When COVID volumes waned in the spring and early summer, most health systems “de-escalated” dedicated COVID testing and triage facilities. But with the Delta variant surging across the country, consumers are now once again looking for services like drive-through testing, which is perceived as more convenient and safer.
One physician leader told us patients in the ED are asking why the hospital got rid of the “COVID tent”, which provided a separate pathway for patients with respiratory and other COVID symptoms—and a highly visible signal that the rest of the department was as COVID-free as possible.
Another system is now fielding questions from the media about whether they’ll bring back their dedicated COVID hospital: “We spent a lot of time last year convincing the community that the dedicated hospital was key to safely managing care during the pandemic. Now we’ve got almost as many COVID admissions spread across our hospitals.”
Over the past year, providers have learned how to safely manage COVID care and prevent spread in healthcare settings—but consumers may perceive the lack of dedicated facilities as a decline in safety.
Unlike last year, hospitals are full of non-COVID patients, as those who delayed care reemerge. And with the current surge likely to continue into flu season, emergency rooms will only get more crowded, necessitating a new round of communication describing how hospitals are keeping patients safe, and reassuring patients that healthcare settings remain one of the safest places to visit in the community.
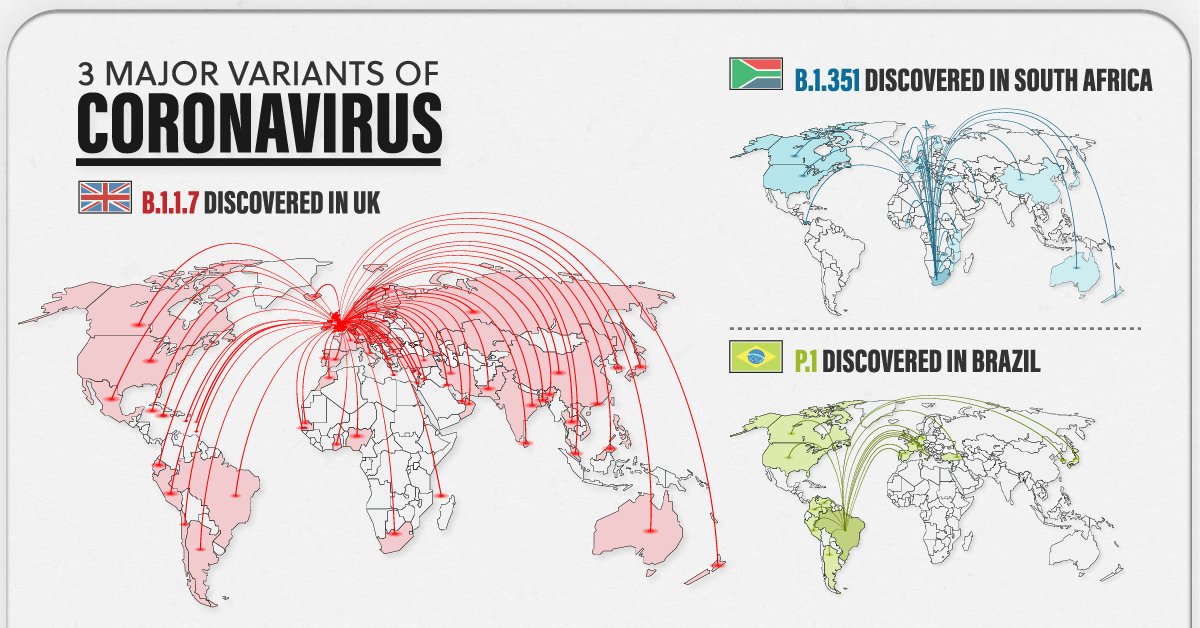
As billions of people gear up for widespread vaccination against COVID-19, another issue has reared its head. Three major COVID-19 variants have emerged across the globe—and preliminary research suggests these variants may be cause for concern.
But what makes them different from the original strain?
The following visualizations answer some key questions, including when these variants were first discovered, how far they’ve spread worldwide, and most importantly, their potential impact on the population.
Some Context: What is a Variant?
Before diving in, it’s important to understand why viruses mutate in the first place.
To infect someone, a virus takes over a host cell and uses it to replicate itself. But nature isn’t perfect, and sometimes, mistakes are made during the replication process—those mistakes are called mutations.
