The February 14th deadline for healthcare workers to receive their first dose of the COVID vaccine does not appear to have significantly worsened the hospital staffing crisis, even in rural hospitals. But the mandate hasn’t necessarily meant that all healthcare workers are now vaccinated, as some hospitals reported approving a flurry of medical and religious exemptions to avoid staff departures.
The Gist: Just as when states and early-adopter health systems enforced healthcare worker vaccine mandates last year, COVID vaccine uptake jumped just ahead of the federal deadline.
After months of challenges, we may finally be moving beyond debates over healthcare worker vaccine requirements. And as hospitalizations from the Omicron wave continue to decline, most states and health systems are not planning to implement booster requirements.
The website for the group Physicians for Informed Consent (PIC) reads like an apolitical, educational resource that provides information on vaccines and why they shouldn’t be government-mandated. Its mission is “that doctors and the public are able to evaluate the data on infectious diseases and vaccines objectively, and voluntarily engage in informed decision-making about vaccination.”
The group’s accompanying social media accounts, however, tell a different story. On PIC’s Facebook, Twitter, Instagram, and LinkedIn feeds, you’ll find post after post about reasons to be scared of vaccines – especially for children – often highlighting selective portions of scientific research that contain vaccination risks.
Who’s Behind PIC?
The group was founded in 2015 after California passed a law that prohibited the use of personal belief exemptions from vaccinations required for children to attend any public or private school in the state.
Three years later, the number of waivers issued by doctors to parents seeking medical exemptions for their children tripled. As a result, another law was passed in 2019, cracking down on the inappropriate use of medical exemptions.
The group’s founder, Shira Miller, MD, is a concierge integrative medicine doctor based in Los Angeles, specializing in menopausal care. On her own Twitter profile, she describes herself as “Facebook’s Most Popular Menopause Doctor.”
Miller earned her medical degree in 2002 from Technion-Israel Institute of Technology in Haifa, Israel, and has reportedly been working as a concierge physician since 2010.
PIC’s leadership team also includes 20 physicians from a wide range of specialties, most of whom, like Miller, don’t specialize in infectious diseases.
Among its leaders is Paul Thomas, MD, an Oregon-based pediatrician. Thomas, who is listed as one of PIC’s founding directors, was issued an emergency suspension order of his medical license in 2021 by the state medical board, in which they cited at least eight cases of alleged patient harm. In line with PIC’s philosophy, Thomas maintains that he isn’t “anti-vax” – he’s pro-informed-consent.
Also on the team is Jane Orient, MD, internist and executive director of the Association of American Physicians and Surgeons (AAPS), a group that also opposes vaccine mandates. Orient received her medical degree from Columbia University and currently practices in Arizona. In 2020, the AAPS sued the federal government for withholding its stockpile of hydroxychloroquine from COVID patients, despite research showing that the drug is ineffective. The complaint was dismissed in September 2021.
Doug Mackenzie, MD, a plastic surgeon who graduated from Johns Hopkins University of Medicine, is PIC’s treasurer. He has previously identified himself as an “ex-vaxxer” rather than an anti-vaxxer when speaking on a panel in 2019.
The only RN on the team is Tawny Buettner. After California mandated vaccinations for healthcare workers, Buettner organized a protest outside of her place of work, Rady Children’s Hospital in San Diego; she later sued the hospital after she was dismissed from her job. According to the complaint, Buettner and the 36 other plaintiffs alleged that their requests for religious exemptions from the COVID-19 vaccine were all denied.
Kenneth Stoller, MD, also listed on the leadership team, graduated from the American University of the Caribbean School of Medicine and completed pediatric residency training at the University of California Los Angeles. Stoller was disciplined in 2019 for doling out medical exemptions to children without adequate evidence. According to state records, his license in California has since been revoked; he currently holds a medical license in New Mexico.
What’s PIC?
The most notable physician groups accused of spreading COVID-19 misinformation since the vaccine rollout have been affiliated with right-wing media, if not overtly proclaiming conservative, anti-vaccination beliefs.
For example,America’s Frontline Doctors, a group notorious for its support of hydroxychloroquine as a treatment for COVID-19, has made its values well-known. The group’s founder, Simone Gold, MD, JD, was arrested for participating in the Jan. 6 capitol riot and has openly opposed mask-wearing. Similarly, physician leaders of theFront Line COVID-19 Critical Care Alliance, known for promoting the use of ivermectin to treat COVID-19, tout their appearances on the ultra-conservative Newsmax on the website’s homepage.
