https://www.kaufmanhall.com/insights/thoughts-ken-kaufman/misadventures-primary-care

Innovation in the American economy over the past 30 years has been nothing short of stunning—one remarkable technological advance after another. Industry by industry and product by product, corporate innovation has profoundly changed the way we navigate our economic and consumer lives. From this context of technological and innovative change came the corporate belief that healthcare could be “significantly improved” through the same application of aggressive corporate strategy and innovation.
So along came Walmart, Walgreens, CVS, and Amazon with all the resources in the world and with the best intentions to contemporize primary care.
The goals of all this were front and center: change the definition of the healthcare gatekeeper, lower costs, improve quality, and create a much more consumer-friendly care experience. Yet here we see that American business has proven—once again—that the best intentions, the smartest ideas, and a lot of money are still no guarantee of commercial success. How quickly the corporate retail re-invention of primary care all came apart.
Between 2017 and 2022, retail clinic claims grew 200%, spiking particularly during the pandemic, according to Healthcare Finance. And yet now, Walmart has abandoned its primary care strategy, Walgreens is pulling back significantly—even after announcing significant expansion plans as little as a year ago—and CVS is facing uncertainty after a leadership shakeup.
Under corporate leadership and strategy, primary care has become a catalog of woes. Let’s unpack that catalog.
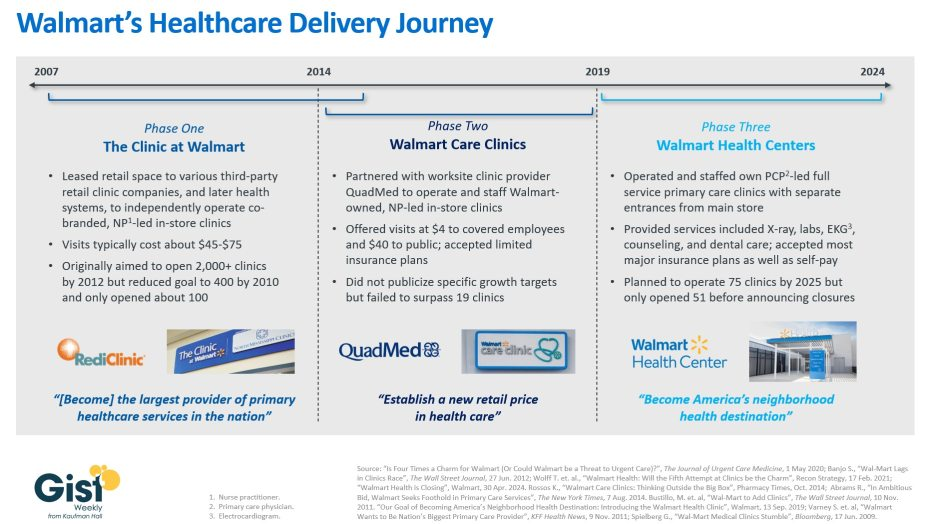
Walmart opened its first health center in 2019, offering a range of basic services with prices posted. At first, it focused on patients who could pay cash, but eventually evolved to accept a range of insurance plans. Walmart brought a level of strategic aggression to its primary care initiative by announcing in 2023 it would nearly double the number of clinics it operated. But in an abrupt about face, the megaretailer shuttered all 51 primary care locations in April, citing an unsustainable business model with an inability to maximize revenue and adequately control expenses.
Walgreens, on the other hand, opted to invest in existing providers. In 2020 and 2021, Walgreens spent $6.2 billion on the primary care clinic chain VillageMD, establishing it as the majority owner. In 2022, Walgreens sunk another $3.5 billion, through a mix of debt and equity, into VillageMD’s $8.9 billion acquisition of Summit Health. Walgreens, like Walmart, suffered for its primary care investments. The company was forced to take a $5.8 billion write-down on Village MD in the second quarter of this year.