A virus with one or more mutations is referred to as a variant. Most of the time, variants do not affect a virus’s physical structure, and in those instances, they eventually disappear. However, there are certain cases when a mutation impacts part of a virus’s genetic makeup that does change its behavior.
According to the U.S. Centers for Disease Control (CDC) a change in behavior can alter:
Rate of transmission
Deadliness
Ability to potentially infect someone with natural or vaccine-induced immunity
Preliminary research has detected some of these changes in the three major COVID-19 variants—B.1.1.7, B.1.351, and P.1.
The 3 Major COVID-19 Variants
The three major variants emerged at different times, and in different parts of the world. Here’s an overview of each variant, when they were discovered, and how far they’ve spread so far.
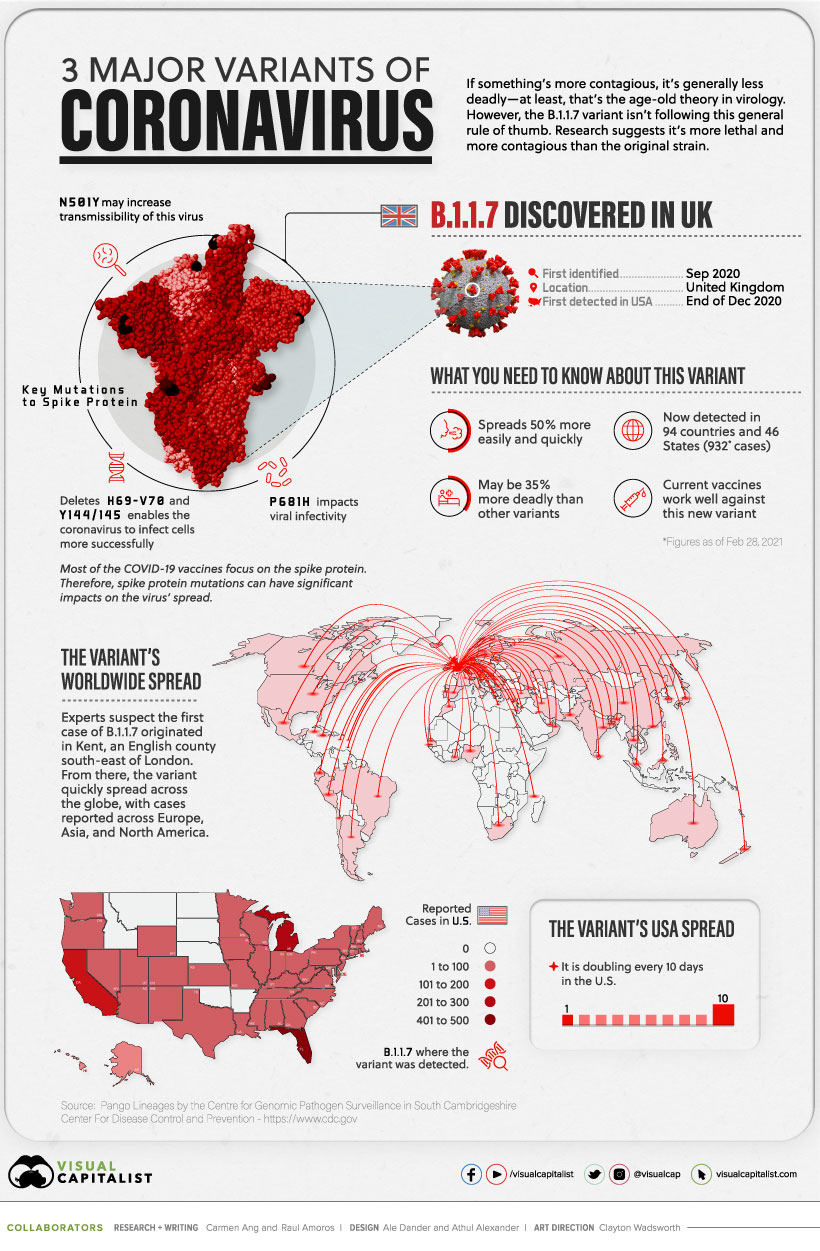
B.1.1.7
The B.1.1.7 variant was detected in the UK in the fall of 2020. By December 2020, it had spread across the globe, with cases emerging across Europe, North America, and Asia.
Currently, the variant has been reported in roughly 94 countries.
Early research suggests it’s 50% more transmissible than other variants, and potentially 35% more deadly than the standard virus. Luckily, studies suggest that some of the existing vaccines work well against it.