PIC wants to be different. The group’s focus, according to its general counsel Greg Glaser, JD, of Copperopolis, California, is on the “authoritative citations that show, or calculate, the risks [of vaccines] to the public,” he told MedPage Today.
“We are pro-informed consent, pro-ethics, pro-health. PIC is not anti-vaccine, and PIC is not pro-vaccine – PIC is neutral,” Glaser said on behalf of the group.
In August 2021, Glaser submitted an amicus brief to the Supreme Court PIC’s behalf, arguing against the implementation of vaccine mandates. The document claims that “government statements confirm there is no evidence that COVID-19 vaccines prevent the spread of SARS-CoV-2 or COVID-19,” ignoring the breadth of existing literature that says otherwise.
As COVID-19 cases fall and hospitals tiptoe out from yet another surge, the nation is left collectively asking one major question: What comes next?
By now, health experts have made it clear COVID-19 will always be around in some capacity but have stressed uncertainty about the potential scope and severity of future surges.
While difficult to predict what the pandemic’s next act could look like, several potential scenarios have emerged in recent months.
Below are four possible paths the pandemic could take in the future, as outlined by physicians, epidemiologists and global health officials:
1. Delta rebound. Delta has seemingly fallen out of the collective pandemic lingo amid omicron’s dominance in recent months, though there is still a chance delta — thought to be the deadliest strain thus far — makes a comeback.
In a Jan. 24 op-ed for The Washington Post, Ashish Jha, MD, dean of Brown University’s School of Public Health in Providence, R.I., said “It is possible, though unlikely, that the delta variant returns and co-circulates with omicron in different populations, contributing to ongoing infections and hospitalizations.”
It’s important to note that delta is still dominant in some parts of the world, health experts toldThe Atlantic, adding that while unlikely, there is a chance it could morph into something that catches up with omicron, allowing the two to tag-team — a dangerous combination given delta’s brutality and omicron’s transmissibility.
2. COVID-19 may become a seasonal virus. Dr. Jha said this scenario is likely, whether delta makes a comeback or not.
“That means we are likely to see surges in Southern states this summer (as people there spend more time indoors) and in Northern states next fall and winter as the weather turns cold again,” he wrote in a Jan. 24 op-ed for The Washington Post.
Emerging evidence suggests COVID-19 may be a seasonal disease, though the research is still preliminary. A July 2021 study from the University of Pittsburgh projected a seasonal COVID-19 pattern in North America with three repeating waves: one starting in New England in the spring, the second starting in the South in the summer, and the third kicking off in the Dakotas in the fall. Based on these findings, researchers predicted the U.S. would see a summer 2021 wave in the South and a fall 2021 wave in North-Central states, which is similar to what happened with the delta and omicron surges. As of November 2021, the study had not been peer reviewed.
3. A new variant emerges. If there’s one thing on this list that’s near certain, it’s that there will be new variants in the future. Global health officials have said they expect future variants to be even more transmissible than omicron.
“Omicron will not be the last variant that you will hear us talking about,” Maria Van Kerkhove, PhD, the World Health Organization’s technical lead on COVID-19, said Jan. 25. “The next variant of concern will be more fit, and what we mean by that is it will be more transmissible, because it will have to overtake what is currently circulating.”
Health officials aren’t so much concerned about the emergence of new variants themselves but whether they will cause more or less disease severity. WHO officials have warned against assuming the virus will become milder as it continues to mutate.
“There is no guarantee of that,” Dr. Van Kerkhove said. “We hope that is the case, but there is no guarantee of that and we can’t bank on it,” she added, emphasizing the importance of interventions such as ramping up global vaccination coverage to prevent the emergence of new variants.
Health experts are also concerned white-tailed deer may become a reservoir for the virus to mutate and spread to other animals or back to humans in the form of a new variant.
“This is a top concern right now for the United States,” said Casey Barton Behravesh, who directs the CDC’s One Health Office, which focuses on connections among human, animal and environmental health. “If deer were to become established as a North American wildlife reservoir — and we do think they’re at risk of that — there are real concerns for the health of other wildlife species, livestock, pets and even people,” she told The New York Times.
