In a concession to Wall Street investors, starting this summer, UnitedHealth will stop paying commissions to agents and brokers for some new enrollees in nearly 200 UnitedHealthcare Medicare Advantage plans across 39 markets.
And it’s happening not because UnitedHealth can’t afford to pay.As we’ve published previously, the company reported $9.1 billion in profits during the first quarter of 2025 — up from $7.9 billion the year before. But that wasn’t enough to satisfy Wall Street, which punished UnitedHealth with the steepest one-day stock drop in 26 years — a $110 billion free fall in market value — after the company revised its full-year profit guidance downward.
Why the drop?
Because UnitedHealth admitted it may not squeeze quite as much profit from taxpayers this year as expected — mainly due to unexpectedly high care utilization from some of the new Medicare Advantage enrollees it brought on during the last open enrollment period. Particularly enrollees who, as then-CEO Andrew Witty described, came from other insurers exiting the market and hadn’t been properly coded. Yawn.
For Now, Brokers Are UNH’s Patsy
This recent commission cut is less about operational efficiency and more about damage control. UnitedHealth is signaling to investors that it’s willing to shrink its Medicare Advantage footprint — at least temporarily — if that helps preserve profit margins. And Wall Street analysts are eating it up, seeing it as a way to slow the flow of high-cost members and stabilize earnings, according to BarChart.
Off Wall Street, the move has already come under fire. As the National Association of Benefits and Insurance Professionals put it, UnitedHealth is “cutting off the very people best equipped to help” seniors — especially low-income and rural enrollees who depend on brokers to explain their options.
While we would warn seniors against enrolling in a Medicare Advantage plan in the first place – without brokers, many beneficiaries will be left to fend for themselves in a system that’s already infamously confusing, expensive and deadly.
A Strategic Retreat Disguised as a Cost-Containment Strategy
The problem is the perverse incentive structure UnitedHealth and other insurers helped build — one that rewards risk-coding gamesmanship more than it rewards delivering care. For years, the company thrived by maximizing revenue through “coding intensity” and by acquiring everything from doctors’ offices to behavioral health firms to control more of the health care ecosystem.
Now, UnitedHealth is responding the way Wall Street expects: by slashing anything that isn’t bolted down – including brokers.
So here we are:
UnitedHealth is still wildly profitable, still drawing billions from taxpayer-funded programs like Medicare and Medicaid — and now it’s cutting out the professionals who presumably help seniors navigate a convoluted health care system. All this, mind you, to appease jittery investors. And despite UnitedHealth’s current wobbly share price, analysts expect it to rebound, especially with a continuation of share buybacks on the horizon.
During the first quarter of this year alone, the company bought back $3 billion worth of its own shares. Over the past year, buybacks totaled more than $12 billion. When you factor in dividends, the company said it “returned” more than $16 billion to shareholders in 2024. That’s how you keep investors at least partially satisfied.
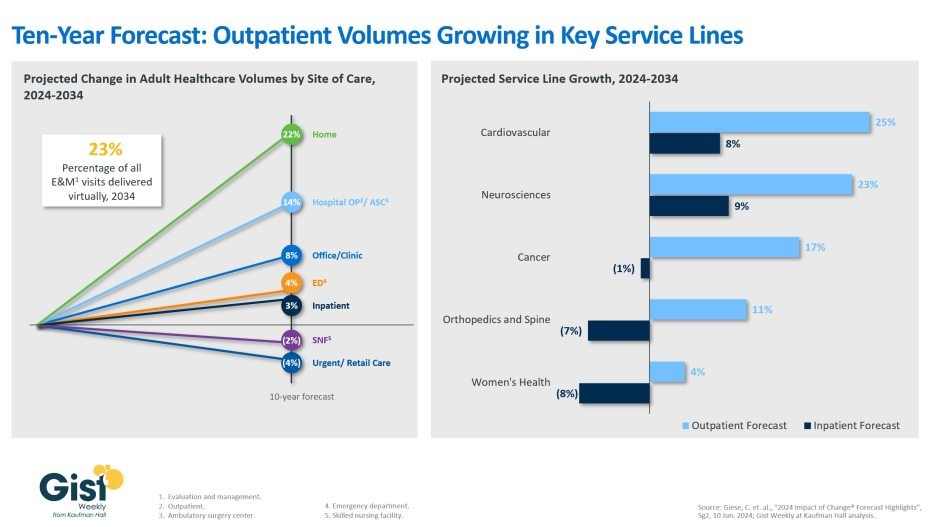
Using the latest data forecast from Sg2, a Vizient company, the graphic above illustrates how the outpatient shift will continue to accelerate through 2034.
Home-based care and outpatient services, including ambulatory surgery centers, are projected to be the fastest growing care sites over the next decade, with volumes increasing 22% and 14% respectively.
Sg2 forecasts that physician offices, emergency departments, and inpatient settings will experience more modest volumes increases, whereas skilled nursing facilities and retail care volumes are predicted to decline.
Additionally, although the initial outpatient procedural shift was largely focused on orthopedics, the next wave of outpatient volume growth will come from other service lines.
Driven by regulatory changes, as well as patient demand, outpatient cardiovascular volumes are expected to increase by 25% over the next decade, closely followed by neurosciences at 23%.
Continued health system investment into higher-acuity outpatient care remains crucial.
