A society loses its moral compass the moment profit outweighs the value of human life.
Chomsky’s words call out the mindset that treats human survival as expendable when money is involved. He argues that ordinary language fails to describe the depth of this moral failure. His point is simple: when greed becomes more important than humanity, something fundamental has already broken.
Solitude becomes a strength when the alternative threatens your character.
When George Washington warns that it is better to be alone than in bad company, he’s reminding us that the people around us shape our values, choices, and future. Choosing solitude over harmful influences protects your integrity and keeps your path clear, steady, and self‑directed.
To kick off the new show, KFF’s Business of Health with Chip Kahn, Charles Kahn III hosts Drew Altman who explains how KFF is continually evolving to research, analyze, and lead on health policy. They discuss how the new podcast will break down the business side of health care, artificial intelligence, and what it all means for health care delivery and patients.
Cigna’s earnings tell a story Wall Street loves but its retreat from the ACA Marketplace could accelerate a system already tipping toward collapse.
Cigna reported its first-quarter 2026 results last Thursday. Like most of the other big health insurance conglomerates that have reported so far, it did a better job of meeting Wall Street’s profit expectations in the first three months of the year than it did in all of 2025.
Total revenues rose 5% to $68.5 billion. Adjusted income from operations came in at $2.1 billion, or $7.79 per share — up 12% from a year ago, though missing analyst estimates by five cents. The company raised its full-year outlook for adjusted income from operations to at least $30.35 per share. David Cordani, in what he called a “somewhat bittersweet” moment as his final quarterly earnings call as CEO, described the results as reflecting “disciplined execution, deliberate portfolio shaping and a continued focus on targeted innovation.”
That jargon didn’t impress investors. Cigna’s stock price fell $3.19 on Thursday but was up 2.76% for the week, closing Friday at $282.90.
None of that is surprising. Cigna is a well-run company by the metrics Wall Street uses to measure well-run companies. What’s worth examining is what the numbers actually reveal about how the first quarter results were achieved and – equally if not more important – what Cigna announced alongside it.
Another big exit
The biggest news from Thursday’s release and call with analysts wasn’t about earnings. Cigna will stop offering plans on the Affordable Care Act marketplaces after the 2026 plan year. The exit will affect 369,000 members across 11 states, with coverage ending January 1, 2027.
Brian Evanko, who will succeed Cordani as CEO on July 1, framed the decision as a strategic choice to exit a market where Cigna is unlikely to achieve scale. “This is small business for us today, and it’s been shrinking in recent years,” he said.
He’s right about the numbers. What he didn’t say is why it’s shrinking — and what Cigna’s exit will do to the people left behind.
Cigna is by no means the first big insurer to announce an exit from the ACA Marketplace.Aetna pulled out at the end of 2025, forcing approximately 1 million members across 17 states to find new coverage for 2026. But even that headline understates the breadth of the retreat. At the end of 2025, when Congress chose not to renew some of the tax credits that had made ACA coverage affordable for millions of Americans, a wave of smaller insurers also left:Molina Healthcare announced significant changes to its service area; HAP CareSource exited Michigan; Chorus Community Health Plan withdrew; Mountain Health CO-OP left Wyoming; Primewell Health Services exited Arkansas and Mississippi; UM Health Plan and Michigan Care ended; and Celtic/WellCare left North Carolina. Blue Cross Blue Shield terminated PPO products in Arizona. And last month, Baylor Scott & White Health Plan announced it will no longer offer marketplace plans after the end of this year, affecting approximately 100,000 enrollees in Texas.
That means that before open enrollment for 2027 coverage even begins this fall, at least half a million people — Cigna’s 369,000 plus Baylor Scott & White’s 100,000, on top of the million who lost Aetna coverage last year — will either have to scramble to find comparable coverage (at a significantly higher price) or go uninsured.
And we may not yet know the full scope. Every spring and summer, health insurers file proposed premium rates with state regulators — filings that reveal what insurers are planning for the coming year. Those rate filings typically land in May and June. The Q2 earnings season follows in July and August. Each of those moments is an opportunity for another insurer to announce what Cigna announced Thursday. The exits we know about may be the beginning, not the end.
This is not a series of isolated corporate decisions. It is the beginning of a potential death spiral, and it is already in motion.
The mechanism is straightforward. ACA sign-ups for 2026 are already down by over 1 million people compared to the same period last year — the first decline since 2020. The main reason was the December 31, 2025 expiration of the enhanced premium tax credits that were enacted during the Biden administration. For subsidized enrollees who stayed in the same plan, average net premiums rose 114%. When premiums spike, the people who leave first are the healthy ones — younger, lower-utilization enrollees who do the math, decide the cost isn’t worth it and gamble that they’ll have another year of good health. The people who stay are the ones who have no choice: the chronically ill, the older, the people who know they will need care. The marketplace is already smaller and sicker, according to consultants and insurance executives, with more consumers choosing cheaper bronze plans that carry higher out-of-pocket costs.
A smaller, sicker pool means higher claims. Higher claims mean higher premiums. Higher premiums drive out even more healthy enrollees, which makes the pool sicker and more expensive still. And that is exactly what Evanko described when he noted that Cigna’s ACA enrollment had already dropped from 446,000 to 369,000 — a 17% decline in a single year.
The insurers aren’t abandoning a failed program. They are ensuring it fails — and then leaving before it does.
I wasn’t surprised to hear that Cigna is leaving the ACA Marketplace because it has never been a big player in the individual health insurance business. Around 90% of Cigna’s health plan enrollment is in its role as a third-party administrator (TPA) for large employers. The company also has sold all of its Medicare Advantage business.