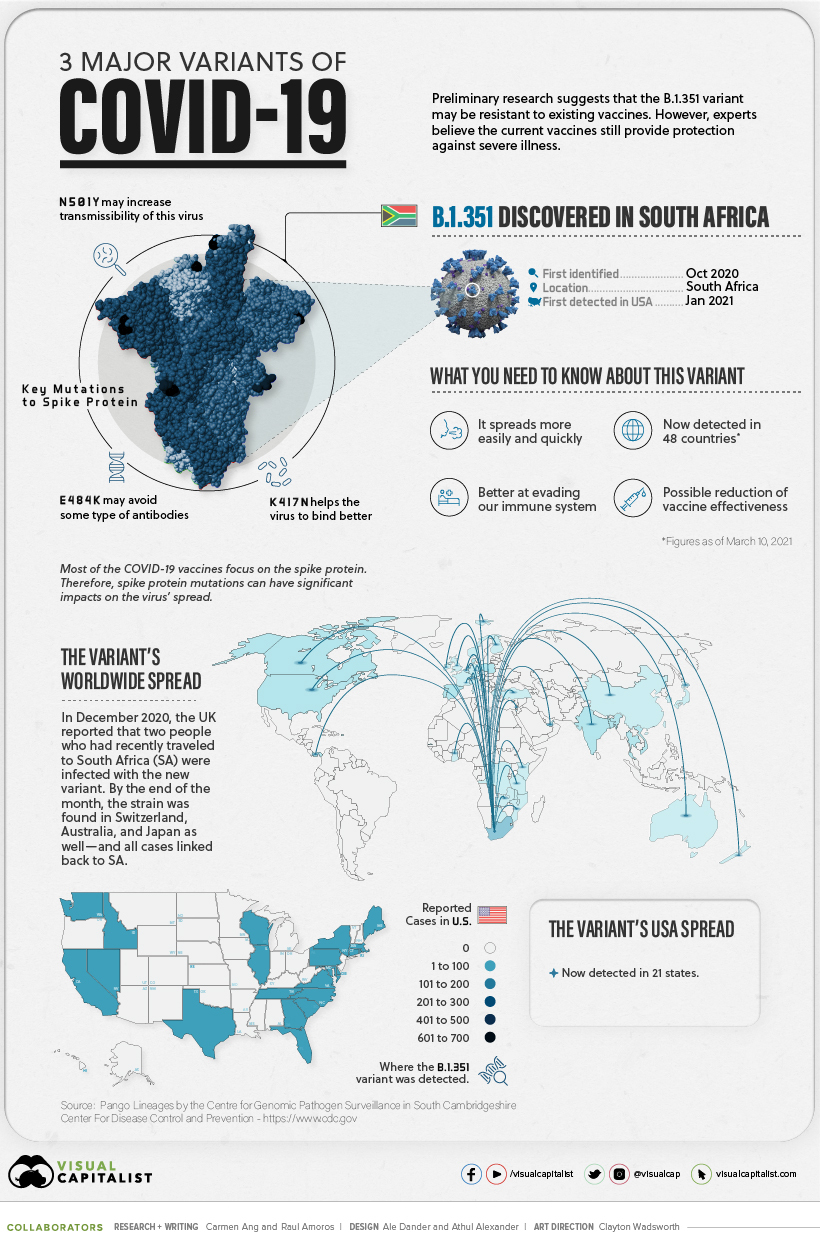
B.1.351
In October 2020, the second major variant was discovered—B.1.351. It was first identified in South Africa, but by end of the year, it had spread to the UK, Switzerland, Australia, and Japan.
There are approximately 48 countries with reported cases, and research suggests several of the existing COVID-19 vaccines may not be as effective against this variant.