On the one hand, the alternative to traditional Medicare is still popular among consumers, who have been lured by the promises of lower out-of-pocket costs and increased supplemental benefits.
On the other hand,Medicare Advantage profitability is on the decline, as shown in recent quarterly reports from the large insurers. The headwinds, executives said during recent earnings calls, have been due to greater than expected utilization of benefits and lower than expected reimbursement from the government.
Adding to MA’s margin challenges are providers who are making the decision to cut their ties with MA plans rather than deal with delays in prior authorization and claims payments.
Moody’s Investors Service said this year, and an HFMAsurvey from March indicates 19% of health systems have discontinued at least one Medicare Advantage plan, while 61% are planning to or considering dropping Medicare Advantage payers.
Until recently, the story of Medicare Advantage was one of ascendancy. Just last year it hit a milestone: More than half of eligible Medicare beneficiaries are now in MA plans. So why is business taking a step back?
WHY THIS MATTERS
There are many factors at play, but a big one is the 3.7% rate increase for 2025 that Medicare Advantage plans will receive from the Centers for Medicare and Medicaid Services. The federal government is projected to pay between $500 and $600 billion in Medicare Advantage payments to private health plans, according to the 2025 Advance Notice for the Medicare Advantage and Medicare Part D Prescription Drug Programs released in April.
The payment rate was considered inadequate by insurers, who were also troubled over other key factors, including a 0.16% reduction in the Medicare Advantage benchmark rate for 2025, which represents a 0.2% decrease.
“AHIP has strong concerns that the estimated growth rate in the Advance Notice – an average of 2.44% – will lead to benchmark changes that are insufficient to cover the cost of caring for 33 million MA beneficiaries in 2025,” AHIP president and CEO Mike Tuffin said in April. “The estimate does not reflect higher utilization and cost trends in the healthcare market that are expected to continue into 2025.”
According to Karen Iapoce, vice president Government Programs at ZeOmega, the cost of running an MA business is increasing due to the burdens being placed on health plans.
“If you sit inside with a health plan, they’re asked to do a lot with not as much bandwidth as they had before,” said Iapoce. “For example, health equity requires plans to have new regulatory guidance they need to meet. There’s a host of measures around health equity. Our plans are not in the business of really understanding how to manage transportation, how to manage housing, so they’re working with other entities. This requires an expert to sit in with the health plan … and then track and report. On the business end, they want to show an ROI, but that could be six months or a year down the line.”
Because of that, she said, the benchmark rate is likely insufficient to cover the projected increase in administrative and other costs. Iapoce said the benchmark rates represent the maximum amount that will be paid to a person in a given county; this is used as a reference point for calculation. If a plan is higher than the benchmarks, the premiums end up going to the beneficiary. More commonly, the plans bid below the benchmark, and the difference represents the rebate plans will receive. But they also factor into risk adjustment.
“The plans are getting into these contract negotiations, so they have to know what goes into that benchmark,” said Iapoce. “I might not be a high utilizer, but you may be. If we’re bringing in a community of high utilizers, there’s no one offsetting that. There’s no balance.”
Richard Gundling, senior vice president, content and professional practice guidance at HFMA, said MA plans started running into these issues when the program crossed over the threshold of more than 50% of beneficiaries.
“When a Medicare Advantage plan comes in, then all the extra administrative burdens come into play,” said Gundling. “So you have prior authorizations, all the issues around lack of payment and denials. Patients get caught in the middle, and in particular elderly patients think they’re still on traditional Medicare.
“It used to be that healthier beneficiaries went into Medicare Advantage,” he added. “Sicker beneficiaries tended to stay in traditional Medicare. That’s not the case anymore, and so there’s a higher spend.”
Gundling said beneficiaries are likely flocking to MA with visions of lower costs and increased benefits such as eyeglasses and hearing aids, and many don’t realize the tradeoffs, such as prior authorizations and network restrictions.
MA remains popular with seniors, but studies show the plans cost the government more money than original Medicare.
A 2023 Milliman report showed annual estimated healthcare costs per beneficiary are $3,138, compared to $5,000 for traditional fee-for-service Medicare, and over $5,700 if a traditional Medicare beneficiary also buys a Medigap plan.
MA membership has grown nationally at an annual rate of 8% to approximately 32 million, while traditional Medicare has declined at an average annual rate of 1%. As that has happened the percentage of people choosing MA has grown to 49% from 28%, data shows.
Yet Medicare Advantage profitability is on the decline, Moody’s found in February. That’s largely because of a significant spike in utilization for most of the companies, which Moody’s expects will result in lower full-year MA earnings for insurers. Adding to that is lower reimbursement rates for the first time in years that are likely to remain weaker in 2025 and 2026, which is credit negative.
Moody’s analysts contend that MA may have “lost its luster,” citing as evidence Cigna’s efforts to sell its MA business, even after a failed merger with Humana.Cigna this past winter announced it had entered into a definitive agreement to sell its Medicare Advantage, Supplemental Benefits, Medicare Part D and CareAllies businesses to Health Care Service Corporation (HCSC) for about $3.7 billion.
Iapoce said Medicare Advantage may be a victim of its own success.
“Because of all this great promotion about what a Medicare Advantage plan can do for you, you’re seeing an increase in enrollment, or more people moving over, and the demographics are starting to change,” she said.