What did surprise me was the company’s other big reveal: It has put its EviCore unit, which provides prior authorization and utilization management services to health plans (not just Cigna’s), up for sale. Evanko told analysts that the industry’s prior authorization standardization push (which I wrote about last Wednesday) could “open new doors for the EviCore business, which could potentially result in a partnership or a combination with complementary industry participants.”
EviCore is the prior authorization machinery — the infrastructure through which doctors’ requests for patient care get approved, delayed, or denied. Cigna is exploring selling it, or spinning it off, at precisely the moment that prior authorization is under the most intense public and regulatory scrutiny it has ever faced.
Think about what that means. Just days after the industry announced a voluntary reform campaign to standardize the prior authorization process, Cigna said it might sell the business unit that does the prior authorizing. That tells me that the company’s executives don’t think EviCore will be able to continue contributing to Cigna’s profits.
What the numbers say — and don’t
One of the most important numbers in any health insurer’s earnings report isn’t revenue. It’s the medical loss ratio — the percentage of premium dollars actually spent on patient care. The lower the MLR, the more the company keeps.
Cigna’s MLR for Q1 2026 was 79.8%, down from 82.2% a year ago. That 240-basis-point decline is the engine behind the strong earnings performance. For every dollar Cigna collected in premiums this quarter, it paid out roughly two cents less in medical claims than it did a year ago.
The company attributes the decline primarily to the 2025 sale of its Medicare Advantage business to Health Care Services Corporation — older, costlier populations leaving the risk pool.
What no analyst asked: Is the MLR decline connected to Cigna’s prior authorization practices? The company’s own Transparency Report, published in March, claims a 15% reduction in prior authorization volume. Did tighter scrutiny on the remaining high-cost requests contribute to lower medical costs and therefore a better MLR? We don’t know because Wall Street analysts chose not to ask.
Another thing analysts didn’t explore was litigation against its PBM, Express Scripts. Evernorth — the division that encompasses Express Scripts and that now accounts for 85% of Cigna’s revenue — generated $58.4 billion in adjusted revenues, driven by specialty drug volume and biosimilar adoption. What the earnings release doesn’t mention is that Express Scripts is currently the subject of federal RICO litigation alleging the company created a Swiss entity called Ascent Health Services to divert drug rebates away from plan sponsors and patients.
On Thursday’s call, analysts asked about Evernorth’s growth trajectory, capital deployment, the EviCore strategic review, and the CEO transition. No one asked what happens to the 369,000 people who will lose their Cigna coverage on January 1. No one asked whether the cascade of ACA exits constitutes a market failure requiring a policy response. No one asked what the prior authorization denial rate was for the quarter, or how many denials were later overturned on appeal.
Those questions have answers, but Wall Street analysts don’t ask because they assume most investors have little interest in such matters. And they are right.
New data shows middle-class Americans cutting essentials, dropping coverage, and delaying care — just as Pope Leo XIV calls health care a “moral imperative.”
Pope Leo XIV (who became pope a year ago this week) isn’t just the first American pontiff—he’s also, as a Chicago native and Villanova University alum, the first leader of the Roman Catholic Church to have experienced the U.S. health care system firsthand. So it shouldn’t come as a surprise that this world spiritual leader born as Robert Prevost would use his lofty new platform to call for radical change.
“Health cannot be a luxury for the few,”Leo told a recent conference on health care inequality in Europe organized by both Catholic bishops and the World Health Organization, adding that good health care is essential for social peace.
“Universal health coverage is not merely a technical goal to be achieved; it is primarily a moral imperative for societies that wish to call themselves just,” the pope said. “health care must be accessible to the most vulnerable, then, not only because their dignity requires it but also to prevent injustice from becoming a cause of conflict.”
In less than a year on the job, the new pontiff has shown a lot of political savvy, and a knack for good timing. Leo’s endorsement of health care as a human right coincided with a couple of new, important U.S. surveys showing that both rising insurance premiums and high out-of-pocket medical bills have become the major driver of an affordability crisis that is hitting middle-class families hard.
To back this up, the leading health care non-profit KFF conducted a followup survey with more than 800 Americans who last year had been enrolled in Affordable Care Act (ACA) insurance in 2025. It found broadly that most have been struggling to pay medical bills since Congress failed late last to extend the federal subsidies that had made ACA coverage affordable for many in recent years.
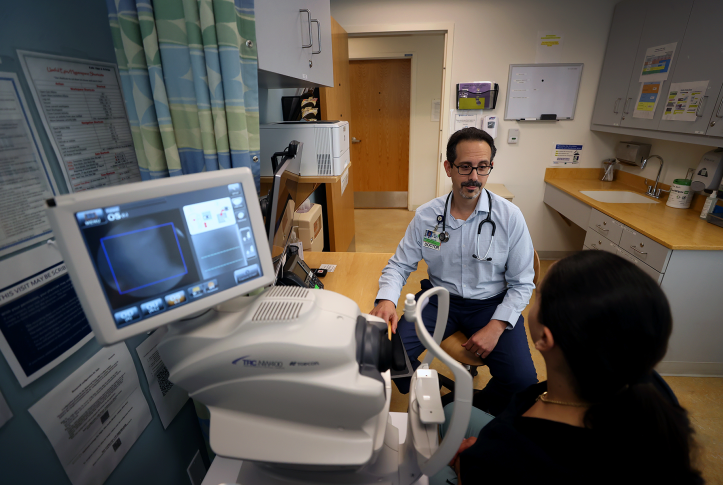
In the third episode of the HEALTH CARE un-covered Show, we take a deep dive into prior authorization’s toll — from doctors to federal policy — featuring Dr. Wendy Dean, Dr. Seth Glickman and Rep. Suzan DelBene (D-WA) on CMS’s new AI-driven WISeR model.
