At a recent dinner with my good friend and colleague Dave Blom, the former President and CEO of Ohio Health, he and I discussed the difficulties of leading and managing complex healthcare organizations in the post-Covid era.
We agreed that the leadership issues that matter most right now center around the ability of executives to possess and demonstrate an authentic emotional IQ.
Taking care of patients—in fact, taking care of communities—is not only managerially complicated but also emotionally testing.
Success cannot be achieved by technical and clinical excellence alone; rather, it must be built on a platform of an emotional IQ that is supported, valued, and shared by the entire organization.
The below list is what Dave and I settled on as the most important elements of emotional IQ for healthcare leaders today, and we think that leadership teams thatfully embrace these behaviors unlock a higher level of organizational trust, as well as corporate and managerial integrity.
–Empathy.
A leader needs to understand and share the feelings of his or her entire organization, as well as understand the difference between sympathy and empathy: sympathy is a passive emotion while empathy is an active emotion. A leader with empathy not only notes the problem but immediately moves to be of help at either the personal or organizational level, whichever is required.
–Vulnerability.
Historically, executive leadership, especially in corporate situations, has been trained and encouraged not to show emotion or weakness. But organizations are changing, and the composition of the today’s workforce is different. The patient care process is emotional in and of itself, and daily operational interactions demand a different kind of leadership—a leadership that is comfortable with both emotion and weakness.
–Humility.
Executives who show humility are willing to ask for help, and don’t insist on everything being done their way; they are quick to forgive and are known for their patience. Humility supports a collaborative and cooperative leadership model, which has at its core a heavy dose of decentralization and delegation.
I recently had dinner with my good friend and colleague, Dave Blom. For many years, Dave was the President and CEO of Ohio Health. During his tenure, Ohio Health was one of America’s most successful health systems by any measure. Dave Blom was known nationally as a calm, steady, and thoughtful hospital leader.
Dave and I were talking about the difficulties of leading and managing complex healthcare organizations in the post-Covid era. The hospital problems of finance, staffing, access, and inflation have been well itemized and documented. While the day-to-day operating problems are undeniably significant and persistent, Dave and I agreed that the hospital leadership issues that really matter right now center around the ability of hospital executives to possess and demonstrate an authentic emotional IQ to lead a diverse workforce in such difficult circumstances.
Such a realization is supported by the recognition that no matter how technically excellent they are, hospitals are just not like other organizations in other industries. Taking care of patients—in fact, taking care of communities—is not only managerially complicated but emotionally testing. Leadership gets much more complicated in the current environment.
Having moved the conversation to this point Dave and I then took on the definition of a workable and effective leadership emotional IQ. That emotional IQ is characterized by the following:
Empathy. During Covid, when leadership was challenged at every level and at every American organization, the value of personal empathy moved to the forefront. Empathy is defined as “the ability to understand and share the feelings of another.” More directly, a hospital CEO needs to understand and share the feelings of his or her entire organization. Great hospital leaders understand the difference between sympathy and empathy. Sympathy is a passive emotion, an emotion that notes and cares about a problem but doesn’t necessarily act on that problem. Empathy is an active emotion. A leader with empathy not only notes the problem but immediately moves to be of help either at the personal or organizational level, whichever is required.
Vulnerability. Vulnerability is defined as “the willingness to show emotion or to allow one’s weakness to be seen or known.” Historically, executive leadership—especially in corporate situations—has been trained and encouraged not to show emotion or weakness. But organizations are changing, and the composition of the hospital workforce is different. The patient care process is emotional in and of itself and the daily operational interaction demands a different kind of leadership—a leadership that is comfortable with both emotion and weakness.
Humility. Executives who show humility “are willing to ask for help and don’t insist on everything done their way; they are quick to forgive and are known for their patience.” Humility also reflects changing organizational ecosystems. Humility is not generally indicative or compatible with the “military command” model of leadership. It is more supportive of a collaborative and cooperative leadership model, which has at its core a heavy dose of decentralization and delegation.
As our dinner was coming to a close, we took note of two other leadership observations.