For many consumers, the appeal of an MA plan is the same as that of an online retailer like Amazon, said Iapoce. Such retailers offer one-stop shopping for a variety of goods, and the perception is that MA essentially offers one-stop shopping for a variety of healthcare services and benefits.
But while this massive shift is happening, it puts providers in an awkward position, said Iapoce.
“Their reimbursement is almost being dictated, in essence, by a health plan,” she said. “It almost feels like the payer has the upper hand over the provider. Think: I’m a provider. It’s my job to get this female with this particular age and condition a mammogram, and the health plan has told me to get her a mammogram. But you, as the health plan, get the money for it. I, as the provider … what am I getting? What’s it doing for me? It becomes this very tense situation, and the provider is probably the entity that is running on the thinnest of staff.”
Gundling expects that despite some “growing pains,” MA will remain viable and continue to grow.
“Nobody’s going to stay still,” said Gundling. CMS has to consider, ‘Are we paying the health plans appropriately for the types of patients they have?’ And then health plans will need to look at their medical utilization rules – ‘Are we overdoing pre-authorization or denying things appropriately?’ And providers need to say, ‘This is a market we need to continue to grow.’
“There’s still going to be a role for it,” he said. “It’s just that we’ve introduced a larger population into it, and I think that’s where a lot of the surprises come in.”
THE LARGER TREND
CVS reportedearlier this month that healthcare-benefits medical costs, primarily due to higher-than-expected Medicare Advantage utilization, came in approximately $900 million above expectations.
Last month, Humana said it expected membership may take a hit from future Medicare Advantage pricing resulting from the CMS payment rate notice. Humana is actively evaluating plan level pricing decisions and the expected impact to membership, president and COO James Rechtin said on the call.
Elevance Health, formerly Anthem, reported a 12.2% earnings increase for Q1, but company margins have not been as affected as those insurers that are heavily invested in the MA market. Fewer of its members are in MA plans compared to other large insurers Humana, CVS Health or UnitedHealth Group, executives said.
This is National Hospital week. It comes at a critical time for hospitals:
The U.S. economy is strong but growing numbers in the population face financial insecurity and economic despair. Increased out-of-pocket costs for food, fuel and housing (especially rent) have squeezed household budgets and contributed to increased medical debt—a problem in 41% of U.S. households today. Hospital bills are a factor.
The capital market for hospitals is tightening: interest rates for debt are increasing, private investments in healthcare services have slowed and valuations for key sectors—hospitals, home care, physician practices, et al—have dropped. It’s a buyer’s market for investors who hold record assets under management (AUM) but concerns about the harsh regulatory and competitive environment facing hospitals persist. Betting capital on hospitals is a tough call when other sectors appear less risky.
Utilization levels for hospital services have recovered from pandemic disruption and operating margins are above breakeven for more than half but medical inflation, insurer reimbursement, wage increases and Medicare payment cuts guarantee operating deficits for all. Complicating matters, regulators are keen to limit consolidation and force not-for-profits to justify their tax exemptions. Not a pretty picture.
And, despite all this, the public’s view of hospitals remains positive though tarnished by headlines like these about Steward Health’s bankruptcy filing last Monday:
The public is inclined to hold hospitals in high regard, at least for the time being. When asked how much trust and confidence they have in key institutions to “to develop a plan for the U.S. health system that maximizes what it has done well and corrects its major flaws,” consumers prefer for solutions physicians and hospitals over others but over half still have reservations:
A Great Deal
Some
Not Much/None
Health Insurers
18%
43%
39%
Hospitals
27%
52%
21%
Physicians
32%
53%
15%
Federal Government
14%
42%
44%
Retail Health Org’s
21%
51%
28%
The American Hospital Association (AHA) is rightfully concerned that hospitals get fair treatment from regulators, adequate reimbursement from Medicare and Medicaid and protection against competitors that cherry-pick profits from the health system.
It can rightfully assert that declining operating margins in hospitals are symptoms of larger problems in the health system: flawed incentives, inadequate funding for preventive and primary care, the growing intensity of chronic diseases, medical inflation for wages, drugs, supplies and technologies, the dominance of ‘Big Insurance’ whose revenues have grown 12.1% annually since the pandemic and more. And it can correctly prove that annual hospital spending has slowed since the pandemic from 6.2% (2019) to 2.2% (2022) in stark contrast to prescription drugs (up from 4% to 8.4% and insurance costs (from -5.4% to +8.5%). Nonetheless, hospital costs, prices and spending are concerns to economists, regulators and elected officials.
National health spending data illustrate the conundrum for hospitals: relative to the overall CPI, healthcare prices and spending—especially outpatient hospital services– are increasing faster than prices and spending in other sectors and it’s getting attention: that’s problematic for hospitals at a time when 5 committees in Congress and 3 Cabinet level departments have their sights set on regulatory changes that are unwelcome to most hospitals.
My take:
The U.S. market for healthcare spending is growing—exceeding 5% per year through the next decade. With annual inflation targeted to 2.0% by the Fed and the GDP expected to grow 3.5-4.0% annually in the same period, something’s gotta’ give. Hospitals represent 30.4% of overall spending today (virtually unchanged for the past 5 years) and above 50% of total spending when their employed physicians and outside activities are included, so it’s obvious they’ll draw attention.