Most of the respondents (80%) said they were paying more now for health care than in 2025, with just over half (51%) reporting they are now spending “a lot more.” For middle-class Americans, the critical need to stay healthy has meant cutting their budget for other essentials. KFF found that a majority (55%) were reducing spending on food or other household basics, but that jumped to 62% for people getting treatment for chronic disease.
Faced with drastically higher monthly premiums, KFF found, has forced these families to make difficult, consequential choices. Some 28% switched into a different ACA plan in an effort to hold down their monthly premiums – which means much higher deductibles and thus the risk of large out-of-pocket medical expenses. Even worse, some 9% told the KFF survey that they have dropped health insurance altogether, which means they are one accident or major illness away from a financial disaster.
A 34-year-old Texan who dropped his Obamacare coverage told the KFF pollsters that the sole reason was the cost. “The prices are simply too high,” he said. “$800 a month for the absolute cheapest plan for two people. Our income is $120k, so we don’t qualify for subsidies in Texas. I don’t think we could afford our mortgage if I had to pay for health insurance.”
Another respondent reported that his “Income exceeded the subsidy limit, forcing us to pay the full cost, so we switched down to a bronze from a gold plan. Even doing that our premiums are 3 times what they were in 2025, with lower plan features and a higher deductible.”
About 22% of the KFF respondents said they are still insured, but not through the ACA Marketplace. In some cases that is because they were able to switch to an employers’ health plan or because they were now eligible for Medicare and Medicaid. But others, KFF noted, switched into different types of high-deductible plans or a cost-sharing group – solutions that often lead to considerable out-of-pocket expenses.
One 56-year-old Texas man surveyed by KFF said that as a reaction to the higher insurance premiums he would “attempt to use health care as little as possible” – with the hope that by carefully consulting with his doctors and pharmacists he would avoid paying any out-of-pocket expenses that aren’t absolutely necessary.
The U.S. announced a peace deal with Iran to which Iranian officials denied knowledge.
The strait of Hormuz opened, then closed.
The stock market soared then fell.
The President signed an Executive Order to loosen restrictions on psychedelic drugs.
Vax skeptic HHS Secretary Kennedy nominated vax supporter Erica Swartz, MD, to head the CDC.
The Centers for Medicare and Medicaid Services (CMS) announced its proposed Medicare inpatient hospital services reimbursement would increase 2.4% in fiscal 2027.
Two members of the House of Representatives announced their resignations—both due to sexual impropriety (stupidity).
And pundits were busy justifying or challenging polling showing a Trump Slump.
That’s the context for meetings this week in DC between hospital leaders and Members of Congress as part of the American Hospital Association’s Annual Meeting. Though much of the legislative agenda for hospitals has shifted to states, federal issues still matter, especially funding in the FY 2027 federal budget and appropriations to key departments and programs.
Hospitals are on the defensive in DC. On behalf of its members and in concert with its peers (FAH, CHA, AEH, et al) they’re seeking…….
Protection against 340B cuts.
Protection against site neutral payments.
Protection against competition from physician owned hospitals.
Protection against “corporate insurer” business practices.
Protection against unwanted regulation that disrupt their “normal” business practices
Protection against price gauging by drug companies.
Protection against reduced tax exemptions for not-for-profit hospitals.
Protection against funding cuts in the FY2027 federal budget.
And others.
Per AHA President and CEO: “The timing of our presence and voice in Washington is especially important this year. Health care affordability remains in the spotlight. Congress is discussing the prospects of one or two more reconciliation packages this year, even as we are asking them to examine the overreach and mitigate certain health care provisions from last year’s package. And we are 199 days from the midterm elections…” (AHA Today April 17, 2026)
The reality is this: hospitals have lost much of the good will they earned during the pandemic. Pushback by AHA against hospital price transparency, site neutral payments, 340B changes et al. have been successful. But heightened visibility about executive compensation, profitability, tax exemptions, private equity ownership concerns and for-profit venture-development has eroded Congressional favor, exacerbated nurse and physician burnout and lessened community support. AHA is aware.
In 2024, AHA and its coalition changed the name of its public-relations campaign from the Coalition to Protect America’s Health Care to Coalition to Strengthen America’s Healthcare to “… support the Coalition’s expanded capacity as a proactive, always-on organization dedicated to positively shaping public perception of hospitals and health systems, neutralizing opposition attacks, and holding corporate payers accountable for their role in delaying and denying care while driving up overall health care costs.” For AHA and most hospitals, it’s been an uphill battle against think tanks (West Health, Lown et al), investigative journalists (WSJ, NYT, STAT, Modern Healthcare) and competing interests, especially insurers and private investors, who see hospitals as protectors of the past rather than designers of healthcare’s future.
To restore trust and garner good will among employees, employed physicians, local and national employers, elected officials and community leaders, hospital leaders in DC should engage Congress in several areas usually not discussed:
Proactive education targeted to key constituents explaining how hospitals operate including actual costs, AI applications, et al and notable inefficiencies. Asking for money or regulatory relief is not enough. The public’s ignorant about how hospitals operate!
Long-range planning: Hospital boards tend to plan for NOW and NEAR to but spend inadequate time on FAR. Understanding long-term changes in clinical care, technology, regulatory and economic realities are keys to preparedness. And, like capital and facility plans, executive compensation should be linked directly to organizational readiness for long-term changes along with short-term financials). Long-term planning is not a luxury or distraction; it’s necessary.
Systemness: Hospitals should lead in the design of local/regional “systems of health” that provide a full range of needed health services affordably, rationalizes resources appropriately, is connected includes health, social services and funding programmatically. They’re the logical partner with government to integrate health and social services and, as a result, reduce fragmentation and waste. No excuses.
Workforce: Hospitals should modernize workforce plans to maximize technology-enabled consumer self-care, expand mid-level opportunities, facilitate AI-enabled administrative and clinical process improvements and compensate based on merit and performance.
