Medicare starts a long road to cutting prices for drugs, starting with 10 costing it $50.5 billion annually – a health policy analyst explains why negotiations are promising but will take years.
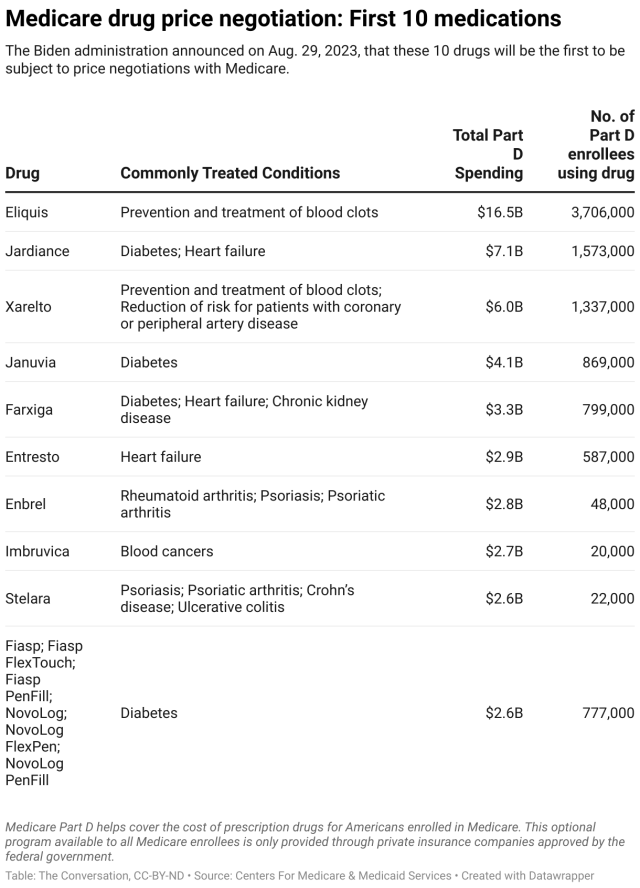
The Biden administration released on Aug. 29, 2023, a list of the first 10 drugs that will be up for negotiations with pharmaceutical companies over their Medicare prices.
The drugs are purchased through Medicare Part D, a prescription drug coverage program for Americans ages 65 and older. The 10 medications accounted for more than US$50.5 billion in gross costs between June 1, 2022, and May 31, 2023.
Provisions authorizing these negotiations were part of the Inflation Reduction Act which Congress passed in 2022, allowing Medicare to negotiate drug prices for the first time. Pending successful negotiations, these changes would amount to what researchers estimated to be net savings of about $1.8 billion in 2026. The Congressional Budget Office projected an even bigger savings of $3.7 billion.
The top 10 list includes such drugs as Johnson & Johnson’s Xarelto, which treats blood clots, and Amgen’s Enbrel, which treats rheumatoid arthritis and psoriasis.
Negotiations are expected to begin in October and continue until August 2024, with lower prices going into effect in 2026.
Democrats have hailed the new law’s drug pricing provisions as game-changing. They’re likely to make the issue a centerpiece of their 2024 election campaigns. Democrats are further emboldened as public opinion polls show overwhelming support for the policy among Americans.
As a scholar who researches the politics of health policy, I’m skeptical that Medicare drug price negotiations will end up making as big a difference as Democrats have promised, at least in the near future. While U.S. prescription drug prices are excessive, the true potential of the policy is unclear, as it remains muddled in lawsuits and industry opposition. However, if it can withstand the ongoing attacks and become settled law, Americans ages 65 and up could see real financial relief down the line.
Cutting drug costs for Medicare enrollees
The Inflation Reduction Act allows the Centers for Medicare & Medicaid Services to negotiate prices with the companies that make some of the most expensive drugs in the Medicare program, including life-saving cancer and diabetes treatments like Imbruvica and Januvia.
If the negotiations proceed as planned, the drug-price-negotiation provision is expected to save the U.S. government about $98.5 billion by 2031 by allowing it to pay less on prescription drugs for Americans on Medicare – nearly 66 million people. The Biden administration hopes that these cost savings will be passed down to Americans 65 and older through reduced Medicare Part D premiums and lower out-of-pocket costs.
The Inflation Reduction Act provides additional benefits for older Americans, including limiting their out-of-pocket expenses for prescription drugs to no more than $2,000 annually, limiting the growth of Medicare Part D premiums, eliminating out-of-pocket costs for vaccines and providing premium subsidies to low-income people ages 65 and older.