Today, however, most are consumed by near-term concerns– reimbursement issues with insurers, workforce adequacy and discontent, government mandates– and few have the luxury to look 10-20 years ahead.
I believe hospitals should play a vital role in orchestrating the health system’s future and the role they’ll play in it. Some will be specialty hubs. Some will operate without beds. Some will be regional. Some will close. And all will face increased demands from regulators, community leaders and consumers for affordable, convenient and effective whole-person care.
For most hospitals, a decision to invest and behave as if the future is a repeat of the past is a calculated risk. Others with less stake in community health and wellbeing and greater access to capital will seize this opportunity and, in the process, disable hospitals might play in the process.
Near-term reactive navigation vs. long-term proactive orchestration–that’s the crossroad in front of hospitals today. Hopefully, during National Hospital Week, it will get the attention it needs in every hospital board room and C suite.
PS: Last week, I wrote about the inclination of the 18 million college kids to protest against the healthcare status quo (“Is the Health System the Next Target for Campus Unrest?” The Keckley Report May 6, 2024 www.paulkeckley.com). This new survey caught my attention:
According to the Generation Lab’s survey of 1250 college students released last week, healthcare reform is a concern. When asked to choose 3 “issues most important to you” from its list of 13 issues, healthcare reform topped the list. The top 5:
Health Reform (40%)
Education Funding and access (38%)
Economic fairness and opportunity (37%)
Social justice and civil rights (36%)
Climate change (35%)
If college kids today are tomorrow’s healthcare workforce and influencers to their peers, addressing the future of health system with their input seems shortsighted. Most hospital boards are comprised of older adults—community leaders, physicians, et al.
And most of the mechanisms hospitals use to assess their long-term sustainability is tethered to assumptions about an aging population and Medicare.
College kids today are sending powerful messages about the society in which they aspire to be a part. They’re tech savvy, independent politically and increasingly spiritual but not religious. And the health system is on their radar.
The big question coming out of the health insurance earnings season is how much elevated utilization among seniors is carrying over into 2024.
Medicare Advantage medical costs dominated fourth-quarter discussions between health insurers and investors, after higher healthcare utilization popped up like weeds in some segments of each payers’ business.
Yet health insurers’ forecasts for how higher utilization will affect their performance in 2024 are night and day.
Some payers controlled medical costs more effectively than analysts expected, said rising spending shouldn’t affect their outlooks for this year or guided to a stronger 2024 than previously forecast. That group includes UnitedHealth, Centene, Elevance and Cigna.
However, Humana and CVS cut their 2024 earnings outlooks on the heels of last year’s results, and said they expect elevated medical costs to continue this year.
Humana’s outlook is especially grim: The Kentucky-based payer’s earnings expectations for 2024 came in about half as low as analysts had expected.
Even payers that emerged from 2023 with their financial outlooks unscathed said they plan to cut benefits or raise premiums this year. The plan redesigns are to protect margins in MA — a business that historically generates significant profits, but is facing challenges that threaten to kill the golden goose.
Yet, more members are creating more problems for some insurers because of rising medical utilization. Starting in the second quarter last year, seniors sought out medical care they had delayed during the COVID-19 pandemic, hiking insurers’ spending.
For example, CVS added 800,000 MA enrollees for 2024, mostly nabbed from other payers after CVS aggressively expanded its benefits. But that’s coming back to haunt the Rhode Island-based insurer, which cut its earnings per share outlook for this year due to high medical costs.
There are a few potential explanations for what’s driving the elevated utilization, and whyinsurers might not have properly forecast the uptick in trend, according to J.P. Morgan analyst Lisa Gill.
Enrollees in MA tend to be healthier than those in traditional Medicare. But as more seniors join MA, the program’s risk population could be skewing sicker, Gill wrote in an early February research note. Insurers could have missed early warning signs of higher acuity as seniors avoided doctor’s offices during the pandemic.
Higher demand could have also existed earlier, but providers might not have been able to address it because of labor shortages that have now ameliorated, Gill said. Similarly, insurers could have added new MA enrollees with less diagnosis history relative to the rest of their population, resulting in lower visibility into their conditions.
Medical loss ratio is a useful metric for understanding how unexpectedly high utilization is affecting insurers.
Medical loss ratio, or MLR, is a percentage of how much in healthcare premiums insurers spend on clinical services and quality improvement. The higher the MLR, the less in premiums insurers are spending on administration or marketing — or retaining as profit. As such, insurers generally try to keep their MLRs low (though within regulatory bounds to avoid sanctions).
MLRs soared in payers’ Medicare businesses in the fourth quarter, as the utilization trends that emerged earlier in 2023 conflated with a typical seasonal rise in medical spending during the winter months.
Utilization inflation
Insurers chalked the increase in medical costs up to different drivers.
Seniors covered by UnitedHealth and Humana, which together hold almost half of the total MA market share, continued to seek outpatient care in droves in the fourth quarter, including procedures like orthopedic surgeries.
UnitedHealth’s members required more spending on seasonal diseases like the flu, COVID or respiratory virus RSV. Elevance, Centene and CVS also reported elevated outpatient care overall for things like elective procedures, along with higher spend on seasonal needs.