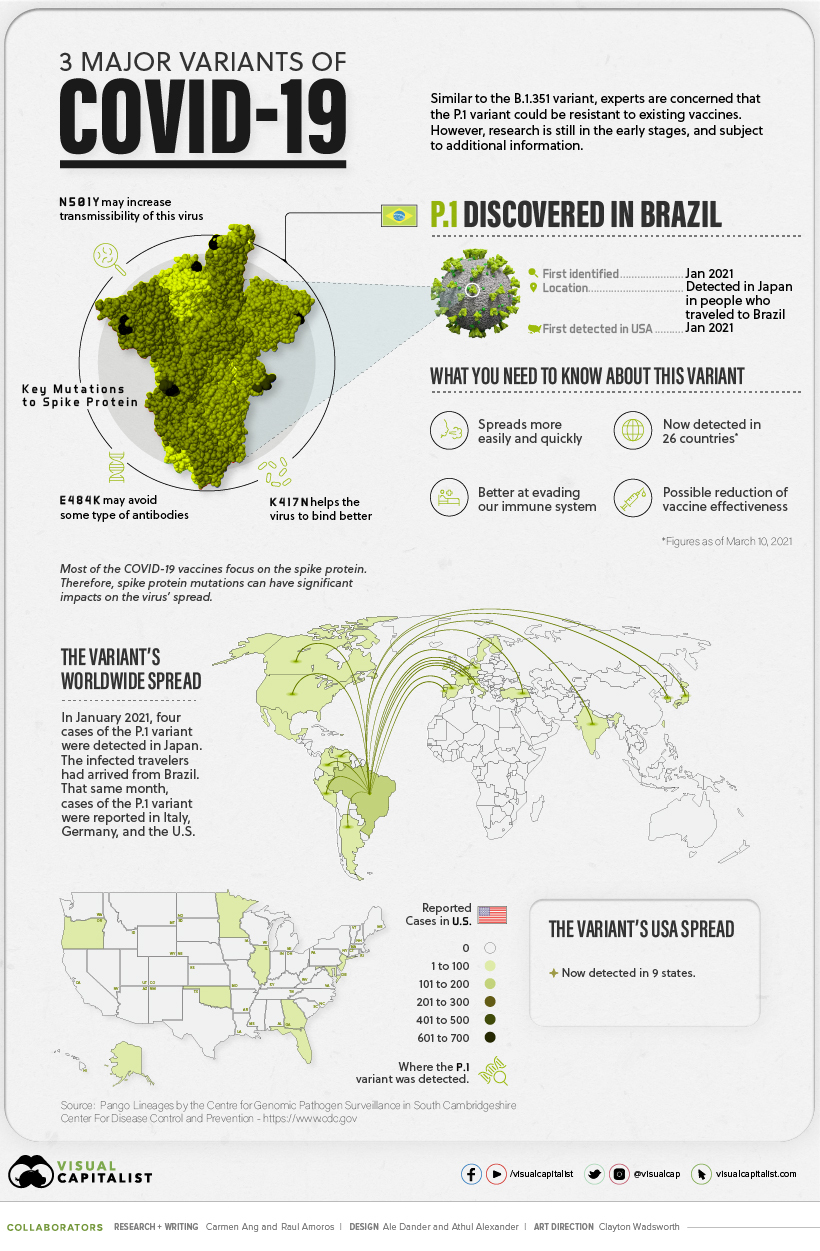
P.1
The P.1 variant was the last to arrive on the scene.
It was first discovered in January 2021, when Japan reported four cases of the variant, which was found in travelers who had arrived from Brazil.
Approximately 25 countries have reported cases of the P.1 variant, and early research suggests this variant is not only more contagious, but could also have the ability to infect people with natural immunity who had already recovered from the original strain.
Still Early Days
While there have been preliminary studies showing a dip in vaccine effectiveness, some experts emphasize that it’s too early to tell for certain. More data is needed to gain a deeper and more accurate understanding.
In the meantime, experts are emphasizing the importance of following our current public health strategies, which include physical distancing, vaccination, washing your hands, and using masks.
Oh, how the tide has turned. Three months ago, COVID was ravaging my homeland, India. The Delta variant was burning through the country like an uncontrolled wildfire. People carted dying relatives town to town, desperately seeking hospital beds or a whiff of oxygen. A cousin in India said, “COVID is not taking lives, just the beds. Lack of oxygen is taking lives.”
I watched India’s suffering unfold and felt guilty for living in one of the world’s most resourceful and scientifically advanced countries. My homeland was floundering, but at least my other homeland — the U.S. — was finally on track.
104 million Americans had been vaccinated. The Pfizer vaccine alleviated the worst outcomes of the B.1.1.7 and B.1351 variants. Adolescents aged 12-15 were gearing up for vaccine eligibility within days, and the CDC was reporting the U.S. could see a sharp decline in COVID cases by July if nationwide vaccinations continued. Health care workers had proper PPE, millions of people were getting vaccinated each week, and infection rates were declining steadily. We could finally see Spring’s light at the end of the year’s tortuous dark tunnel. Our country was in the home stretch.