The Inflation Reduction Act also includes a separate provision that requires drugmakers, under certain conditions, to provide the Medicare program with rebates if drug price increases outpace inflation, starting in January of 2023. That measure is expected to yield $71 billion in savings over a decade.
Penalties for companies that won’t negotiate
The 10 drugs that the Centers for Medicare & Medicaid Services have selected accounted for $3.4 billion in out-of-pocket spending in 2022 for Americans ages 65 and older and $50.5 billion, or about 20%, of total Part D gross prescription drug costs from June 1, 2022, to May 31, 2023.
Pharmaceutical companies have to sign agreements to participate in the upcoming negotiations by October 2023. Based on criteria such as public feedback and consultation, as well as the clinical value of the drug, the Centers for Medicare & Medicaid Services will make an initial price offer in early 2024, with the potential to further negotiate the price until August 2024. Going forward, additional drugs will be subject to negotiations.
If drugmakers don’t negotiate, they will face stiff penalties in the form of a tax, reaching as high as 95% of U.S. pharmaceutical product sales. Alternatively, the companies may pull their drugs from the Medicare and Medicaid markets, meaning that seniors on Medicare would lose access to them.
Why US drug prices are so high
Americans pay substantially more for prescription drugs compared with people who live in countries with similar economies, like Germany, the U.K. and Australia. While Americans spent more than $1,100 a year in 2019, Germans paid $825, the British paid $285 and Australians paid $434 per person.
The reasons for this disparity are multilayered and include the overall complexity of the U.S. health care system and the lack of transparency in the drug supply chain. Of course, many other countries also directly set prices for drugs or use their monopoly on health services to drive down costs.
For example, Dulera, an asthma drug, costs 50 times more in the U.S. than the international average. Januvia, a diabetes drug that is among the first 10 drugs up for price negotiation, and Combigan, a glaucoma drug, cost about 10 times more.
These costs impose a big burden on Americans – 1 in 5 of whom skip at least some of their prescribed medications due to the expense. Those 65 and older are particularly affected by these problems.
Strong resistance
It’s too soon to say how big the impact of the drug pricing provisions will be and whether this policy will be sustained.
Drugmakers have opposed any governmental regulation of drug prices for decades. They are fighting the measure in court and running a public relations campaign that warns of reduced investments in life-saving cures because their financial incentives are reduced.
Even if the drug price negotiations survive the industry’s legal challenges, it’s possible that future Republican administrations won’t embrace or enforce this policy. This is because potential Republican wins in the 2024 presidential and congressional elections could unravel or severely curtail the new drug negotiation policy. Indeed, Republicans have been working feverishly on designing a strategy to use the negotiations against Democrats in the upcoming elections.
Weighing the prospects
In my view, the government’s efforts to cut prices for prescription drugs that Part D enrollees obtain are a step in the right direction. For now, the effect will likely be small because patients already receive discounts on the listed drugs, bringing the net savings down substantially. However, the potential for real savings for Americans ages 65 and older will undoubtedly grow as more drugs become subject to negotiation.
At the same time, drug manufacturers have indicated that they are willing to take their legal battles against the Medicare drug pricing reform all the way to the Supreme Court. If that happens, there’s a good chance they will prevail because the arguments made in their lawsuits are likely to appeal to the Supreme Court’s conservative majority, which has been favorable to many of the arguments made by drugmakers in their lawsuits.
Moreover, drugmakers could also simply pull their drugs from Medicare and Medicaid to force the government’s hand. The Centers for Medicare & Medicaid Services seems to have deliberately chosen drugs that make up a high percentage of manufacturers’ drug sales to counter this possibility. The industry has a history of skillfully exploiting loopholes and possesses a vast lobbying apparatus.
It’s also too soon to know if this is going to be a win for American patients overall. It’s possible that Americans who aren’t covered by Medicare may actually see prices go up. That’s because if drugmakers do make less money on drugs for people enrolled in Part D, they might make up for those lost profits by charging more for drugs that other people depend on.
And lastly, it’s possible that there will be fewer new prescription drugs – as an indirect result of this policy that’s supposed to improve access to health care – because it may reduce drugmakers incentives. While the number of cases is likely small, it would potentially take a toll on patients who might have seen a cure to their disease – or some relief from their symptoms.