Consumers including patients: Hospitals and AHA should embrace “healthcare consumerism” actualize its centricity in interactions with individuals who use its services. Competition in a value-based system of health depends on customized engagement with consumers.
Positioning: And hospitals must temper the “blame and shame” game against insurers, drug companies and demonstrate leadership in affordability, administrative waste reduction and optimal resource rationalization. Being their target is understandable: hospitals are 31% of direct spending and, with employed physicians, ancillaries and diversified interests, responsible for at least 55% of the U.S. health economy.
I acknowledge hospitals are uniquely complex organizations—labor intense, capital intense and highly regulated by states and the federal government. Events like last week’s add to uncertainty about their future but efforts to “protect” their status quo are ill-conceived. It’s time for AHA and its followers to plan beyond clinical innovations, technologies and the current regulatory and political environment. Otherwise, most hospitals will be public utilities.
I do not think the future of the U.S. health system will be a repeat of its past. That’s good news and bad news for hospitals.
Paul
PS: Each week, I try to distill lag and lead indicators from the Clinical Care, Technology, Capital, Funding, Consumer and Regulatory environments of consequence to healthcare insiders. What’s abundantly clear is that outside forces—economic, political, global—will impact U.S. healthcare future more than its internal dynamics. The future for hospitals is not a repeat of their past: that’s clear. What’s unclear is who will shape that future and what role hospitals will play.
I study the future of the U.S. health system. The framework I use is based on monitoring trends, lag and lead indicators in five zones of unique relevance in the health industry at home and abroad:
Clinical innovations that produce new diagnostics, therapeutics & methods of care.
Technologies that improve how processes and decision-making (clinical/administrative) are made, by whom and where.
Regulations (and politics) that set boundaries, define roles, appropriate public funds, protect public interests and facilitate (or not) competition.
Capital markets (public and private) that enable funding, define access (credit) and determine costs of capital (monetary & fiscal policies, interest rates).
Consumers who use and purchase health products and services and vote on health issues.
Based on 30 years-plus years of applying this framework to my industry surveillance process, it’s clear that traditional lag indictors like enrollment, utilization, spending, workforce supply-demand et al are less useful in predicting its future. Instead, indicators from outside healthcare seem more aligned to its future than indicators from within. Why?
Technologies developed outside healthcare now control the system’s processes and pace of adoption. Technologies are solving problems that legacy healthcare has struggled to address. AI-enabled point solutions are reducing administrative cost and inappropriate clinical variation. Private capital is funding cheaper, and better remedies without permission of insiders.
The public’s receptive. Public satisfaction with the status quo has plummeted. Expectations have changed. Affordability concerns have been neglected by insiders. Non-healthcare employers are fed-up. And voters are receptive to solutions insiders fear.
Regulators are changing the rules. Partisan brinksmanship on most contentious healthcare issues has intensified. The Trump administration’s health apparatus (legislative priorities, executive orders, judicial appointments) embraces price transparency, competition, and necessary spending cuts due years of fraud, waste and abuse. And it is facilitating a dramatic increase in state responsibility for implementing and funding its policies.
Objectively, the reality is this: the players outside healthcare including Big Tech, Big Banks and Big Employers are forcing changes faster than healthcare insiders are comfortable and the health system’s future is uncertain as a result. Boards of most healthcare organizations inadequately evaluate future state options due to urgent issues that require attention and/or lack of CEO interest. And in many, long-range planning is relegated to 5-year capital plans and program portfolio updates. Radical change is dismissed, and executive compensation is set accordingly.
Will the health system change radically? Or will it incrementally evolve? To facilitate meaningful discussion, at least three future state possibilities merit deliberation by leaders:
Big Public-Small Private: By 2040, federal and state governments fund 85% of health services funds contracting with private hospitals, medical groups and other providers based on evidence-based performance standards of quality, costs and access. Funding will be sourced from individual and employer taxes while a small percentage of the population will purchase services in a separate, smaller private market. Medicare, Medicaid, CHIP and Social Security programs will be combined (eventually) and budgets will be capped. Note: this model already in place in many developed systems i.e. Canada, UK, et al and is considered an incremental change to the status quo akin to “Medicare for Most” proponents.
Retail health: By 2040, employer tax deductions for employee health benefits are eliminated as a result of employer dissatisfaction with costs and cost shifting by providers based on underpayments by Medicaid and Medicare. Individuals are responsible for purchasing individual insurance and choosing and paying for the doctors, hospitals, medications and ancillary services they use. Note: many economists believe the unintended consequence of third-party health insurance is unnecessary waste, costs and marginalization of consumer choice in healthcare. Forced consumerism, they argue, would bring discipline to health spending. Critics (including most physicians) counter consumers are incapable of smart shopping for their health needs. This option represents a transformational change to the health system wherein its economy is based on retail health.
Restructure: By 2040, system restructuring to reset its focus. The health system’s structure is its major barrier to change. Horizontal consolidation dominant now in most sectors represents a defensive maneuver whereby insiders protect against restructure by imposing its muscle-strength. Current incentives reward specialty providers, inpatient and outpatient services, patent protected specialty drugs, institutional senior care and separate financing and delivery systems. At the same time, they discourage needed investment in behavioral health, enabling of mid-level providers, incentives based on value (costs + outcomes), community-based integration of health and social services programs and guided self-care. Systemic restructure is necessary but unlikely until and unless demanded by community leaders, elected officials and private investors. In the interim, vertically integrated community health organizations will be surrogates for wider adoption.
No one knows for sure what healthcare’s future will be, but all recognize the status quo is not sustainable. Ownership status (for-profit vs. not-for-profit) will matter less and affordability will matter more. Regulation will increase and states will play a larger role. And base rates for reimbursement will decreasingly be based on Medicare rate setting.
