).
The Operating Function:
The Operating Function manages the portfolio of clinical services and strategic initiatives that define the charitable mission of the organization. Clinical services generate patient revenue, and if that revenue creates a positive margin (i.e., exceeds expenses), that excess is invested back into the health system. Operating margins are, on average, very low in not-for-profit healthcare. For example, for the not-for-profit hospitals and health systems rated by Moody’s Investors Service, median operating margins from 2017–2021 ranged between 2.1% and 2.9%. These rated organizations represent only a few hundred of the thousands of hospitals and health systems in the country and are among the most financially healthy. A 2018 study of a wider group of more than 2,800 hospitals found an average clinical operating margin of -2.7%.
The Finance Function:
Because the positive margins generated by the Operating Function are rarely enough to support the intensive capital needs of maintaining and improving acute-care facilities, care delivery models, and technology, not-for-profit health systems rely on the Finance Function for internal and external capital formation. The Finance Function builds cash reserves and secures external financing
(e.g., bond proceeds, bank lines of credit) to support the capital spending needs of the organization. The cash reserves maintained by the Finance Function also help the organization meet daily expenses at times when expenses exceed revenues.
The Investment Function:
Not-for-profit hospitals and health systems will also endeavor to invest some of their cash reserves to generate returns that, first, act as an additional hedge against potential risks that could disrupt operations or cash flow, and second, pursue independent returns. Any independent returns generated serve as an important supplement to revenues generated through the Operating Function.
The three functions described above are common to all not-for-profit organizations. The main differences are mostly within the Operating Function. In higher education, for example, tuition revenue takes the place of clinical revenue. While higher education also maintains enterprise risk, the Operating Function for colleges and universities is less vulnerable to volume swings as enrollment is typically steady and predictable. Likewise, higher education is less labor intensive than healthcare.
Financial reserves include all liquid cash resources and unrestricted investments held in the Finance and Investment Functions. These reserves are equivalent to the emergency funds individuals are encouraged to maintain to help them meet living expenses for six to twelve months in case of a job loss or other disruption to income.
Absolute reserve levels are important, as discussed above, but they must also be viewed relative to a hospital’s daily operating expenses. A common
metric used to describe these reserves is Days Cash on Hand. If an organization has 250 Days Cash on Hand, that means that it would be able to meet its operating expenses for 250 days if revenue was suddenly shut off. The size of Days Cash on Hand will be proportionate to the size of the hospital and health system. Some of the largest not-for-profit health systems have annual operating expenses approaching $30 billion annually: meeting those expenses for 250 days would require Days Cash on Hand of more than $20 billion.
The shutdown that occurred in the early days of the pandemic (March through May 2020) is an example of a time when cash flow nearly shut off for most hospitals (except for emergency care). Reserves, measured in absolute and relative terms such as Days Cash on Hand, allowed hospitals that were nearly empty to maintain staffing and operations throughout the period. Other hospitals that were inundated with patients during the initial surge were able to fund increased staffing and personal protective equipment costs through their reserves. Other examples of how reserves provide a buffer
against unexpected events include natural disasters such as hurricanes, tornadoes, deep freezes, and wildfires, which can require the temporary shutdown of operations; cyberattacks, which can halt a hospital’s ability to provide services; a defunct payer that is unable to reimburse hospitals for care already provided; or an escalation in labor costs as experienced by many during 2022.
Without the reserves to pay for contract labor or premium pay, many hospitals would have undoubtedly had to close or limit services to their community.
KEY TAKEAWAYS
Financial reserves are created through the interdependent relationship of operating, finance, and investment functions in not-for-profit health systems.
These reserves build financial resilience: the ability to withstand adverse changes to core functions and continue to provide services to the community.
Financial reserves play an important role in supplementing any shortfalls in revenue or capital formation in one or more of these three functions.
Financial reserves are equivalent to individual emergency funds—both are intended to cover expenses if income or revenue flows are significantly disrupted.
A common metric used to describe financial reserves is Days Cash on Hand: an organization’s combined liquid, unrestricted cash resources and investments, measured by how many days these reserves could cover operating expenses if cash flows were suddenly shut off.
Financial reserves, measured in absolute and relative terms such as Days Cash on Hand, allowed hospitals that were nearly empty during the early days of the pandemic to maintain staffing and operations throughout the period. Other hospitals that were inundated with patients during the initial surge were able to fund increased staffing and personal protective equipment costs through their reserves.
A Comparison: Financial Reserves and Higher Education Not-for-Profits
Not-for-profit hospitals and health systems are not alone in their reliance on financial reserves; most not-for-profit organizations carry reserves that enable them to maintain operations and make needed investments even in times of weaker operating performance. Higher education is probably most comparable to healthcare, with significant overlaps between the two sectors. Moody’s Investors Service, one of the three major rating agencies, notes that 16% of its rated higher education institutions have affiliated academic medical centers (AMCs), and revenue from patient care at these AMCs contributes to 28% of the overall revenues for the higher education sector.
The magnitude of Days Cash on Hand levels varies by industry; financial reserves maintained by private not-for-profit higher education
institutions, for example, are significantly greater than those maintained by not-for-profit hospitals and health systems. For comprehensive private universities across all rating categories, Moody’s reports median Days Cash on Hand in 2021 of 498 days for assets that could be liquidated within a year. This compares with a median 265 Days Cash on Hand in 2021 across all freestanding hospitals, single-state, and multi-state healthcare systems rated by Moody’s.
Financial reserves are a critical measure of financial health across both healthcare and higher education. They help ensure that not-for-profit colleges, universities, hospitals, and health systems can continue to fulfill their vital societal functions when operations are disrupted, or when they are experiencing a period of sustained financial distress.