Preliminary findings recently found white-tailed deer on New York’s Staten Island infected with omicron, the first time the strain has been detected in wild animals in the U.S. Scientists are still exploring a number of questions regarding the virus’s spread among deer, such as how they contract the virus, how the pathogen might mutate inside the host, and whether deer could pass the virus back to humans.
4. The omicron subvariant may spread globally, prolonging the current COVID-19 surge in some parts of the world.
Research shows BA.2 is more transmissible than BA.1, the original omicron strain, though there is no evidence to suggest the subvariant causes more severe illness. The WHO said it expects cases of the omicron subvariant to increase globally due to its growth advantage over BA.1.
“We expect to see BA.2 increasing in detection around the world,” Dr. Kerkhove said during a Feb. 8 media briefing.
In late January, Nathan Grubaugh, PhD, an epidemiologist at the Yale University School of Public Health in New Haven, Conn., toldThe New York Times he was “fairly certain” the subvariant will become dominant in the U.S. but is unclear on “what that would mean for the pandemic.”
The BA.2 variant could spur a new surge, but it’s more likely that U.S. cases will continue to decrease, according to Dr. Grubaugh. If anything, the variant may simply slow the decline.
Overall, most experts told the Times that BA.2’s presence would not significantly alter the course of the pandemic, and so far, data backs this up. COVID-19 cases have been falling nationwide since peaking in mid-January, and modeling from Rochester, Minn.-based Mayo Clinic predicts this trend will continue over the next 14 days.
The weekly number of BA.2 sequences identified in the U.S. has also fallen since mid-January, according to a Feb. 11 U.K. Health Security Agency’s report. The U.S. confirmed 191 BA.2 sequences in the week of Jan. 17, which fell to 116 in the week of Jan. 24. In the week of Jan. 31, just four sequences were confirmed, according to supplemental data from the report.
Data from federal, state, and local health agencies show COVID-19 case, hospitalization, and death rates are much lower for vaccinated Americans than they are for the unvaccinated.
The first week of December 2021, when Omicron was first detected in the US, unvaccinated adults were nearly 25 times more likely to be hospitalized than vaccinated adults. While Omicron caused a big spike in COVID-19 cases, vaccinated people continued to be less likely to be hospitalized than the unvaccinated.
In King County, Wash., which includes Seattle, unvaccinated people were 13 times more likely to be hospitalized for coronavirus since December than people who were fully vaccinated.
New York City was one of the first areas in the US to get hit with Omicron. During the week ending January 15, 0.6% of all unvaccinated people were hospitalized with COVID-19 , compared with 0.02% of all vaccinated people.
These two areas have some of the most up-to-date data that illustrates the differences in susceptibility and severity of coronavirus based on vaccination status. But other state and local health agencies as well as the Centers for Disease Control and Prevention (CDC) also provide data that shows vaccine effectiveness.
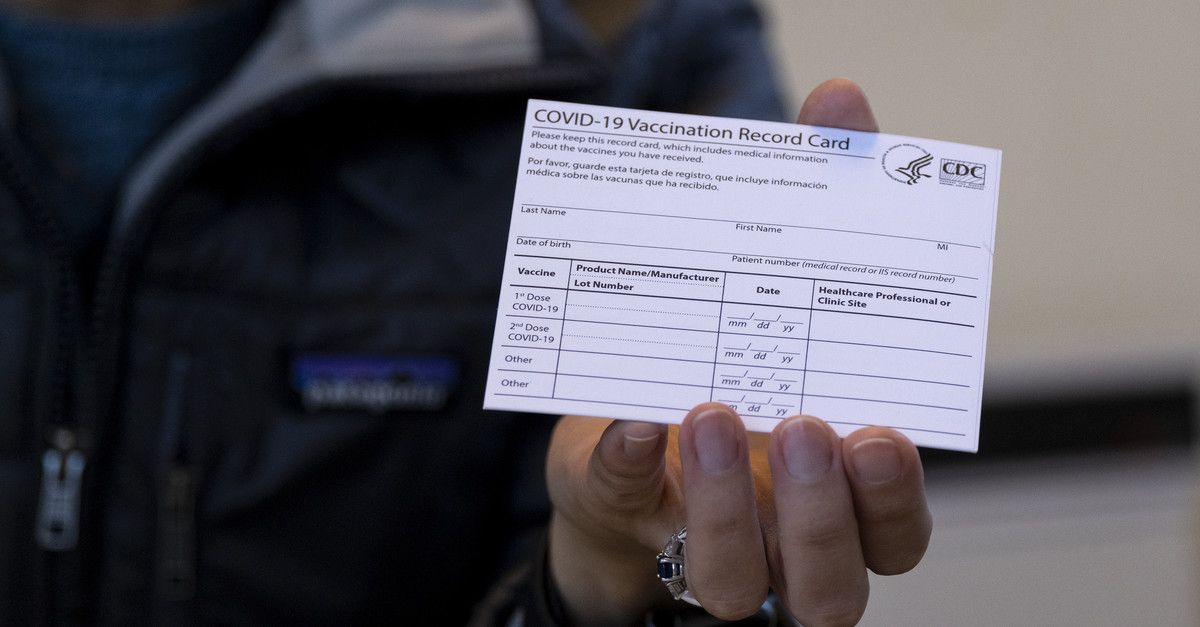
As of January 26, 210 million Americans, or 64% of the population, were considered fully vaccinated after completing the initial series of COVID-19 shots. Twenty-six percent of Americans had received a booster dose.