First, when you create a leadership team that fully embraces the principles of empathy, vulnerability, and humility, then that emotional IQ combination creates the highest order goal of organizational trust. All of this is exceptionally meaningful since organizational trust is more important than ever, given that it is in such short supply at all levels of American society. Dave Blom then advanced the discussion to one further point. When you gain the full value of empathy, vulnerability, and humility and you add to that the organizational trust you have established, all the principled prerequisites for establishing corporate and managerial integrity are in place. Empathy plus vulnerability plus humility equals organizational trust. And then empathy plus vulnerability plus humility plus trust equals organizational integrity.
The emotional IQ of leadership is not created by accident. It requires a hyper-aware organization at both the management and Board level. It requires governance and executive leaders who understand that hospital success cannot be achieved by technical and clinical excellence alone. That success must be built on a platform of an emotional IQ that is supported, valued, and shared by the entire hospital community.
Politicians, economists, auto industry analysts and main street business owners are closely watching the UAW strike that began at midnight last Thursday. Healthcare should also pay attention, especially hospitals. medical groups and facility operators where workforce issues are mounting.
Auto manufacturing accounts for 3% of America’s GDP and employs 2.2 million including 923,000 in frontline production. It’s high-profile sector industry in the U.S. with its most prominent operators aka “the Big Three” operating globally. Some stats:
The US automakers sold an estimated 13.75 million new and 36.2 million used vehicles in 2022.
The total value of the US car and automobile manufacturing market is $104.1 billion in 2023:
9.2 million US vehicles were produced in 2021–a 4.5% increase from 2020 and 11.8% of the global total ranking only behind China in total vehicle production.
As of 2020, 91.5% of households report having access to at least one vehicle.
There were 290.8 million registered vehicles in the United States in 2022—21% of the global market.
Americans spend $698 billion annually on the combination of automobile loans and insurance.
By comparison, the healthcare services industry in the U.S.—those that operate facilities and services serving patients—employs 9 times more workers, is 29 times bigger ($104 Billion vs. $2.99 trillion/65% of total spend) and 6 times more integral in the overall economy (3% vs. 18.3% of GDP).
Surprisingly, average hourly wages are similar ($31.07 in auto manufacturing vs. $33.12 in healthcare per BLS) though the range is wider in healthcare since it encompasses licensed professionals to unskilled support roles. There are other similarities:
Each industry enjoys ubiquitous presence in American household’ discretionary. spending.
Each faces workforce issues focused on pay parity and job security.
Each is threatened by unwelcome competitors, disruptive technologies and shifting demand complicating growth strategies.
Each is dependent on capital to remain competitive.
And each faces heightened media scrutiny and vulnerability to misinformation/disinformation as special interests seek redress or non-traditional competitors seek advantage.
Ironically, the genesis of the UAW dispute is not about wages; it is about job security as electric-powered vehicles that require fewer parts and fewer laborers become the mainstay of the sector. CEO compensation and the corporate profits of the Big Three are talking points used by union leaders to galvanize sympathizer antipathy of “corporate greed” and unfair treatment of frontline workers.
But the real issue is uncertainty about the future: will auto workers have jobs and health benefits in their new normal?
In healthcare services sectors—hospitals, medical groups, post-acute care facilities, home-care et al—the scenario is similar: workers face an uncertain future but significantly more complicated. Corporate greed, CEO compensation and workforce discontent are popular targets in healthcare services media coverage but the prominence of not-for-profit organizations in healthcare services obfuscates direct comparisons to for-profit organizations which represents less than a third of the services economy. For example, CEO compensation in NFPs—a prominent target of worker attention—is accounted differently for CEOs in investor-owned operations in which stock ownership is not treated as income until in options are exercised or shares sold. Annual 990 filings by NFPs tell an incomplete story nonetheless fodder for misinformation.
The competitive landscape and regulatory scrutiny for healthcare services are also more complicated for healthcare services. Unlike auto manufacturing where electric vehicles are forcing incumbents to change, there’s no consensus about what the new normal in U.S. healthcare services will be nor a meaningful industry-wide effort to define it. Each sector is defining its own “future state” based on questionable assumptions about competitors, demand, affordability, workforce requirements and more. Imagine an environmental scan in automakers strategy that’s mute on Tesla, or mass transit, Zoom, pandemic lock-downs or energy costs?
While the outlook for U.S. automakers is guardedly favorable, per Moody’s and Fitch, for not-for-profit health services operators it’s “unsustainable” and “deteriorating.”