During an October 15 earnings call, Walgreens CEO Tim Wentworth said the company “is reorienting to its legacy strength as a retail pharmacy-led company,” according to the Wall Street Journal. “We are in the early stages of a turnaround that will take time.” And that comment came with the potential closure of 1,200 Walgreens retail locations, following on the heels of 160 primary care clinic closures earlier this year.
CVS, too, has not been immune to primary care turbulence, as CVS Health CEO Karen Lynch was forced to step down last month after presiding over an expansion of healthcare clinics but then closing dozens of them in California and New England. CVS’s strategic approach revolved around its $10.6 billion acquisition of Oak Street Health in 2023 and its intention to expand primary care in 1,100 MinuteClinics. That strategy now seems to be up in the air with the departure of Ms. Lynch. The CVS board is now suggesting an approach that may involve a spinoff of its insurance and pharmacy benefits manager units, Aetna and Caremark.
Amazon, however, at the moment shows no signs of abandoning its foray into primary care. Rather than focusing its efforts on solely brick-and-mortar locations, Amazon organized its primary care strategy around the 2023 $3.9 billion acquisition of One Medical, a concierge-style service designed to facilitate both in-person and virtual visits. While Amazon’s primary care strategy remains somewhat opaque, it seems to revolve around partnering with employers and health systems to cultivate primary care patient loyalty through a membership program that builds on the Amazon Prime brand.
Each company took a slightly different approach to primary care, but all four planned to leverage their exceptional size to achieve profitability.
Interestingly, scale has not been sufficient to solve the challenges of primary care. American Medical Association President Bruce A. Scott wrote recently: “If retail giants can’t make today’s care delivery model work financially, how on earth can physicians in private practice?” It’s no wonder the ongoing shortage of about 20,000 primary care physicians is expected to persist. A recent AAMC report found that by 2036, that number could double.
Primary care has been unsuccessful as a transactional business; retailers sell goods at a set price and send customers on their way. In healthcare, payment models are nowhere near as straightforward. Patients, particularly in areas where access to care is limited, may have continuous, rather than episodic, needs. All of this complexity has seemed to add up to higher costs and lower margins. Primary care seems to require a much more complex business model, one robust enough to remain patient as that business model experiments with various approaches or is vast enough to offset losses with other lines of revenue.
So where does all of the above lead us? Are there any useful conclusions or lessons to be learned? Maybe so.
- Primary care is an essential component of any hospital system of care. Done right, it acts as both an important gatekeeper and as a trusting component of the continuity of healthcare service.
- At the moment, there is not enough primary care to meet the demand. Stories abound of patients whose longtime primary care physicians retire and said physicians cannot be replaced without a great effort—or often not at all.
- Right now, the economics of primary care don’t work as a standalone service. Many have tried and—regardless of whether they were big or small, for profit or not-for-profit—this essential patient-centered service can only operate when subsidized by a larger enterprise. Walmart, Walgreens, and CVS have all tired of those subsidies.
- The overall healthcare system and its quality of care and delivery is significantly damaged by the current state of primary care. Too many patients receive delayed diagnosis and treatment and slow or little necessary follow-up. Patients that should be seen in the office are instead funneled to the emergency room. Care, of course, remains well-intentioned but often is instead inconsistent and chaotic. Conditions that might have been deftly managed instead become chronic.
- All this leads to the importance of not giving up on primary care. Patients prefer to be seen in the primary care ecosystem. They tend to trust that level of care and attention. Patients also prefer to be seen in-person when they are feeling particularly poorly, and they appreciate prompt answers about concerning health issues. What this all suggests is that we are at a moment when hospitals need to double down on the primary care dilemma. Primary care needs to be examined as an essential component of the overall enterprise-wide strategic plan both clinically and—especially—financially.
Corporate America, with all of its economic power and resources and scale, has found primary care to be a confounding and, so far, unsuccessful business model. So, after all of the recent noise and promises and slide decks, the problem and promise of primary care is back in the mission-driven hands of America’s not-for-profit hospitals—exactly where it should have been all along.