Protecting the status quo is not a solution. Failure to seriously evaluate future state options is professional malpractice. Outsiders want results, not excuses.
This will be a quiet week for healthcare in DC with major hearings, confirmations and legislative votes not scheduled.
Last week was relatively calm as well. The House Ways and Means Committee heard testimony from hospital CEOs of HCA, ECU Health, Common Spirit and NY Presbyterian featuring accusations of price gauging and unnecessary costs. And a study that found an OpenAI model outperformed doctors in diagnostic reasoning stirred attention in the physician and healthcare tech worlds where AI’s a dirty word to some and salvation to others.
But, for healthcare, it was an uncharacteristic quiet week. No shutdown announcements akin to Spirit’s 2 a.m. Saturday advisory “winding down all operations.” No strikes by nurses or new megadeal announcements. No public announcements from CMS on new alternative payment models or final rules on reimbursement. But It’s a temporary calm before the tsunami building offshore. It’s the cumulative result of four convergent forces each capable of destabilizing the health economy on its own:
The One Big Beautiful Bill (HR1) Medicaid cuts and work requirements start January 1, 2027: states are scrambling to be ready.
Economists expect prices for gas, food and energy to be high into next year as a result of the war in Iran. Consumer confidence is at a modern-era low.
The labor market is shifting toward the AI economy where server farms and worker displacement are immediate foci.
And polling shows public erosion of trust and confidence in America’s major institutions at a 40-year low including its health system, Congress and even organized religion.
U.S. healthcare has much to be proud of: we justifiably tout our breakthrough meds and devices, Star Ratings, Top 100 lists and modern buildings. We remind legislators we’re the biggest private sector employer in the U.S. economy and, at every opportunity, our economic impact on communities. And, in every sector of our $5.6 trillion industry, we’re now talking about affordability (without defining it).
In April, I met with several health system Boards, limited partners in 2 healthcare investment funds and health officials in 3 states. The sentiments are the same: they’re concerned about the future and preparing for the worst. They’re asking their leaders and corporate strategists to do the impossible—avert the storm, at least for a little while. They’re confident public funds for healthcare are already stretched with no relief in sight. And they’re attempting contingency planning knowing their efforts might be moot given political volatility in DC and states.
Understandably, the appetite for risk taking in organizations and government agencies like these is relatively low. It’s safer to consolidate horizontally than vertically, cut costs, change incentives, modify reg’s slightly than attempt “newer, better, cheaper” solutions to well-known problems. Old playbooks are dependable. And, for healthcare’s operators, radical incrementalism disguised as transformation has served its interests well for 50 years as spending grew from 9% of the GDP in 1980 to 18% today. Bigger players in each sector have done well and pay their executives to keep it that way while the smaller players are collapsing.
Transformation of the system, and a clear destiny for its future are secondary to self-preservation in US healthcare today. Our investors and lenders expect it, Board compensation committees reward it, and our workforce depends on it.
Thus, until and unless elected officials, large (non-healthcare) employers and concerned community leaders act, it will not happen. And if neglected, the entire system will collapse in the next 10 years.
It’s a possibility few Boards of healthcare organizations seriously consider but growing numbers of concerned citizens fear. Like Spirit Airlines passengers and its 17,000 employees are experiencing, they’re SOL.
Paul
PS: I am in Alaska this week with the Southcentral Foundation, the Alaska Native-owned 501(c)(3) nonprofit that provides comprehensive outpatient and inpatient services to more than 70,000 Alaska Native and American Indian peoples living in the Indian Health Service’s Anchorage Service Unit. Two features of how SCF operates impress me: its purposeful blending of physical, mental, emotional and spiritual wellness in care management, and its Nuka System of Care ownership model in which individuals are customer owners, not patients. There are lessons to be learned from both.
To understand how private equity, or PE, may be reshaping the way physicians experience the practice of medicine and their relationships with hospitals, insurers, and patients, we interviewed six doctors who have worked for PE-backed practices and four advisers who guide physicians through the partnership process.
We wanted to know if an infusion of capital from private investors with plans for expanding or restructuring a practice makes it easier for physicians in private practice to maintain a sense of independence and even lessens burnout. Or instead, if these transactions convert once-independent doctors into employees with less agency than before.
The physicians we interviewed included two urologists who ran one of the largest PE-backed specialty practices in the United States before it sold to Cardinal Health; two orthopedic surgeons and one obstetrician/gynecologist (ob/gyn) whose practices were acquired; and an anesthesiologist who saw his own practice disrupted when two PE-backed staffing companies shook up the local market. All but one agreed to speak on the record about their experiences. The other asked to remain anonymous because his comments focused largely on former colleagues.
When Investors View Doctors as Partners, Satisfaction with Private Equity Deals Is Higher
For physicians, the value of private equity investment is very much in the eye of the beholder, and it’s largely contingent on whether physicians are treated by the investors as employees or as business partners. The PE deals that go awry — sometimes publicly, due to litigation or physician departures — often involve ventures where PE firms extract profit by changing productivity standards, staffing models, and hours of operations. When profits are achieved by expanding a practice’s services or its geographic reach, there’s more opportunity, if not incentive, for partnership.
Specialties in which changes in technology or treatment protocols are redefining the role of physicians can create growth opportunities for PE firms and the practices themselves. Urology provides an instructive example. Over the past three decades, as treatment modalities for prostate cancer have evolved, urologists have assumed a more sizeable role in cancer care. While it can be lucrative to provide radiation therapy, immunotherapy, and oral oncolytics or infusions in outpatient settings, or establish ancillary businesses such as pharmacies, these require upfront capital and management expertise. Practices with 10 or fewer urologists, once the norm in the U.S., may lack the resources to take advantage of these opportunities. They also may struggle to compete with nearby health systems that command higher payments from insurers and larger discounts from suppliers.