National data isn’t as recent but shows lower hospitalization risks among the boosted.
CDC data compiled from hospitals in 12 states shows that, in the week before Christmas, unvaccinated people ages 50 to 64 were 32 times more likely to be hospitalized with COVID-19 than people in the age range who got a booster shot. They were eight times more likely to be hospitalized with COVID-19 than fully vaccinated people without a booster.
Unvaccinated people 65 and older were about 50 times more likely to be hospitalized than those who were fully vaccinated and received a booster.
More recent data from across the country suggests vaccinated people continue to experience lower hospitalization rates.
Georgia and North Dakota are two states publishing recent data on hospitalizations for people who have received a booster shot.
These comparisons do not account for age, so they don’t directly show the effectiveness of boosters. But the available data suggests vaccinated people are hospitalized at lower rates than unvaccinated people, just like before the Omicron wave.
In the first week of December, the combination of Georgia’s unvaccinated population and those receiving only one dose of the vaccine were 10 times more likely to be in a hospital with COVID-19 than the boosted population.
Georgia counts anyone in a hospital who tests positive for COVID-19 as a COVID-19 hospitalization.
Hospitalization rates in the state increased for everyone regardless of vaccination status during the Omicron wave. But the gap between the boosted population and the unvaccinated or partially vaccinated remained.
As of mid-January, the weekly hospitalization rate for Georgia’s booster group was a third of the rate for the combined unvaccinated and not fully vaccinated population. As of January 31, 48% of Georgians were not fully vaccinated, while 17% had received a booster.
During the same period in North Dakota, unvaccinated and partially vaccinated people were about twice as likely to be hospitalized with COVID-19 compared with the vaccinated. The hospitalization gap was three times greater for those with boosters.
Several other states published data on hospitalizations through mid-January. They all show vaccinated Americans at much lower risk.
Covid-19 death rates in the United States are “eye-wateringly” high compared with other wealthy nations—a problem that several health experts say underscores the shortfalls of the country’s pandemic response.
U.S. Covid-19 death rates exceed those of other wealthy nations
According to CDC data, over 880,000 Americans have died from Covid-19 since the beginning of the pandemic—a death toll greater than that of any other country. And during the current omicron wave, Covid-19 deaths are now greater than the peak number seen during the delta wave and more than two-thirds as high as record numbers seen last winter before vaccines were available, the New York Times reports.
Moreover, since Dec. 1, when omicron was first detected in the United States, the proportion of Americans who have died from Covid-19 has been at least 63% higher than other large, wealthy countries, including Britain, Canada, France, and Germany, according to a Times analysis of mortality figures.
Currently, the daily Covid-19 death rate in the United States is nearly double that of Britain and four times that of Germany. The only large European countries to surpass the United States’ Covid-19 death rates have been the Czech Republic, Greece, Poland, Russian, and Ukraine—all of which are less wealthy nations where the most effective treatments may be limited.