Nonetheless, the parallels between the current state of worker sentiment in the U.S. auto manufacturing and healthcare services sectors are instructive. Auto and healthcare workers want job security and higher pay, believing their company executives and boards but corporate profit above their interests and all else. And polls suggest the public’s increasingly sympathetic to worker issues and strikes like the UAW more frequent.
Ultimately, the UAW dispute with the Big Three will be settled. Ultimately, both sides will make concessions. Ultimately, the automakers will pass on their concession costs to their customers while continuing their transitions to electric vehicles.
In health services, operators are unable to pass thru concession costs due to reimbursement constraints that, along with supply chain cost inflation, wipe out earnings and heighten labor tension.
So, the immediate imperatives for healthcare services organizations seem clear as labor issues mount and economics erode:
Educate workers—all workers—is a priority. That includes industry trends and issues in sectors outside the organization’s current focus.
Define the future. In healthcare services, innovators will leverage technology and data to re-define including how health is defined, where it’s delivered and by whom. Investments in future-state scenario planning is urgently needed.
Address issues head-on: Forthrightness about issues like access, prices, executive compensation, affordability and more is essential to trustworthiness.
Stay tuned to the UAW strike and consider fresh approaches to labor issues. It’s not a matter of if, but when.
PS: I drive an electric car—my step into the auto industry future state. It took me 9 hours last Thursday to drive 275 miles to my son’s wedding because the infrastructure to support timely battery charges in route was non-existent. Ironically, after one of three self-charges for which I paid more than equivalent gas, I was prompted to “add a tip”. So, the transition to electric vehicles seems certain, but it will be bumpy and workers will be impacted.
The future state for healthcare is equally frought with inadequate charging stations aka “systemness” but it’s inevitable those issues will be settled. And worker job security and labor costs will be significantly impacted in the process.
In the era of great awakening, leaders have to step up and be conscious about building trust with people they work with.
The old rules and hierarchies, that were already becoming obsolete, have now been thrown out of the window. People look for integration of work and well-being knowing that work is what you do, not a place you go to.
Opportunities are abound and excellent people have ample choices (they always had). It is high time that organizations and leaders think this through carefully to first align their own mindset to this new reality and then take conscious actions to build teams, practices and processes that are not just high-performing but also have a strong fabric of trust woven in.
Employees, after all, are volunteers who exercise their choice of working with you. Effective leadership is about making it worth for them.
Building high-trust environment means putting the human back at the center of how a business functions and building everything – purpose, culture, processes, structures, rituals, systems, tools and mindsets – around it.
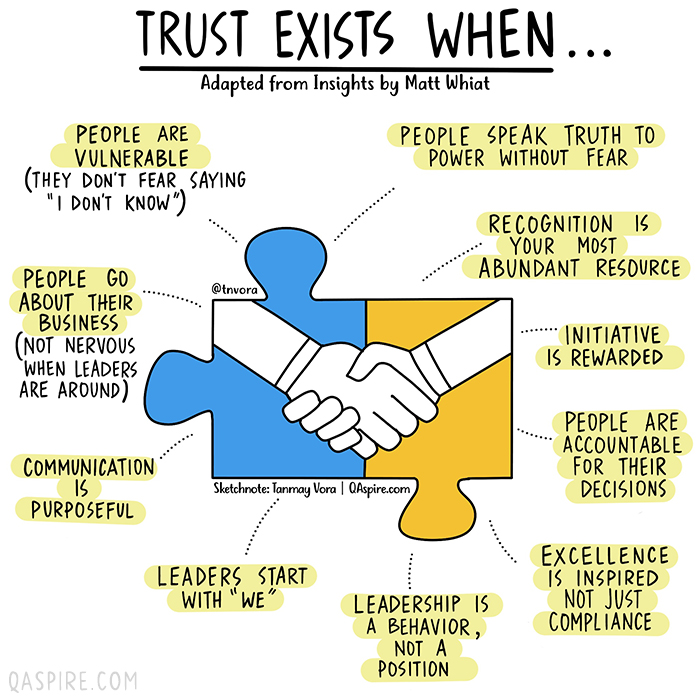
How would we know if we are working in an environment where we can trust others and that we are trusted? We can always answer this based on our intrinsic feeling but if you are a leader who is working hard to build trust, here are a few vital signs that you need to look for.