



Despite all the time, money, and energy spent on improving healthcare quality and value, there is no “overarching concept” or consistent definition of what constitutes a “high-performing health system,” a review by The Joint Commission has found.
“The absence of a consistent definition of what constitutes high performance and how to measure it hinders our ability to compare and reward health care delivery systems on performance, underscoring the need to develop a consistent definition of high performance,” the review found.
In their search for a consistent definition of the term, The Joint Commission researchers sifted through English-language articles defining high performance with respect to a healthcare system or organization in PubMed and WorldCat databases from 2005 to 2015 and the New York Academy of Medicine Grey Literature Report from 1999 to 2016. The entity/condition to which the definition was applied was extracted from included articles.
The number and type of dimensions used to define high performance within and across articles was tabulated and the number and type of metrics used by performance dimension and by article was calculated.
Instead of a consistent definition, the researchers found that high performance was variably defined across different dimensions, including quality (93% of articles), cost (67%), access (35%), equity (26%), patient experience (21%), and patient safety (18%).
Most articles used more than one dimension to define high performance (75%), but only five used five or more dimensions. The most commonly paired dimensions were quality and cost (63%).
The Joint Commission researchers said in their review that measuring performance in the nation’s healthcare delivery system “has gained significant traction” over the years with policy makers, even though they apparently do not have a consistent definition of the term.
To support delivery system improvement nationally, the Agency for Healthcare Research and Quality recently funded three Centers of Excellence to study high-performing systems, particularly their ability to quickly move new evidence-based care practices into practice, The Joint Commission review noted.
“Research to understand what enables healthcare delivery systems to perform highly, and policy efforts to measure and recognize high-performing health care delivery systems, is predicated on an agreed-on definition of what it means to be high-performing,” the researchers said.
“Achieving consensus on what it means to be high-performing is essential to facilitate comparisons across delivery systems and in applied measurement activities, such as programs that designate and publicly recognize high performers.”

Like everything in health care, network adequacy is complicated, with numerous measures and differing regulations by program. This post offers a flavor and a bit of organization of that complexity, based on some of our recent reading.
Medicare Advantage
When is network adequacy assessed? CMS is only certain to assess a plan’s network upon application for a new contract or expansion of a contract’s service area. At its discretion, CMS may review networks at other times, for instance when a plan terminates a contract with a provider, when it changes ownership, or when there are network access complaints or plan-identified network deficiencies.
What types of entities are assessed for adequacy? There are different network adequacy standards for each of 27 practitioner specialty types (e.g., primary care, cardiology, urology) and 23 facility types (e.g., acute inpatient hospitals, outpatient dialysis, mammography).
Are all markets treated equivalently? No. CMS places each county into one of five categories: Large Metro, Metro, Micro, Rural, or CEAC (Counties with Extreme Access Considerations). Within each practitioner and facility type, there are different network adequacy standards by county type. These can change from year-to-year as well.
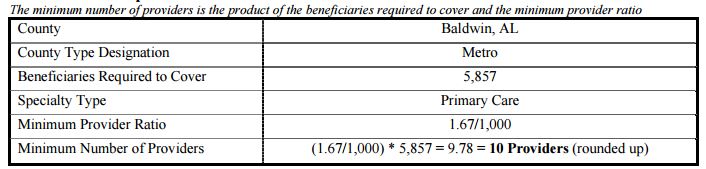
How is network adequacy measured? The gist is that each plan must contract with a specified number of providers of each type. Moreover, 90% of beneficiaries in the county must live within specified travel distance and travel time from at least one provider of each type. To calculate the minimum number of providers, each county receives a population of beneficiaries (termed “beneficiaries required to cover” in the table below) that is equal to the 95th percentile of penetration in all plans in its county type, multiplied by the total number of beneficiaries in the county. That’s a mouthful, but roughly speaking it means that CMS makes sure that each plan can serve a number of beneficiaries larger than it is ever likely to enroll.
This is rather abstract. How about a concrete example? Sure! The following tables should help. The first illustrates the calculation of the number of primary care providers a plan in Baldwin, AL must contract with (10) for 5,857 beneficiaries.