“Death rates are so high in the States—eye-wateringly high,” said Devi Sridhar, head of the global public health program at the University of Edinburgh. “The United States is lagging.”
Similarly, Joseph Dieleman, an associate professor at the University of Washington, said the United States “stands out” with its high Covid-19 death rate. “There’s been more loss than anyone wanted or anticipated,” he said.
Vaccination shortfalls plague the U.S.
Lagging Covid-19 vaccination rates among Americans likely contributed to the country’s outsized death toll compared with other nations, several health experts said.
Currently, around 64% of the U.S. population has been fully vaccinated. However, several peer countries, including Australia (80%), Canada (80%), and France (77%), have achieved higher vaccination rates.
Unvaccinated people make up the majority of hospitalized Covid-19 patients, according to the Times, but lagging vaccination and booster rates among vulnerable groups, such as older Americans, has also led to increased hospitalizations.
Around 12% of Americans ages 65 and older are not fully vaccinated, and among those who are fully vaccinated, 43% still have not received a booster shot, leaving them with waning immunity against the omicron variant. In comparison, only 4% of Britons ages 65 and older are not fully vaccinated, and only 9% have not had a booster shot.
“It’s not just vaccination—it’s the recency of vaccines, it’s whether or not people have been boosted, and also whether or not people have been infected in the past,” said Lauren Ancel Meyers, director of the University of Texas at Austin’s Covid-19 modeling consortium.
Similarly, former FDA Commissioner Scott Gottlieb said that the United States‘ lagging vaccination rates compared to the U.K.’s, particularly for boosters, may be due to “protracted wrangling” that “may have sowed confusion, sapping consumer interest.”
How the U.S. could fare in future Covid-19 waves
According to some scientists, the gap between the United States and other wealthy nations may soon begin to narrow. Although U.S. vaccination rates have been slow, the delta and omicron waves have infected so many people that overall immunity against the coronavirus has increased—which could potentially help blunt the effect of future waves.
“We’ve finally started getting to a stage where most of the population has been exposed either to a vaccine or the virus multiple times by now,” said David Dowdy, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health. “I think we’re now likely to start seeing [American and European Covid-19 death rates] be more synchronized going forward.”
However, other experts noted that the United States has other disadvantages that could make future Covid-19 waves difficult. For example, many Americans have chronic health problems, such as diabetes and obesity, that increase the risk of severe Covid-19 outcomes.