Add in the difficulty of recruiting younger urologists to replace retiring doctors and administrative burdens such as managing payer contracting and cybersecurity threats and PE begins to look more like a savior than a threat. Indeed, while nearly half of urologists were employed by hospitals or other institutions as of 2019, PE acquisitions of urology practices have become a dominant form of practice consolidation in recent years.
Upfront Payment Leads to Practice Changes and a Big Payday
Solaris Health, at one point the largest of at least six PE-backed urology practices in the United States, scaled quickly — from 130 physicians when it was launched in 2020 to almost 800 in August 2025. It did so by pitching itself as a national practice controlled by physicians but backed by Lee Equity, a firm with investments in many specialties. Those who signed on received stock and a lump-sum payment that, in keeping with the conventions of PE transactions, was a multiple of a practice’s future income that physicians were willing to forgo. Although the cash is an advance on future earnings, the payment is often taxed at a capital gains rate, enabling physicians to reduce their tax burden and begin investing.
“I always tell doctors if you’re tempted to buy a boat with the money, don’t. Take the cash and invest it,” says Gary Kirsh, MD, cofounder of Solaris Health. He served as the company’s CEO until Cardinal Health, a pharmaceutical and medical products supplier, paid $1.9 billion for the business in 2025.
In the lead-up to such sales, PE firms recoup their investment through what’s known as “the scrape” — taking a percentage of practice profits, typically between 20 percent and 30 percent. While this makes a sizeable dent in physicians’ take-home pay, many PE firms promise to restore income to previous levels by increasing practice revenues or reducing expenses. Known as “income repair,” it’s a process that can take a few years to play out.
Raj Patel, MD, a urologist from Homewood, Ill., who joined Solaris Health in 2021 and served on its corporate board, was initially skeptical of promises of revenue growth because he was already so entrepreneurial. He also valued his independence. “I would tell my partners, our group doesn’t need private equity,” Patel says.
Over time, however, Patel began to see that joining a large PE-backed practice, with more than 120 urologists in the Chicago area alone, might be a way to enhance access for patients and professional satisfaction for doctors. Instead of everyone performing the same procedures and sending advanced cases to large health systems, they could begin to subspecialize and refer patients to one another.
While the MSO took a share of profits, it also assumed an equal share of an individual practice’s expenses, including the cost of hiring advanced practice providers to handle low-acuity cases and manage calls from staff in local emergency departments — a pain point for Patel’s practice, as this support was expected by hospitals but not reimbursed. Solaris also hired navigators to support patients as they explored different options for treatment. And it had the financial resources to invest in a laboratory for genetic testing, a pharmacy, and the data analytics to determine why some practices had better clinical outcomes or financial performance than others. Although clinicians are expected to follow clinical pathways, Patel says those are determined by clinicians that advise the MSO. “Physicians really need to lead that,” he says.
After he joined, Patel was also able to begin enrolling his patients in clinical trials, another income stream. As revenues increased, Patel achieved income repair in just one year. While some might worry this may lead to higher health care costs, Kirsh believes the opposite is true — that consolidation of physician practices enables clinicians to steer patients to outpatient settings, which, he says, can be significantly cheaper than hospital-based care due to lower fixed costs and the avoidance of facility fees.
Our business model is not to acquire scale and hold insurance companies hostage on rates. We’re creating a national network that shares best practices, professional management, and ancillary services, and doing it in a way that streamlines care for patients.
Gary Kirsh, MDcofounder, Solaris Health
Cardinal Health says it hasn’t made changes to Solaris’s operations or pricing since the acquisition; whether that holds true remains to be seen. Its management services organization, The Specialty Alliance, formed in 2025, now has a stake in the practices of roughly 3,000 providers specializing in gastroenterology and urology. The company also has acquired practices affiliated with Integrated Oncology Network, which has 50-plus community-based oncology centers and more than 100 providers. Sen. Elizabeth Warren (D–Mass.) has raised concerns that the company is buying physician practices as a means of locking customers and physicians into restrictive contracts for drugs and other supplies, reducing competition among wholesalers, and driving up costs. She’s also concerned that practice acquisitions will reduce competition between hospitals and nonhospital providers and has called on the Federal Trade Commission to scrutinize pending sales.
Soon after the deal was announced, Kirsh retired as CEO, handing the reins to James Weber, MD, a gastroenterologist from Southlake, Texas, who became CEO of Specialty Care Alliance after Cardinal acquired a majority stake in GI Alliance in November 2024 for $2.8 billion. Weber says Cardinal’s investment enabled his group to get off the private equity “merry-go-round” and begin partnering with urologists and other specialists who aren’t solely dependent on hospitals for delivering care. Instead of buying a stake in the MSO only to sell it again, as a private equity investor might, Cardinal sees value in building a long-term relationship with physicians as this diversifies its customer base and opens up the possibility of selling higher-margin products and services, Weber says. Rather than forcing such supplies and services upon doctors, Cardinal competes with other vendors in an open-bidding process and profits when the MSO gets the best deal it can — even if it’s from a competitor, he says.
Where Growth Is Harder to Achieve, Tensions Are Magnified
Partnering with private equity firms may have less upside for specialists who have reduced practice expenses to the bare minimum; have maximized their income from ancillary services like imaging, physical therapy, and durable medical equipment; or are working at full tilt. In these instances, income repair may be impossible, especially if the firm tacks on new charges or takes away benefits.
Two orthopedic surgeons we spoke with, one in Pennsylvania and the other in Florida, said partnering with PE had cost them financially. Both had worked in what they described as well-respected practices that faced competition from large academic medical centers intent on expanding, in one case by buying up primary care practices that influenced local referrals patterns. As nonprofits, the systems had several advantages: a lower tax rate and access to the federal 340B Drug Pricing Program, which allows safety-net providers to purchase drugs at a discount and receive reimbursement from insurers at market rates.