Now the Delta variant is here and I have to wonder, Who were we kidding? We don’t live in a world where vertical borders prevent airborne particles from crossing time zones. Planes and boats carry viruses from one country to the next like microscopic stowaways. The virus doesn’t abandon ship. It mutates, and adapts, and colonizes.
We had a real chance to strangle this monster, to show the rest of the world how it was done, to help them all in the process. We let that chance slip away. Not everyone and not everywhere, but enough people got complacent. Some waited for herd immunity to carry the load—a number that crept from 60 to 70 to 85 percent, depending on what you read and when you read it—and others just figured it would pass. Now the Delta variant, the same one that tore through India and Great Britain, has twisted out of our flimsy grip and is roaring with laughter.
How did this happen?
Misinformation. Political discord. Vaccine hesitancy. The bottom line is our vaccination rate faltered. The CDC reported that on August 1, 2021, approximately 400,000 Americans received their first COVID dose. While that seems high, it’s less than a quarter of the peak in mid-April. We haven’t maxed out eligible people (only 58.1 percent of eligible people were fully vaccinated as of a week ago). We’re maxing out the number of people who know COVID’s real repercussions are far worse than the vaccine’s feared ones.
The U.S now has the third-highest rate of vaccine skepticism among 15 of the world’s largest economies. Our vaccine surplus is so large the FDA extended Johnson & Johnson’s vaccine expiration dates to avoid throwing out perfectly good doses. Less than a week ago, President Biden announced the U.S. has donated and shipped more than 110 million doses to 60 countries. While I applaud the humanitarian effort, I question the fate of those doses if the 41.9 percent unvaccinated eligible people in our country had wanted them.
It makes me wonder: Why does science take a backseat to unsubstantiated pseudoscientific claims?
Spreaders of vaccine disinformation fill their social media accounts with statements questioning COVID’s existence and purporting unproven treatments (never mind the fact that we wouldn’t need treatments if COVID didn’t exist) with little to no peer-reviewed scientific research to support their anti-vaccine claims. According to Imran Ahmed, CEO of the Center for Countering Digital Hate, twelve people — the “disinformation dozen” — produce 65 percent of the shares of anti-vaccine misinformation on social media platforms.”
Is it easier for some to believe that a science-backed treatment is inherently more dangerous than an unknown herb plucked from a field? Perhaps. But what do they say to the approximately 216 kids hospitalized daily in the U.S. over the past week, particularly in areas where vaccine coverage is low? Bad luck? You weren’t strong enough? What would have made them stronger?
Yes, there are measures underway to increase vaccinations—full FDA approval, social media crackdowns on misinformation, and government, company, military, and college mandates. But let’s be honest, many Americans are fighting these measures, as they will fight future mandates, and the next vaccine.
Only two things can change how non-vaxxers perceive COVID vaccines: education and trust. We need to sincerely hear their reasons, and then gently clarify misinformation—vaccines don’t introduce disease into our bodies. They stimulate our immune systems to obtain immunity without getting the disease. Vaccines don’t alter our DNA. Their safety has been tested. Medicines have potential side effects, but illnesses have definite ones. COVID kills indiscriminately; vaccines don’t.
Trust is harder. How can we help people trust these vaccines? I suppose on a deeper level, it’s more about trusting the people that make the vaccines. Big pharma, for-profit companies—sure, they are the money makers. But behind the scenes, the vaccines are created by men and women who’ve accepted the charge to make this world—not just individuals—safer and healthier. They’ve spent years studying, researching, and testing potential vaccines with dedication and patience, including the mRNA technology in COVID vaccines. Just because the COVID vaccine’s rollout was fast-tracked to combat the pandemic doesn’t mean the scientists cut corners in designing and testing it.
Unfortunately, we don’t have the luxury of slowly educating and gradually building trust. COVID is terrorizing our planet now. The world is shaking its heads at the U.S., wondering what happened. We were supposed to be the leader. This morning, an aunt in a small town in India sent me a WhatsApp message: “I have taken the vaccine … the positivity rate has gone down … I am worried for America … how r u?” I don’t know. America, how are we? It’s not too late to destroy this monster, but if the unvaccinated remain unmoved, it will be soon.