The next table shows that in Baldwin, AL, at least one primary care provider must be within 10 miles and 15 minutes of travel time for 90% of beneficiaries in the county. Additionally, a PCP who is not within the time and distance requirements of at least one beneficiary, will not count towards the minimum number of providers required. Moreover, because at least 90% of beneficiaries must be within the time and distance requirements, a plan may have to contract with more than the minimum number of providers required to meet these requirements.

Where can I learn more? Here are some potentially helpful links:
Marketplaces
The following is for federally facilitated marketplaces, but concludes with a comment about state facilitated ones.
When is network adequacy assessed? As best we can tell, network adequacy is assessed for each plan every year.
What types of entities are assessed for adequacy? CMS focuses on a subset of specialist areas and facility types that have been associated with network adequacy problems in the past: hospital systems, dental providers (if applicable), endocrinology, infectious disease, mental health, oncology, outpatient dialysis, primary care, and rheumatology. That other specialists and facility types are not necessarily scrutinized is one limitation of the approach.
Are all markets treated equivalently? No. CMS places each county into the same categories used for MA plans’ network adequacy: Large Metro, Metro, Micro, Rural, or CEAC (Counties with Extreme Access Considerations). Within each practitioner and facility type, there are different network adequacy standards by county type. Presumably, these can change from year-to-year as well.
How is network adequacy measured? The approach is similar to that for MA plans: 90% of enrollees must have access to at least one provider/facility type within specified travel distances and travel times. A key difference is that there does not appear to be a minimum number of each provider type every plan must contract with. It’s reasonable to hypothesize, therefore, that marketplace plans would have much more narrow networks than MA plans, but no direct comparison exists, to our knowledge.
Public Health Care Programs: Lower Cost but Not Lower Quality
In recent days, Democrats have stepped into the health policy vacuum created by the Republicans’ failure to repeal and replace the Affordable Care Act. Proposals making the rounds include allowing Americans to buy into Medicare at age 55 or to buy into Medicaid.
Both Medicare and Medicaid pay lower prices to health care providers compared with private market plans offered by employers and in the Affordable Care Act marketplaces. On that basis, you might think these public programs are more cost-efficient. Are they?
Imagine that I take my car to the cheapest mechanic in town, while you take yours to the most expensive. My repairs, though costing less, don’t always fix the problem or last as long. You get what you pay for.
Let’s take a look at whether something similar is happening with public health programs. One study examined claims data for 26 low-value services and found that as much as 2.7 percent of Medicare’s spending is on these services alone, which include ineffective cancer screening, diagnostic testing, imaging and surgery. That sounds pretty bad.
But a paper that appeared in Health Services Research this year suggests that private plans do not perform better. Looking at the years 2009 to 2011, the authors compared the rates at which Medicare and private health plans provided seven low-value services. The services compared were among those identified as unnecessary by national organizations of medical specialists as part of the Choosing Wisely campaign.
The researchers found that four of the seven services they examined were provided at similar rates by Medicare and commercial market plans: cervical cancer screening over age 65; prescription opioid use for migraines; cardiac testing in asymptomatic patients; and frequent bone density scans. Medicare was less likely to pay for unnecessary imaging for back pain, but more likely to pay for vitamin D screening.
This finding might seem counterintuitive. Commercial market plans pay higher rates and confer higher profit margins, meaning there is more financial incentive for physicians to provide privately insured patients more of all types of care, whether low or high value.
But other results from the study suggest a more likely explanation: Doctors tend to treat all their patients similarly, regardless of who is paying the bill.
“What kind of insurance you have does affect your access to health care,” said Carrie Colla, associate professor of the Dartmouth Institute for Health Policy & Clinical Practice and the lead author of the study. “But once you’re in front of the doctor, by and large you’re treated the same way as any other patient.”
One apparent exception found in the study involved the seventh service it examined: cardiac testing before low-risk, noncardiac surgery. This service was provided to 46 percent of Medicare beneficiaries and 26 percent of privately insured patients. The large difference could reflect the fact that cardiac problems are more prevalent among older people. So a doctor with equal concern for all her patients might test Medicare patients at a higher rate for that reason. Nonetheless, such testing is considered low value even for the Medicare population.