Adrienne Towsen, MD, an orthopedic surgeon from West Chester, Pa., says that after her 75-physician practice was sold in 2022 to a management company backed by PE, promised changes to back-office functions never materialized, and the accounting grew more opaque. Then came cuts. Doctors were told they needed to start paying for their own cellphone plans, as well as life and disability insurance. Management fees also increased, and the ancillary income physicians once earned from physical therapy and MRIs — worth as much $100,000 a year to each doctor — was carved out of their compensation.
While she had received an upfront payment, she found it didn’t make up for the cuts in her take-home pay. Towsen says part of the problem was that the revenue target she and her colleagues needed to hit to bring fees down was set at an all-time high, the year of the sale.
Towsen says she started to feel like she was caught in a bad relationship. Problematic behavior was followed by unfulfilled promises from management to do better. She wanted to exit, but the contract required her to pay back the lump sum if she left before three years. Leaving also would trigger a noncompete clause, severing relationships with patients she’d built over two decades. She resigned the first day she could, giving up her shares in the company.
Equally painful was the disruption in her relationships with patients. “I had very frank discussions with patients and told them exactly why I was leaving. They were upset,” she says. Many reported experiencing similar problems with other specialists.
I kept hearing, ‘I’m losing all my good doctors.’ It makes you feel so guilty.
Adrienne Towsen, MDorthopedic surgeon
When the Math Doesn’t Add Up
R. James Toussaint, MD, an orthopedic surgeon in Florida who worked in investment banking before going to medical school, chose to join The Orthopaedic Institute in Gainesville because it had a reputation for high-quality care and was large enough for him to subspecialize in foot and ankle surgery. When PE firms came calling in 2017, he had a hard time persuading his partners that it would be the PE firm that benefited, not them. “I had structured deals like this myself and knew what the benefits and drawbacks were. I also knew once you sell your house, it’s nearly impossible to buy it back,” he says.
Once the sale went through, he says the firm added new layers of management overhead, including executives tasked with business development and marketing. “These aren’t positions generating revenue the way surgeons do. They’re essentially cost centers,” Toussaint says.
Since he had already maximized the hours he worked, as well as opportunities to earn income from ancillary services like MRIs, physical therapy, and durable medical equipment, there wasn’t a way to offset these expenses and other management fees by working longer hours. “There’s no eighth day in the week to work,” he says.
He says the lump-sum payment he’d received wasn’t sufficient to cover the loss of income. After a couple of years, he decided to resign and negotiated a settlement to release him from the noncompete clause. He then joined the academic medical center that was once viewed as a competitor, a move he wishes he made sooner. “Looking back, the whole transaction just made no sense. I should have just left immediately because there literally was no upside.”
Toussaint says in some cases patients are left in the dark when physicians leave. “It’s embarrassing for the group,” he says. “So they just say they left or they retired and the patients are left trying to figure out where their doctor is. It’s unfortunate.”
We reached out to the private equity–backed ventures that help run the two orthopedic surgery practices for comment. Both offered to connect us to physicians with a different perspective.
John Stevenson, MD, a neurosurgeon who’s been at The Orthopaedic Institute for three decades, agreed the early days of partnering with a private equity–backed firm had its ups and downs, in part because they were the first orthopedic practice to do so and it took time to develop and execute a growth strategy. But over the long run, he says he’s come out ahead because he’s been able to see more patients with the help of midlevel clinicians and gained access to better insurance contracts, lower-cost supplies, and other resources that help patients, including staff with pain management expertise.
Jason Sansone, MD, an orthopedic surgeon in Madison, Wis., found it helpful to partner with the private equity–backed venture Towsen did — Healthcare Outcomes Performance Company (HOPCo). He’d been employed by a multistate health system but found its bureaucracy and the inability to innovate stifling. “We wanted more autonomy and offered to assume financial risk in exchange for it,” he says, but the health system insisted on an employment model.
In 2023, he and 10 other doctors struck out on their own, betting they could negotiate contracts with payers that would reward them based on the value of services they provided rather than the volume. “Sometimes that means more conservative treatments and other times, it’s just doing surgery instead of requiring patients to go through physical therapy and steroid injections that you know aren’t going to help,” he says. Having fought for their independence, he and his partners were reluctant to give up equity in their practice, so they hired HOPCo to provide management services and built an ambulatory surgery center as a joint venture. Sansone says he’d only consider giving up equity in the practice itself to fund an expansion. “We view private equity as a source of capital for growth rather than a means of generating liquidity,” he says.
From Boutique to Big Box Store
The ob/gyn we spoke with, now working in North Carolina, joined a large obstetrics practice just three months before its partners voted to sell it to a PE-backed venture. As a new hire, Dr. M (who asked for anonymity because his comments focused largely on former colleagues) wasn’t eligible for the lump-sum payment, but he figured that banding together with other doctors in his state would improve payer contracts and make it easier to participate in value-based contracts.
Dr. M didn’t anticipate how hard it would be to lose the ability to make business decisions — like choosing a vendor or launching an infusion clinic so pregnant patients experiencing nausea didn’t seek emergency care. Merging practices brings standardization that tends to lift low performers but restricts the flexibility of high performers, he says. “It’s like going from being a boutique specialty store to being bought out by Walmart. We were doing everything in-house and doing things well. It cheapened our brand.”
Dr. M also didn’t like having salaries capped. He figured his fellow physicians were leaving as much as $200,000 on the table each year despite seeing as many as 35 patients per day.
I think there are people who are happy just going to work and getting a paycheck, but if you are in medicine to take care of patients and be in business, private equity ownership is a frustrating thing.