That wasn’t the case for Cigna — which had lower than expected spending on seasonal diseases — and Humana. Humana’s uptick in care was “not respiratory driven,” said CFO Susan Diamond on the payer’s fourth-quarter earnings call in January.
“We don’t have any clear indicators that it is something you can reasonably assume is seasonal,” Diamond said.
As for inpatient care, Centene and CVS didn’t report higher utilization of hospital services than expected. Elevance also didn’t say that inpatient trends were contributing to growing costs.
Yet, UnitedHealth and Humana warned investors about rising inpatient costs, which is concerning for insurers given hospital care is more expensive to cover. UnitedHealth blamed pricey COVID admissions, while Humana said it was seeing more short stays in hospitals across the board.
Humana’s Diamond said recent government regulations requiring MA payers to comply with coverage determinations in traditional Medicare could be a potential driver of the higher inpatient spend. The rule requires insurers to cover an inpatient admission if the patient is expected to require hospital care for at least two midnights.
Other insurers said they had planned for the so-called “two-midnight rule.”
The increase in utilization — combined with weaker payment rates, changes to MA quality ratings and a shifting risk adjustment model — have created an updraft for MLRs, especially for insurers with high exposure to MA like Humana and UnitedHealth.
The big question is how much of this utilization will carry over into this year, and whether payers have properly accounted for utilization changes in their plan designs.
Every major insurer besides Elevance expects to record a higher MLR in 2024 than in 2023. Though, the size of the growth ranges from a 0.8 percentage point increase for UnitedHealth to a 2.7 percentage point increase for Humana.
In response to the challenging financial environment, payers — even those that excelled in controlling medical costs last year — said they’ve been pulling back benefits, raising premiums or exiting underperforming markets to boost profitability.
That’s true for insurers that expect their MA membership to grow this year (UnitedHealth, CVS), and those that expect it to fall (Cigna) or stay flat (Elevance).
As a result, further growth could be curtailed as payers prioritize margins.
“We are first and foremost focused on recovering margin, and market share gains is a secondary consideration,” Brian Kane, who leads CVS’ health benefits division, told investors during its February earnings call.
“I look at next year as a year that I think the whole industry will possibly reprice. I don’t know how the industry can take this kind of increase in utilization along with regulatory changes that will continue to persist in 2025 and 2026,” Humana CEO Bruce Broussard said on the payer’s earnings call.
Insurers said they could revise plans further in light of MA rates for 2025 that the government proposed midway through the earnings reporting season. The rates represent a renewed effort by regulators to rein in growing spending in Medicare.
Executives with Humana, Centene and CVS all said the payment changes are insufficient to cover cost trends. Humana and Centene said the rule would result in a 1.6% and 1.3% drop in rates, respectively. (That’s before risk scoring, which should result in an overall increase in reimbursement in 2025).
Insurers warned regulators that seniors could see their benefits reduced if they finalize the rates as proposed.
“We’ll just adjust the bids accordingly,” Asher said on Centene’s call. “The products may be a little less attractive for seniors from an industry standpoint if we don’t make a lot of progress on the final rates.”
Runaway inpatient spending in particular caused CVS’ insurance costs to snowball after returning “to patterns we have not seen since the start of the pandemic,” its CFO said.
Dive Brief:
CVS had a significantly worse first quarter than the healthcare giant — or Wall Street — expected, after its insurance arm failed to adequately prepare for seniors’ high use of medical care, especially in inpatient facilities.
The Rhode Island-based company’s health services segment — usually a reliable driver of growth — also saw its revenue and income fall in the quarter as its pharmacy benefit manager adjusted to the loss of a major contract with insurer Centene.
CVS slashed its earnings expectations for 2024 on Wednesday following the results. It’s the second time the company has lowered financial expectations this calendar year. “Clearly this is a disappointing result for us,” CFO Tom Cowhey said on a Wednesday call with investors, after which CVS’ stock fell more than 19%.
Dive Insight:
CVS brought in revenue of $88.4 billion in the quarter, up 4% year over year but significantly below analysts’ expectations. Net income was slashed by almost half compared to the prior-year quarter, to $1.1 billion.
The quarter was “burdened by utilization pressures in Medicare Advantage,” CEO Karen Lynch said on the call.
Starting last year, MA seniors began using higher levels of medical services after a long dry spell during the COVID-19 pandemic. The trend has continued into this year, leaving private insurers that manage the plans scrambling to contain costs.
CVS assumed utilization would moderate somewhat coming into the first quarter, but instead it was “notably above” expectations, according to Lynch.
Outpatient services, like mental health and medical pharmacy, along with supplemental benefits like dental continued to be elevated in the first quarter. However, inpatient utilization was particularly to blame for runaway spending.
Inpatient admissions per thousand in the quarter were up “high-single digits” compared to the same time last year, Cowhey said. A small portion of the growth was expected due to implementation of the CMS’ two-midnight rule that’s resulted in insurers having to cover more inpatient admissions. But overall, admissions “meaningfully exceeded” expectations for the quarter, according to the CFO.
“Inpatient seasonality returned to patterns we have not seen since the start of the pandemic,” Cowhey said.
Executives stressed that some of those costs appear to be seasonal and shouldn’t carry into the rest of the year. Inpatient utilization patterns are similar to what CVS’ insurance arm Aetna sawin normal years before the COVID-19 pandemic, and appear to be moderating in April, according to Lynch.