Another recent study, published in JAMA Internal Medicine, also found little relationship between insurance status and low-value care. The study found no difference in the rates at which seven of nine low-value services were provided to patients on Medicaid versus those with private coverage. Six were also provided at the same rates for uninsured and privately insured patients.
Moreover, the study found that physicians who see a higher proportion of patients on Medicaid provide the same rate of low- and high-value services for all their patients as other physicians do. This is an important finding because Medicaid pays doctors less than private plans do, raising concerns that higher-quality doctors would tend not to participate in the program.
“Despite concerns to the contrary, Medicaid patients don’t appear to be seeing lower-quality doctors,” said Dr. Michael Barnett, lead author of the study, a physician with the Brigham and Women’s Hospital and an assistant professor at the Harvard T.H. Chan School of Public Health. “Though raising the prices Medicaid pays doctors may increase physician participation, enhancing enrollees’ access to care, it isn’t likely to change the quality of care patients receive once they are in the doctor’s office.”
If insurance status doesn’t influence how much low-value care patients are being offered, what does? In part, it seems related to the history and organization of local health care markets. A big culprit, according to Ms. Colla’s study, is a market’s ratio of specialists, like cardiologists and orthopedists, to primary care physicians. In areas where there are relatively more specialists, there is also more low-value care. That’s not to say that specialists don’t provide valuable services — but it suggests that they tend to provide more low-value care as well.
In a way, this is good news — the medical system doesn’t seem to discriminate by insurance status. It also means that public programs appear to be relatively cost-efficient, spending less than private payers for care of similar quality. That bodes well for Democrats’ proposals to expand Medicare or Medicaid.
But the bad news is that the study results imply that the value of care is hard to influence by adjusting prices. In a normal market, paying less for something would send a message of its low value, prompting people to provide less of it. The fact that price apparently does not influence doctors’ decisions is just another way in which health care does not seem to function like other markets.


As of Sept. 1, Anthem will no longer pay hospitals in five states for outpatient imaging services for MRIs or CT scans.
Anthem already initiated its policy in four other states on July 1.
Imaging is a big part of hospital revenue, and Anthem said it costs more to have the service done in a hospital outpatient setting than at a freestanding facility.
“Anthem’s primary concern is to provide access to quality and safe healthcare for our affiliated health plan members. We are also committed to reducing overall medical cost where possible when the safety of the member is not put at risk,” Anthem spokeswoman Lori McLaughlin said.
Hospitals in New York, Ohio, Colorado, Nevada and Georgia will be affected starting Friday. Hospitals in Indiana, Kentucky, Missouri and Wisconsin have been under the policy since July 1, when Anthem started what it calls its Imaging Clinical Site of Care program. It is administered by Anthem subsidiary, AIM Specialty Health, for its individual and employer-sponsored members in fully insured programs.
Imaging services can be just as safely provided in a lower cost, free-standing center as in a hospital outpatient setting, according to Anthem.
Anthem’s program also helps identify when hospital outpatient services for certain imaging tests are medically unnecessary, the company said.
Anthem’s policy follows a move in July by the Centers for Medicare and Medicaid Services to make hospital outpatient payments more site neutral. Procedures performed at hospital outpatient departments are paid at a higher rate through the hospital outpatient prospective payment system,than freestanding clinics, which are paid on the Medicare physician fee schedule.
CMS said it would reduce outpatient prospective payment system spending by approximately $500 million in 2017 by no longer paying for outpatient services at a higher rate.
In the divide between pricing and payer reimbursement, providers nationwide may be concerned that other insurers will follow the lead of a large insurer such as Anthem.
“Hospitals need to recognize they are competing in a market already delivering on convenience, quality and affordability,” McLaughlin said.
Anthem said the program gives members an opportunity to save up to hundreds of dollars for each imaging test.
The cost for MRIs and CT scans can vary from $350 to $2,000, Anthem said in 2010 when it launched its imaging cost and quality program to help educate members about their options in choosing high-quality, lower-cost imaging services.