Overall, health experts said the impact of future Covid-19 waves will depend on what new variants emerge, as well as what level of death people decide is tolerable.
“We’ve normalized a very high death toll in the U.S.,” said Anne Sosin, who studies health equity at Dartmouth University. “If we want to declare the end of the pandemic right now, what we’re doing is normalizing a very high rate of death.”
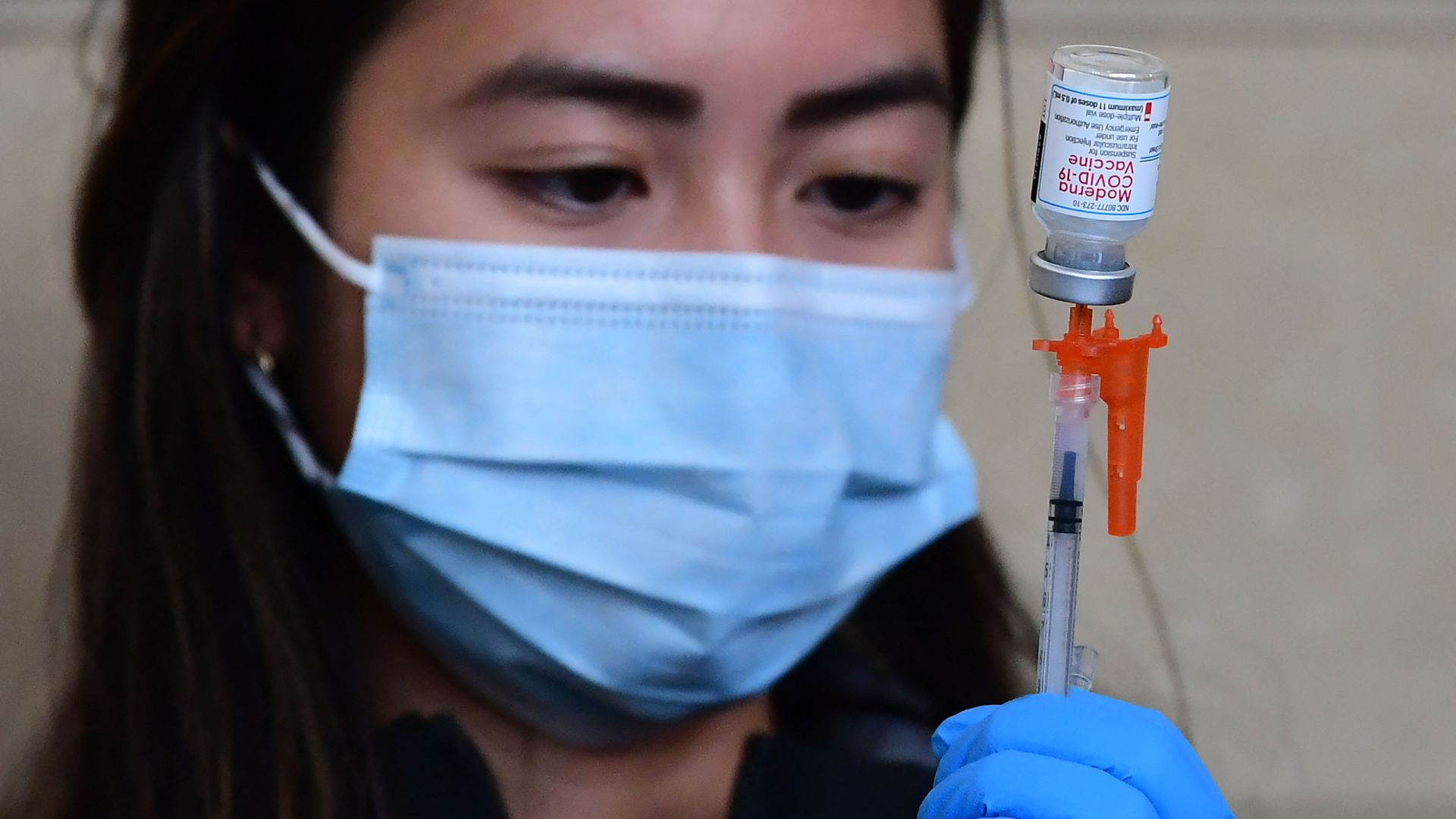
The Food and Drug Administration fully approved Moderna’s mRNA COVID-19 vaccine on Monday, saying it meets its safety and manufacturing requirements.
Why it matters: Moderna’s vaccine, which will now be marketed as Spikevax, is the second coronavirus vaccine to receive full approval after the FDA approved Pfizer-BioNTech’s vaccine in August.
Hundreds of millions of doses of Moderna’s vaccine have already been administered in the U.S. under the FDA’s emergency use authorization.
What they’re saying: “The public can be assured that Spikevax meets the FDA’s high standards for safety, effectiveness and manufacturing quality required of any vaccine approved for use in the United States,” acting FDA Commissioner Janet Woodcock said in a statement.
“The totality of real-world data and the full [Biologics License Application] for Spikevax in the United States reaffirms the importance of vaccination against this virus,” Moderna CEO Stéphane Bancel said.
The big picture: The rise of the Omicron variant forced vaccine makers to reevaluate the effectiveness of their vaccines, which were developed based on eaarlier forms of the virus.
Studies show that Moderna and Pfizer-BioNTech’s vaccines still overwhelmingly prevent severe disease and hospitalizations, especially when the first two doses are reinforced with a booster shot.
CMS is preparing to enforce its vaccine mandate for health care workers, but the agency may not have an accurate count of how many remain unvaccinated—and five health systems are pushing back on federal hospital vaccination data, calling it “extremely erroneous,” Cheryl Clark writes for MedPage Today.
Background
The Supreme Court earlier this month ruled that CMS could require most health care workers to be vaccinated against Covid-19—but U.S. officials currently do not know exactly how many workers remain unvaccinated, primarily due to a lack of reliable immunization data.
At the end of December, CDC reported that 77.6% of hospital workers were fully vaccinated. However, that figure was based on data from only about 40% of the nation’s hospitals. Hospitals currently send vaccination data to the agency on a voluntary basis, but beginning May 15, they will be required to send in weekly data, just like nursing homes have been.