Still, the higher utilization caused the insurer’s medical loss ratio — a marker of spending on patient care — to soar to 90.4% in the first quarter, compared to 84.6% during the same time last year.
Overall, medical costs in the quarter were about $900 million higher than CVS expected, Cowhey said.
CVS’ results suggest the insurer “severely underestimated utilization of new members,” TD Cowen analyst Charles Rhyee wrote in a Wednesday morning note. “Investors already had lowered expectations for MA, but actual results and impact to guidance is likely way worse than expected.”
CVS added more MA members coming into 2024 than any other U.S. health insurer, according to an analysis by consultancy Chartis. That growth caused CVS’ membership to grow 1.1 million members in the first quarter compared to the end of 2023, to 26.8 million individuals.
Revenue in CVS’ health benefits segment, which houses its insurer Aetna, subsequently inflated to $32.2 billion, up 21% compared to the fourth quarter of 2023.
Despite the boom, higher medical costs slashed the segment’s operating income, as did the impact of lower quality ratings in MA.
Lower quality or “star” ratings for 2024 cut steeply into CVS’ reimbursement. Aetna’s largest contract fell from 4.5 stars to 3.5 stars for 2024, causing the payer to lose out on about $800 million in revenue.
As a result of the pressures, “we think [MA] will lose a significant amount of money this year,” Cowhey said.
Following the quarter, CVS lowered its full-year financial expectations for earnings per share on a GAAP and adjusted basis, and for cash flow from operations.
CVS expects to notch an MLR of 89.8% in 2024, up 2.1 percentage points from its previous guidance, because of continued medical utilization pressures, Cowhey said.
Moving into 2025, CVS does expect to recover most of what it lost this year from the star ratings changes. But the insurer faces another setback: MA payment rates recently finalized for 2025 that insurers are slamming as a cut, despite only a modest decrease in base rates.
On the call, Lynch maligned the rates as “insufficient” and a “significant added disruption” in the program.
Like its other peers with major MA footprints, CVS plans to focus on improving profits at the potential expense of members. That includes hiking premiums and exiting counties where Aetna thinks it can’t improve profits in the near term. Aetna could lose members as a result, but the size of eventual losses will in large part depend on what the insurer’s competitors do, according to CVS executives.
Other major MA payers have said they will take similar steps to hike profits.
CVS also dealt with lower visibility into its claims in the quarter because of the massive cyberattack on claims clearinghouse Change Healthcare earlier this year. Change took its systems offline as a result, hamstringing providers’ payments across the U.S. and making it harder for insurers to predict how much they might have to spend on their members’ medical costs.
CVS established a reserve of nearly $500 million for claims it estimates were lodged in the quarter but it has yet to receive. Cowhey said the insurer is “confident” about the adequacy of its reserves.
STAT News today published an op-ed I coauthored with Dr. Philip Verhoef, president of Physicians for a National Health Program, making the point that investors are among the growing number of stakeholders who are souring on big, for-profit insurance companies like the ones I used to work for (Cigna and Humana).
We focused specifically on investors’ concerns about the continued profitability of Medicare Advantage plans most of the big insurers own and operate.
Several companies have lost billions of dollars in market capitalization over the past several weeks as they have reported what they maintain is higher than usual utilization of health care goods and services by seniors enrolled in MA plans.
Today, the companies–especially UnitedHealth Group, the market leader with 7.6 million Medicare Advantage enrollees–are losing billions more in market cap on the news, broke yesterday by the Wall Street Journal, that the Department of Justice is investigating UnitedHealth’s many acquisitions over the years.
UnitedHealth and most of the other companies are no longer just insurance companies. They’ve moved rapidly into health care delivery by buying physician practices and clinics, and three of them, UnitedHealth, Cigna and CVS/Aetna, control 80% of the pharmacy benefit management business.
Investors in MA insurance companies experienced a rude awakening in late January, with insurer stocks plummeting in the face of earnings reports showing profits falling far below expectations in the last quarter of 2023. Companies like CVS Health and UnitedHealth Group saw losses of 5.2% and 6.2% respectively, while Humana, whose business model relies heavily on the MA program, fell an astonishing 14.2%. These insurers cited higher than average health care utilization rates as the culprit and warned that 2024 would likely see more of the same. At the same time, private equity investment in MA has fallen, showing waning confidence in the program.
We went on to note that both Democrats and Republicans in Congress are increasingly concerned about MA insurers’ business practices and, among other things, have introduced bills to crack down on egregious overpayments to MA plans.
The WSJ reported yesterday that the Justice Department has launched an antitrust investigation into UnitedHealth, which has become not only the country’s biggest U.S. health insurer but also a leading manager of drug benefits “and a sprawling network of doctor groups.”
The investigators have in recent weeks been interviewing healthcare-industry representatives in sectors where UnitedHealth competes, including doctor groups, according to people with knowledge of the meetings.
The DOJ’s investigation of UnitedHealth is wide-ranging. Among other things, according to the Journal, “investigators have asked whether and how the tie-up between UnitedHealthcare [the insurance division] and Optum’s medical groups might affect its compliance with federal rules that cap how much a health-insurance company retains from the premiums it collects. (Optum is the company’s division that encompasses the pharmacy benefit manager Optum Rx and the many clinics and physician practices it owns.)