Yet a recent report shows that many consumers don’t make any attempt to compare prices for healthcare services. Most survey respondents said they didn’t comparison shop or even ask how much they would owe in copayments or other cost-sharing expenses before they turned up for an appointment.
In cases in which it’s not medically necessary for a member to receive services from a hospital, members who go to a freestanding facility can save close to $1,000 out-of-pocket for some imaging services for those who haven’t met their deductible, and up to $200 for those whose plans require only a copay, Anthem said.
Members who have high-deductible plans and haven’t yet met their deductible may be responsible for the full cost of the service. In these cases the member saves the difference between the hospital imaging cost and the non-hospital cost, Anthem said.
Other members will pay a co-insurance usually of about 20 percent on the full cost of the service. Plans pay the other 80 percent.
If a member chooses to go to an outpatient hospital facility, and that in-network facility provides the service, it would be the provider, and not the patient, who would be responsible for the cost, according to Anthem. The member would only be held responsible for the cost of the service if he or she signs a waiver, agreeing to be responsible, Anthem said.
Hospitals would then bear the cost of their imaging services provided at outpatient facilities, for beneficiaries covered by Anthem insurance.
Anthem’s exceptions to its policy include: when the services being provided are only available in the hospital setting, the individual requires an obstetrical observation, or the individual is receiving perinatology services. Also, exceptions are in cases where there is no other geographically accessible site, moderate or deep sedation or general anesthesia is required and a freestanding facility does not have this available; the equipment for the size of the individual is not available, or the individual has a documented diagnosis of claustrophobia requiring open magnetic resonance imaging which is not available in a freestanding facility.
AIM collects data on imaging providers, both hospital-based and freestanding, to determine conformance to industry-recognized standards, Anthem said. Providers and staff have access to each facility’s score in an AIM portal, and can use those scores to find facilities.

Who contributes to what you pay at the pharmacy? Why are prescription drugs so expensive in the United States? In this Facebook Live, KHN’s Julie Appleby talks with Stephanie Stapleton and answers readers’ questions about the prescription drug pricing pipeline and the industry stakeholders who have a role in what you pay.
For more in-depth conversations with KHN reporters, check out our Facebook video archive.
Here are videos and a chart to help make sense of drug pricing. And remember you can republish KHN content for free:
Pharmacy benefit managers — companies that are often unnoticed and even less understood by most consumers — hold an important place in the prescription drug-pricing pipeline. In this video, Kaiser Health News details the emergence of these multimillion-dollar corporations and the impact they have on medication costs and patients’ access to these treatments.

With Republican efforts to “repeal and replace” the Affordable Care Act stalled, tentative bipartisan initiatives are in the works to shore up the fragile individual insurance market that serves roughly 17 million Americans.
The Senate Health, Education, Labor and Pensions Committee launches hearings the week Congress returns in September on “stabilizing premiums in the individual insurance market” that will feature state governors and insurance commissioners. A bipartisan group in the House is also working to come up with compromise proposals.
Both before and after implementation of the federal health law, this market — serving people who don’t get coverage through work or the government — has proved problematic. Before the law, many people with preexisting health conditions could not get insurance at any price. Now, consumers in the individual market often face higher out-of-pocket costs and fewer choices of health care providers and insurers than in past years. More than 12 million people buy that insurance through the ACA’s marketplaces, while another 5 million buy it outside of the exchanges.
Policymakers generally agree on what immediate efforts to stabilize the market might include. At the top of most lists is ensuring federal payment of subsidies to insurers to pay the out-of-pocket expenses — such as deductibles and copayments — to protect customers with the lowest incomes. Insurers also want the federal government to continue enforcing the requirement that most Americans either have insurance or pay a tax penalty, and continuing efforts to get uninsured people to sign up for coverage during the upcoming open enrollment period, from Nov. 1 to Dec. 15. Those efforts are essential, insurers say, to help keep healthy customers in their risk pools to defray the costs of beneficiaries with medical needs.
But what about ideas that go beyond the oft-repeated ones? Here are five proposals that are more controversial but generating buzz.