According to Janis Orlowski, chief health care officer at the Association of American Medical Colleges (AAMC), CDC’s data is likely representative of providers nationwide, as an AAMC survey of 125 academic hospitals found similar results. More than 99% of doctors and close to 90% of nurses were vaccinated, she said, but vaccination rates dropped off to the 30% to 40% range for those in more operational roles, such as transportation and food service workers.
Is federal vaccination data for hospitals inaccurate?
Further adding to the confusion about health care workers’ vaccination rates are potential inaccuracies in a federal database that tracks Covid-19 vaccinations among workers in hospitals across the country. According to five health systems listed as having the highest numbers of unvaccinated workers, the database is “extremely erroneous,” Clark writes.
In the database, Adventist Health Orlando (AHO) is shown to have 18,576 unvaccinated workers, 637 partially vaccinated workers, and 25,253 fully vaccinated workers. However, Jeff Grainger, director of external communications for AdventHealth in Central Florida, said those numbers weren’t possible since the organization “[doesn’t] have 44,000 employees in one hospital.” He added that 96% of AHO’s team members have already complied with CMS’ mandate.
The University of Illinois Hospital (UI) was listed in the database as having 12,049 unvaccinated workers and 272 partially vaccinated workers. Jacqueline Carey, from health system’s public affairs department, disputed these numbers, saying UI had 6,530 workers as of Jan. 19, with 96% of them fully vaccinated. The remainder were either partially vaccinated or had approved exemptions.
The hospital with the third highest number of unvaccinated workers was Mount Sinai Hospital, Clark writes, but Lucia Lee, a hospital spokesperson, said the federal data was inaccurate. According to Lee, Mount Sinai Health System, of which the hospital is a part, has vaccinated 99% of its more than 43,000 employees.
A representative for Ochsner Medical Center, which is listed as having the fourth highest number of unvaccinated workers, also pushed back on the statistics in the database. Currently, 99.57% of Ochsner’s over 34,000 employees are compliant with its Covid-19 policy, with 95% of workers Ochsner Health and Ochsner LSU Health Shreveport fully vaccinated.
Finally, Kena Lewis, a spokesperson for Orlando Regional Medical Center, said that federal data showing the hospital has 44,154 workers is inaccurate. Instead, she said the hospital is one of 10 in the Orlando network, which has 23,709 total employees. Although Lewis did not give the health system’s vaccination rates, she said it “continues to review the guidelines regarding Covid-19 vaccination requirements for health care organizations and will take appropriate steps.”
Although it is not clear why there are discrepancies between the federal data and what these health systems are reporting regarding vaccination rates, there are some potential explanations, Clark writes.
According to Carey, the federal database only includes vaccination information provided by the UI health system and employee health services. This means that vaccinations workers received elsewhere, such as through a personal provider or pharmacy, are not included in the data, and they will show up as being unvaccinated.
Separately, a spokesperson for another of the five organizations told Clark on background that short-term nursing staff contracted through agencies may show up as unvaccinated in the federal database. Although the agencies assure employers the nurses are vaccinated, hospitals do not independently verify this information.
Welcome to Wednesday’s Overnight Health Care, where we’re following the latest moves on policy and news affecting your health. Subscribe here: thehill.com/newsletter-signup.
Masks come to the Super Bowl: Fans attending the big game next month will be given KN95 masks.
Despite omicron being less severe on average, the sheer number of cases has driven deaths past the peak from last year’s delta surge.
The average number of U.S. COVID-19 deaths this week surpassed the height of the delta surge earlier this fall and is at its highest point since last winter, when the nation was coming out of the peak winter surge.
The seven-day average of deaths hit 2,166 on Monday, according to the latest data from the Centers for Disease Control and Prevention (CDC). Average daily deaths in mid-September before the omicron variant was discovered peaked at around 1,900.
While increasing evidence shows omicron may be less likely to cause death or serious illness than delta, the sheer infectiousness and the speed at which it spreads has overwhelmed hospitals, primarily with people who have not been vaccinated.
The U.S. saw the highest numbers of deaths in the pandemic just over a year ago, before vaccines were widely available, when the daily average reached 3,400. The last time the U.S. topped 2,000 deaths was last February, as the country was slowly coming down from the January peak.