HEALTH CARE un-coveredexplained last month how UnitedHealth essentially is paying itself billions of dollars every month and circumventing the intent of a federal law that requires insurers to spend at least 80% of premium dollars on their health plan enrollees’ health care.
I know from sources within the Justice Department that investigators saw that piece, as well as the comprehensive analysis we published earlier of the scores of acquisitions UnitedHealth has made in recent years that have enabled it to catapult to the top five of the Fortune 500 list of American companies.
Those sources told me that the DOJ is very concerned about the consolidation within both the health insurance business and the hospital industry. Many U.S. hospitals, in an ongoing effort to negotiate from an enhanced position of strength with UnitedHealth and the other vertically integrated insurers, have merged with each other in recent years and become part of huge health-care delivery systems.
At the close of trading on the New York Stock Exchange yesterday, shares of UnitedHealth Group’s share were down $11.90 or 2.27%. Investors are continuing to head for the exits today. As I write this, the company’s stock price has fallen another $20 (4%) to $494.00. That’s way down from the company’s 52-week high of $554.70.
Shares of most of the other big publicly traded insurers (Centene, Cigna, CVS/Aetna, Elevance, Humana and Molina) are also down, ranging from $.83 at CVS to $11.51 at Humana.
HCA Healthcare is the single hospital operator that Bloomberg identifies as one of “50 Companies to Watch in 2024.”
“From Alphabet and BYD to Eli Lilly and Vivendi, keep an eye on these global stocks this year,” the outlet proposes for the 50 companies out of the 2,000 firms assessed. Bloomberg analysts highlighted the companies as those warranting a closer look, based on “contrarian views and upcoming catalysts for change such as new leadership, asset sales or acquisitions, and plans for new products and services.”
With 182 hospitals and more than 37,000 hospital beds, Bloomberg analyst Glen Losev said HCA “faces cost and revenue challenges that point to a reduction in its operating margin. Wages are increasing, especially for nurses, as are non-labor costs because of general inflation. And fewer physician visits indicate softening demand for care in areas such as elective surgeries.”
HCA is tied to an estimated 5% increase to its revenue in 2024 with a market cap of $72 billion.
The company posted $47.66 billion in revenue for the first nine months of 2023 compared to $44.73 billion in the same period of 2022. Its fourth quarter earnings are due later this month.
Other healthcare companies recognized by Bloomberg as worth watching are Novo Nordisk, BeiGene, Boston Scientific and Eli Lilly. Weight loss drug possibilities drive potential for Novo Nordisk and Eli Lilly, with estimated revenue increases of 22% and 16%, respectively.
Not long ago, I opened a new box of cereal and found a lot fewer flakes than usual. The plastic bag inside was barely three-quarters full.
This wasn’t a manufacturing error. It was an example of shrinkflation.
Following years of escalating prices (to offset higher supply-chain and labor costs), packaged-goods producers began facing customer resistance. So, rather than keep raising prices, big brands started giving Americans fewer ounces of just about everything—from cereal to ice cream to flame-grilled hamburgers—hoping no one would notice.
This kind of covert skimping doesn’t just happen at the grocery store or the drive-thru lane. It’s been present in American healthcare for more than a decade.
What Happened To Healthcare Prices?
With the passage of the Medicare and Medicaid Act in 1965, healthcare costs began consuming ever-higher percentages of the nation’s gross domestic product.
In 1970, medical spending took up just 6.9% of the U.S. GDP. That number jumped to 8.9% in 1980, 12.1% in 1990, 13.3% in 2000 and 17.2% in 2010.
This trajectory is normal for industrialized nations. Most countries follow a similar pattern: (1) productivity rises, (2) the total value of goods and services increases, (3) citizens demand better care, newer drugs, and more access to doctors and hospitals, (4) people pay more and more for healthcare.
But does more expensive care equate to better care and longer life expectancy? It did in the United States from 1970 to 2010. Longevity leapt nearly a decade as healthcare costs rose (as a percentage of GDP).
Then American Healthcare Hit A Ceiling
Beginning in 2010, something unexpected happened. Both of these upward trendlines—healthcare inflation and longevity—flattened.
Spending on medical care still consumes roughly 17% of the U.S. GPD—the same as 2010. Meanwhile, U.S. life expectancy in 2020 (using pre-pandemic data) was 77.3 years—about the same as in 2010 when the number was 78.7 years.
How did these plateaus occur?
Skimping On U.S. Healthcare
With the passage of the Affordable Care Act of 2010, healthcare policy experts hoped expansions in health insurance coverage would lead to better clinical outcomes, resulting in fewer heart attacks, strokes and cancers. Their assumption was that fewer life-threatening medical problems would bring down medical costs.
That’s not what happened. Although the rate of healthcare inflation did, indeed, slow to match GDP growth, the cost decreases weren’t from higher-quality medical care, drug breakthroughs or a healthier citizenry. Instead, it was driven by skimping.
To illustrate this, here are three ways that skimping reduces medical costs but worsens public health:
1. High-Deductible Health Insurance
In the 20th century, traditional health insurance included two out-of-pocket expenses. Patients paid a modest upfront fee at the point of care (in a doctor’s office or hospital) and then a portion of the medical bill afterward, usually totaling a few hundred dollars.