As Israel faces a surge in Covid-19 cases due to the delta variant, data from the Israeli Health Ministry shows that a third dose of Pfizer-BioNTech’s Covid-19 vaccine significantly improved protection against hospitalization or serious disease.
Background
The rollout of Covid-19 vaccines in Israel was one of the fastest and most comprehensive in the world. By March 25, more than half of Israel’s population was fully vaccinated, and by June, the country had lifted all coronavirus-related restrictions.
However, in the summer, Israel saw a surge in Covid-19 cases, which experts believe was fueled by two factors: waning protection from the vaccine and the spread of the highly contagious delta variant.
“The most influential event was so many people who went abroad in the summer—vacations—and brought the delta variant very, very quickly to Israel,” Siegal Sadetzki, a former public health director in Israel, said.
Even so, the rate of severe Covid-19 cases among the vaccinated remains low. As of Thursday, according to data from the Health Ministry, the rate of severe Covid-19 cases was nine times higher among unvaccinated people over the age of 60 than among vaccinated people in the same age range.
Similarly, the rate of severe Covid-19 cases among unvaccinated people under 60 was about twice the rate of severe cases among vaccinated people under 60.
But because so many people in the country have been vaccinated, even a low rate of severe breakthrough infections has led to a significant surge in hospitalizations. NPR reports that half of the seriously ill patients in Israel hospitalized with Covid-19 had been fully vaccinated at least five months ago, and the majority of them are over the age of 60 with comorbidities.
Data shows booster shots provide significantly increased protection
On July 30, Israel began administering booster shots of the Pfizer-BioNTech vaccine to those over the age of 60. On Thursday, the country dropped that age eligibility to 40.
Data from the Health Ministry indicate that a third dose of the Pfizer-BioNTech vaccine provided four times the protection against infection as two doses in people aged 60 and over, Reuters reports. (According to Reuters and NPR, the findings are similar to data released by Israel’s HMO Maccabi Healthcare Services last week, which found that among 149,144 people, a third Pfizer shot among recipients above age 60 reduced the odds of infections by 86% and cut the risk of severe infection by 92%.)
Similarly, a third dose offered about five to six times the protection of two doses against serious illness and hospitalization in people aged 60 and over, according to the Health Ministry data.
According to Reuters, the data underlying these figures was presented at a health ministry panel meeting on Thursday and later published on the ministry’s website. Full details of the study, however, still have not been released.
The debate over booster shots continues
The news comes as experts in the United States continue their debate over the necessity of booster shots. On Wednesday, the Biden administration announced that Americans who had received an mRNA vaccine would be able to get a booster shot beginning in September, pending approval by FDA and a recommendation by CDC.
However, health experts are divided on whether booster shots are necessary, a debate that prompted CDC’s Advisory Committee for Immunization Practices (ACIP) to push back its meeting to discuss booster shots by one week, Bloomberg reports.
“The data [is] coming in rapidly, and we want to make sure we follow our process for review and to ensure we can have a robust deliberation at the next open meeting,” Grace Lee, chair of ACIP, said.
Joshua Barocas, associate professor of medicine at the University of Colorado, said he believes the “federal government is simply trying to stay ahead of the curve.” However, Barocas said, “I have not seen robust data yet to suggest that it is better to boost Americans who have gotten two vaccines than invest resources and time in getting unvaccinated people across the world vaccinated.”
The World Health Organization has also called for wealthier countries to not offer booster shots to their population and instead help poorer countries get vaccinated.
Surgeon General Vivek Murthy said the United States’ efforts to provide boosters to its population won’t interfere with efforts to provide other countries with shots.
“We have to protect American lives and we have to help vaccinate the world, because that is the only way this pandemic ends,” Murthy said.
He did acknowledge that providing booster shots to Americans could “take away” from the supply of vaccines for the rest of the world, but added that the United States has been working to improve the global vaccine supply and production recently to make sure that doesn’t happen.
“We don’t have a choice,” Murthy said. “We have to do both.”
As some states set Covid-19 hospitalization records, many overwhelmed hospitals are outsourcing patients on planes, helicopters, and ambulances to distant cities and states for treatment, Heather Hollingsworth and Jim Salter write for the Associated Press.
Transfers hundreds of miles away
As of last week, the number of Covid-19 patients in most hospitals remained below winter surge levels, Hollingsworth and Salter report. However, Florida, Arkansas, Oregon, Hawaii, Louisiana, and Mississippi recently set pandemic hospitalization records.