Caution urged: Infections are falling in states that were hardest hit earlier, as well as broadly across the nation. Hospitalizations are also falling, but deaths are a lagging indicator and are still increasing. CDC Director Rochelle Walsenky said deaths have increased about 21 percent over the past week.
The fact that the omicron variant tends to cause less severe disease on average also helped avoid an even greater crisis that would have occurred if it was as severe as the delta variant.
Long COVID-19 has had an air of mystery around it for months. Doctors have struggled to explain or understand why some people who contract COVID-19 end up having lingering symptoms like fatigue, difficulty thinking clearly, or shortness of breath weeks or even months later.
A new study published in the journal Cell helps shed some light on the condition, for the first time identifying four factors that can help predict whether someone will develop long COVID-19.
“Being able to identify the factors that can cause the disease, cause the chronic condition, is the first step towards defining that it actually is a condition that can be treatable,” Jim Heath, president of the Institute for Systems Biology in Seattle, and an author of the study, said in an interview. “And then some of these factors also are in fact the kind of things one can imagine developing treatments for.”
The most important factor the study identified in predicting long COVID-19 is the presence of certain kinds of antibodies called autoantibodies, which mistakenly attack healthy parts of the body. Autoantibodies are associated with autoimmune diseases, like lupus, where your immune system attacks your own body.
But someone does not have to have an autoimmune disease to have autoantibodies present and be at higher risk for long COVID-19, Heath said.
“Most people that have autoantibodies don’t really know it,” he said. “They’re what you call subclinical … maybe you have a risk of some autoimmune disease but it hasn’t developed.”
Still, he said one practical application of the study is that lupus treatments could be “worth exploring” as treatments for long COVID-19.
The second factor that can lead to long COVID-19 is the reactivation of a different virus called Epstein-Barr Virus (EBV), which is extremely common, infecting up to 90 percent of people at some point, and often causes only mild symptoms.
The virus usually becomes inactive in the body following the initial infection, but it can be reactivated when someone gets COVID-19, helping lead to long COVID-19 symptoms.
Heath said EBV could become reactivated when the immune system is distracted by fighting COVID-19.
“It could be that the large distraction that’s COVID-19 infection is taking that attention away,” he said.
The third factor identified is how much of the virus that causes COVID-19, officially called SARS-Cov-2, is present in the blood, known as the “viral load.”
This factor along with the role of EBV suggests that new antiviral drugs that fight the immediate effects of COVID-19 infection, like the Pfizer pill Paxlovid, might also be useful in treating long COVID-19.
“Two of these predictive factors are virus levels that are in the blood,” Heath said. “So that suggests that these antivirals that are being used to treat acute disease probably have a role for long COVID as well.”
The final of the four factors that can predict long COVID-19 is more easily identifiable: if a patient has Type 2 diabetes.
While these four factors are a step forward in understanding what causes long COVID-19 and helping develop treatments, the mechanism for why they are associated with long COVID-19 is still not fully clear.
“They have a flavor of mechanistic factors,” Heath said. “The actual mechanism is not clear.”
The study followed 309 COVID-19 patients, taking blood and swab samples at different points in time.
In addition, one way to likely cut the risk of long COVID-19 is vaccination. A separate study from the United Kingdom found that vaccinated people were 41 percent less likely to develop long COVID-19.
A study of 10M blood samples from active-duty military members, published in the journal Science, found that contracting the Epstein-Barr virus (EBV), best known for causing mononucleosis, was associated with a 32-fold increase in getting an MS diagnosis. While experts were cautious not to conclude that EBV causes MS, it appears to at least be a trigger. What’s left unanswered is how EBV, which is infects an estimated 90 percent of Americans by age 35, leads some to develop MS, while the vast majority do not.
The Gist:It’s rare to have such a large, well-designed epidemiological study show a definitive and clear link between two diseases. Several viruses, including EBV and the human papillomavirus (HPV), have been linked with cancer; while more research is needed, it is theoretically possible vaccines targeted at EBV could reduce the risk of multiple sclerosis and certain cancers, similar to how HPV vaccines have successfully in lowered cervical cancer risk.
And with such a large portion of the global population expected to be infected with COVID-19, it will be critical to monitor whether that virus, too, is linked to the development of other diseases years later.