Both those numbers began skyrocketing around 2010 when employers adopted high-deductible insurance plans to offset the rising cost of insurance premiums (the amount an insurance company charges for coverage). With this new model, workers pay a sizable sum from their own pockets—up to $7,050 for single coverage and $14,100 for families—before any health benefits kick in.
Insurers and businesses argue that high-deductible plans force employees to have more “skin in the game,” incentivizing them to make wiser healthcare choices.
But instead of promoting smarter decisions, these plans have made care so expensive that many patients avoid getting the medical assistance they need.Nearly half of Americans have taken on debt due to medical bills. And 15% of people with employer-sponsored health coverage (23 million people) have seen their health get worse because they’ve delayed or skipped needed care due to costs.
And when it comes to Medicaid, the government-run health program for individuals living in poverty, doctors and hospitals are paid dramatically lower rates than with private insurance.
As a result, even though the nation’s 90 million Medicaid enrollees have health insurance, they find it difficult to access care because an increasing number of physicians won’t accept them as patients.
2. Cost Shifting
Unlike with private insurers, the U.S. government unilaterally sets prices when paying for healthcare. And in doing so, it transfers the financial burden to employers and uninsured patients, which leads to skimping.
To understand how this happens, remember that hospitals pay the same amount for doctors, nurses and medicines, regardless of how much they are paid (by insurers) to care for a patient. If the dollars reimbursed for some patients don’t cover the costs, then other patients are charged more to make up the difference.
Two decades ago, Congress enacted legislation to curb federal spending on healthcare. This led Medicare to drastically reduce how much it pays for inpatient services. Consequently, private insurers and uninsured patients now pay double and sometimes triple Medicare rates for hospital services, according to a Kaiser Family Foundation report.
These higher prices generate heftier out-of-pocket expenses for privately insured individuals and massive bills for the uninsured, forcing millions of Americans to forgo necessary tests and treatments.
3. Delaying, Denying Care
Insurers act as the bridge between those who pay for healthcare (businesses and the government) and those who provide it (doctors and hospitals). To sell coverage, they must design a plan that (a) payers can afford and (b) providers of care will accept.
When healthcare costs surge, insurers must either increase premiums proportionately, which payers find unacceptable, or find ways to lower medical costs. Increasingly, insurers are choosing the latter. And their most common approach to cost reduction is skimping through prior authorization.
Originally promoted as a tool to prevent misuse (or overuse) of medical services and drugs, prior authorization has become an obstacle to delivering excellent medical care. Insurers know that busy doctors will hesitate to recommend costly tests or treatments likely to be challenged. And even when they do, patients weary of the wait will abandon treatment nearly one-third of the time.
This dynamic creates a vicious cycle: costs go down one year, but medical problems worsen the next year, requiring even more skimping the third year.
The Real Cost Of Healthcare Skimping
Federal actuaries project that healthcare expenses will rise another $3 trillion over the next eight years, consuming nearly 20% of the U.S. GDP by 2031.
But given the challenges of ongoing inflation and rapidly rising national debt, it’s more plausible that healthcare’s share of the GDP will remain at around 17%.
This outcome won’t be due to medical advancements or innovative technologies, but rather the result of greater skimping.
For example, consider that Medicare decreased payments to doctors 2% this year with another 3.3% cut proposed for 2024. And this year, more than 10 million low-income Americans have lost Medicaid coverage as states continue rolling back eligibility following the pandemic. And insurers are increasingly using AI to automate denials for payment.
Currently, the competitive job market has business leaders leery of cutting employee health benefits. But as the economy shifts, employees should anticipate paying even more for their healthcare.
The truth is that our healthcare system is grossly inefficient and financially unsustainable. Until someone or something disrupts that system, replacing it with a more effective alternative, we will see more and more skimping as our nation struggles to restrain medical costs.
Late last week, the Congressional Budget Office (CBO) released its analysis of the Center for Medicare and Medicaid Innovation (CMMI)’s spending outlays, revealing that in its first decade of operations it produced a $5.4B net increase in federal spending instead of a projected $2.8B reduction.
Moreover, CBO revised its CMMI projection for 2021-2030 from a $77.5B net spending reduction to a $1.3B increase, predicting CMMI may only begin to generate annual savings in 2031. CBO says its updated projections largely reflect revised expectations on CMMI’s ability to identify and scale models that actually reduce Medicare spending.
CMMI was created by the Affordable Care Act (ACA) in 2010 to test new payment models and other initiatives for reducing the federal government’s healthcare costs, but of the nearly 50 models it has run, only four have become permanent programs.
The Gist: This critical report confirms what many in the healthcare world already believed: the ACA’s value-based care initiatives have largely struggled to reduce Medicare spending.
There are plenty of policy factors to blame, including the lack of mandatory participation for providers and conflicting incentives across care models, but one factor left out of the CBO report is CMMI’s disproportionate emphasis on accountable care organizations (ACOs) to produce meaningful cost savings, even as years of data proved otherwise.
ACOs are designed to reduce spending primarily through utilization management, but research has shown that prices, not utilization, are responsible for the US’s high medical spend relative to other countries.
While CMMI’s mission is still laudable and important, the center must make good on its 2021 “strategic refresh” if it hopes to continue receiving Congressional support.