Dr. MOb/gyn
After three years, Dr. M left to become a “locum tenens” provider, a temporary worker paid at a premium by a hospital to fill a critical workforce gap. While there is a baseline level of job insecurity inherent in being a locum provider, they usually command high hourly rates for short-term work, giving providers flexibility but potentially disrupting relationships between patients and providers. “Locums is inherently bad for obstetrics,” he says, and some doctors may avoid it because they can’t foster long-term relationships with patients, but he believes younger patients view doctors more interchangeably and prioritize having timely access to any doctor rather than a specific one. “They’re not necessarily as sentimental as their parents were,” he says.
Dr. M thinks locums jobs may be increasingly attractive to physicians with young families who want substantial time off and to new residency graduates who don’t want to work as employees in large provider groups but have trouble identifying smaller independent practices. As for his old colleagues, he says, “I’m not mad at them that they joined with private equity. I am more frustrated by the fact that they felt like they had to.”
Trying to Sidestep Private Equity
Not all medical specialties draw interest or upfront cash from private equity firms. Since the No Surprises Act went into effect in 2021, preventing hospitals from charging out-of-network rates for the services of emergency physicians, anesthesiologists, and other emergency care providers who opt out of insurance networks, PE firms have had less incentive to invest in their practices.
Marco Fernandez, MD, an anesthesiologist and former president of Midwest Anesthesia Partners, the largest group of independent anesthesiologists in Illinois, turned down such offers when they came in because he doesn’t like how PE-backed anesthesia groups tend to assign cases to certified nurse anesthetists and make physicians their supervisors. “We wanted to do our own cases and take care of our own patients,” he says. “If we’d sold or joined a staffing company, we’d be managing as many as 10 surgeries at once. It would make us glorified rescuers, running in for emergencies and filling out paperwork,” he says. “It’s a different level of stress.”
Retaining hospital contracts for the then-300-physician group became much harder when PE-backed staffing companies using such models stepped into the market, offering a less expensive service. “Within a two-week span, we lost two contracts,” Fernandez says. Some physicians in the group opted to join PE-backed ventures or become hospital employees. The remaining 100, who wanted to retain their model, now primarily serve ambulatory surgery centers or work in three hospitals as locum providers. Similar disruptions are playing out in other markets, leading to delays in surgeries.
Fernandez worries that not having the same anesthesia staff in facilities will impede communication and quality improvement, but he hasn’t found hospitals willing to subsidize a physician-centric approach. In 2022, he joined three other anesthesia groups in forming the Association for Independent Medicine, an advocacy organization that’s been calling for greater regulatory oversight of PE ventures and protections of clinicians’ decision-making. Another organization, the Coalition for Patient-Centered Care, is pursuing a similar mission, in part by asking state and federal lawmakers to apply antikickback and fraud and abuse laws to PE acquisitions of physician practices.
Partnership Is Crucial
The experiences of these physicians, while purely anecdotal, suggest private equity investment can be advantageous if the partnership is structured in a way that aligns physician and investor interests. “A lot of the bad case studies you see involve private equity firms turning physicians into employees whose income is tied to what they generate, mirroring what health systems do,” says Robert Aprill, a partner with Physician Growth Partners, an investment banking and advisory firm that represents physicians in transactions with PE firms. There’s higher satisfaction when investors tie compensation to practice profitability and add value by helping clinicians gain access to data and discounts on supplies, he says. “Private equity can become a vehicle to create super groups across state lines.”
Physicians have to be flexible, Patel says. “Whenever you sell to private equity, it’s not a lifetime achievement award where you walk away with a check. It’s a growth model. That’s where I see private equity deals fail. Both sides aren’t willing to grow together.”
If a partnership goes awry, there can be severe consequences for physicians. Toussaint says that half of the partners at his former practice were gone at the time he spoke with us, and that there was a “mind-boggling” amount of litigation happening. While MSOs typically pick up the cost of a defense, such expenses cut into the profitability, and thus the resale value, of the business. Towsen has also seen instances in which doctors departing from PE-backed ventures had to hire lawyers and forensic accountants to protect their interests.
Keep the Exit Pathway Clear and Well Lit
Too often physicians get distracted by the lump sum that private equity firms offer and sign away rights via letters of intent before showing them to a lawyer, says Randal Schultz, JD, CPA, a health care lawyer with Lathrop GPM in Kansas City. He encourages his clients to capture what matters most to them in contracts, including the hours and years they are expected to work, the terms of compensation that can and cannot be altered, and, perhaps most important, the circumstances under which they can exit without being subject to a noncompete clause or a clawback of the initial payment. “If you get terminated without cause, or they breach the contract, you should be able to walk away without any restrictions,” he says.
PE firms often understand and will try to exploit physicians’ risk aversion, Toussaint says. They know that clinicians with children and tuition bills in their future may be hesitant to start practicing in a new area. In addition to uprooting a family, they’d be subjecting themselves to additional background checks and licensing paperwork. “It’s really time-consuming and draining,” he says.
Ericka Adler, JD, LLM, who leads the health law practice at Roetzel and Andress in Chicago, encourages physicians to think about how they will continue to practice if things go south. “I’ve seen doctors who were terminated from their practices after selling it be subject to a noncompete clause,” she says. Adler also sees a lot of young doctors who are very opposed to working with a PE firm. They want an exit pathway written into their contracts if the practice they join decides to sell to one, so they can move on to a practice that isn’t PE-owned or PE-managed.
Invest in Yourself
Toussaint hopes physicians will consider a third way: capitalizing themselves. “If you have a good management team for your practice, tell them to borrow money to pay partners who want to retire. Then use some of that money to stay true to your growth strategy,” he says.
Now in academia, Toussaint warns the residents he trains to preserve their freedom at all costs. “I tell them your entire life as a doctor has been trying to get in — to the best high school, the best college, and the best medical school. Now your goal when you are negotiating these contracts is to figure out how the hell to get out.”