And unlike in the winter surge, many hospitals were already strained this summer due to patients catching up on previously deferred care, according to Hollingsworth and Salter.
“We are seeing Covid patients and we are seeing car accidents and we are seeing kids come in with normal seasonal viral infections. And we are seeing normal life come into the emergency department along with the extra surge of Covid patients, so it is causing that crisis,” said Mark Rosenberg, president of the American College of Emergency Physicians.
Amid the influx of patients, many of these overwhelmed hospitals are looking to neighboring cities and states for relief. For instance, in Arizona, a Covid-19 hotline is receiving calls from hospitals in Wyoming, Arkansas, Texas, and California in search of bed space, Hollingsworth and Salter report—although the hotline often cannot provide any help.
In Kansas, officials at the Wilson Medical Center in Kansas had to call 40 other facilities in several states seeking a bed for a Covid-19 patient before finally finding an available bed about 220 miles away. Across the state, according to Motient, a company contracting with Kansas to manage transfers, Covid-19 patients generally have to wait an average of 10 hours before being flown to another hospital location, which could be in Wisconsin, Illinois, Colorado, or Texas. “That is just the worst day that you can have in the emergency room as a provider,” Richard Watson, Motient’s founder, said, “to be taking care of a patient that you are totally helpless to give them what you know they need.”
Similarly, in Washington state, the 25-bed Prosser Memorial Hospital, doesn’t have an intensive care unit, so critically ill patients are being sent as far as eastern Idaho—600 miles away.
Staffing shortages, low vaccination rates add to the problem
Finding a hospital to take in patients has become more difficult due to recent staffing shortages, according to Robin Allaman, CNO at the Kearny County Hospital in Kansas.
“Most [hospitals] are saying it isn’t that they don’t have an open bed, it is that they don’t have nursing staff to care for them,” he said. Officials at his hospital called health systems in Nebraska, Oklahoma, and New Mexico before one in Colorado Springs, Colo.—200 miles away—agreed to take a recent patient.
Watson said these delayed transfers can have dire consequences for patients, especially those who need to see specialists, who often are available only in larger hospitals. “Imagine being with your grandma in the ER who is having a heart attack in western Kansas and you are saying, ‘Why can’t we find a bed for her?’ We are watching this happen right in front of us. ‘This is America. Why don’t we have hospital bed for her?’ Well, here we are,” he said.
And while experts had hoped that the vaccines would prevent hospitals from becoming overwhelmed again, Justin Lessler, a professor of epidemiology at Johns Hopkins University, said there hasn’t been the reduction in hospitalizations that officials had hoped for. That’s in part because the delta variant seems to be more severe, particularly in younger people, whose vaccination rates are lower.
Steve Edwards—CEO of CoxHealth, whose hospital in Springfield, Mo., is treating patients from as far away as Alabama—added, “Just imagine not having the support of your family near, to have that kind of anxiety if you have someone grow acutely ill.”
About 8,000 Marshfield (Wis.) Clinic Health System employees have requested black ID badge reels to indicate they are fully vaccinated, the health system told Becker’s Aug. 11.
The nine-hospital health system, which has more than 12,000 employees, started offering the black reels in July. Many Marshfield employees are already required to wear white reels. However, the new black reels are voluntary. Employees who have them may meet in person, but must be masked, if all meeting attendees are vaccinated, the health system said.
“We all look forward to having the opportunity to interact with co-workers outside of the virtual world,” said health system spokesperson Jeff Starck. “The badge reels are a way for more personal interaction and create a sense of normalcy for many employees during what has been a challenging, mostly virtual work environment. The reaction has been overwhelmingly positive.”
Mr. Starck said that some employees may not have not asked for the new reels because they use clips or other devices to display their name badges. Employees who work off-site and don’t attend in-person meetings may not have requested them since they haven’t needed them, and some employees who are vaccinated simply may not want to identify themselves, he speculated.
Marshfield Clinic announced Aug. 4 that it would require employees to become fully vaccinated for COVID-19 by Nov. 15.
As of Aug. 11, about 72 percent of employees are vaccinated, although the health system said that number will rise as it receives proof of vaccination from employees who were inoculated outside the health system.



:no_upscale()/cdn.vox-cdn.com/uploads/chorus_image/image/69062792/icm_fullxfull.336535675_95ew78665csgwwwo8wo4.0.jpg)
