Congressional negotiators are working to revive the health care deal that was dropped from a government spending package in late 2024 — but the odds of resurrecting enhanced Obamacare subsidies as part of the effort appear dire.
Why it matters:
Long-stalled bipartisan priorities that are in play include an overhaul of pharmacy benefit manager practices, as well as a measure that would place more controls on Medicare outpatient spending.
They’d likely be combined with a renewal of health programs due to expire Jan. 30, including certain Medicare telehealth flexibilities and funding for community health centers.
Driving the news:
Leadership and health committees in both parties have quietly swapped offers on a package over the past week while attention was primarily focused on the fight over expired Affordable Care Act tax credits.
Democrats included a three-year extension of the ACA subsidies in their latest offer knowing that GOP leadership is likely to reject it, sources said.
That would still leave intact most of the health care deal that was destined to ride on a government funding package before it was scuttled at the last minute by Elon Musk and then President-elect Donald Trump.
What we’re hearing:
Asked about the likelihood of a health package without the ACA subsidies, Senate Finance Committee Ranking Member Ron Wyden (D-Ore.) pointed to the overwhelming 26-0 vote in his committee for the PBM overhaul in 2023.
“I’m not going to negotiate with myself but the reality is I think a 26-0 vote in the Senate … it’s like unheard of,” Wyden told Axios, adding he is “feeling upbeat” about getting the PBM bill over the finish line.
Senate Finance Chairman Mike Crapo (R-Idaho) also told Axios he is “feeling optimistic” about the PBM bill, saying there is “broad support here and at the White House.”
That measure includes provisions like “delinking” the price of a drug from PBM compensation in Medicare Part D.
The prospective package would also include a measure that would require off-campus hospital outpatient departments to have a unique identifier number.
It’s a cost-saving measure designed to prevent outpatient departments from billing payers at higher amounts associated with full-service hospitals.
But it would stop short of a full-scale, more sweeping change known as site-neutral payments that would more closely align Medicare payments to hospital outpatient departments with freestanding physician offices.
The intrigue:
The outlook for renewing enhanced ACA subsidies, which help millions of Americans afford their premiums, is much bleaker.
While a separate bipartisan group of senators continues to meet in search of a compromise, a key negotiator, Sen. Bernie Moreno (R-Ohio), told reporters on Tuesday that a release of a proposal would be punted until after next week’s Senate recess.
Even if the group can release a proposal — which would include GOP-backed changes like eliminating $0 premium plans — there is deep skepticism in both parties that it can actually pass.
Many Republicans are opposed to any kind of ACA subsidy extension, saying it is wasteful spending that benefits insurance companies.
Top Democrats are pushing for a clean subsidy extension without GOP-backed changes and blasting Republicans for blocking it, in what could be a preview of midterm campaign messaging.
Between the lines:
There still are significant divisions over whether to include new limits on the ACA funding going to plans that cover abortions.
The bipartisan group has discussed a potential compromise that would increase audits and levy penalties on insurance companies that don’t comply with existing rules requiring them to segregate taxpayer money from paying for abortions.
The idea immediately drew fire from the anti-abortion group Susan B. Anthony Pro-Life America, and many Senate Republicans think it does not go far enough.
The bottom line:
There still could be an election-year health deal — just don’t expect it to address ACA subsidies.
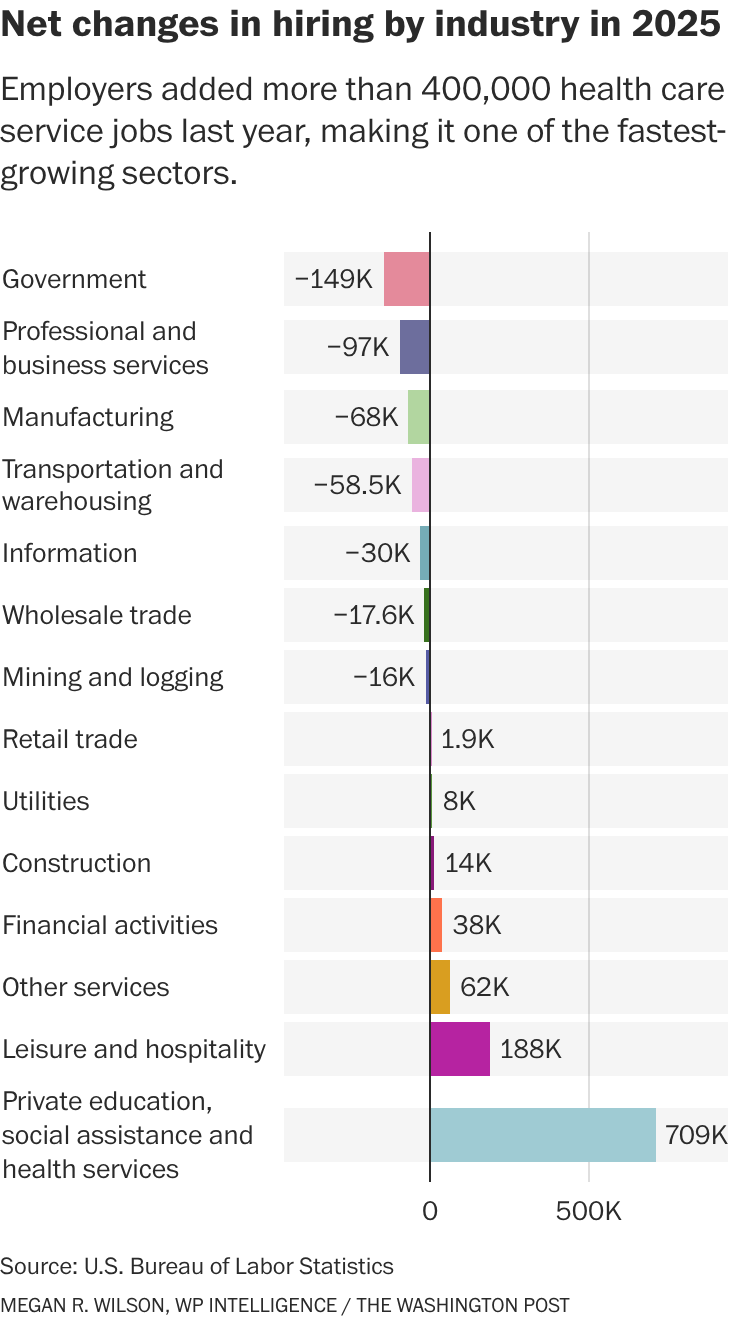
The health services industry was once again a bright spot in the economic data in today’s jobs report, which otherwise landed with a thud and capped off the weakest year for overall hiring since the pandemic.
The growth underscores how much health care employers are propping up the overall labor market — accounting for most of the gains, both in sheer numbers and percentage growth.
“The fundamental reason why health care employment continues to grow so strongly is that the aging population continues to boost demand for health care services,” said Jed Kolko, a senior fellow at the Peterson Institute for International Economics. “The population will continue to age, so that fundamental driver of demand continues.
”Behind the numbers: Although economists expect the health industry to continue expanding, they note that 2025 represented a slowdown from the previous year. Although many factors are at play, multiple analysts said the Trump administration’s restrictive immigration policies may be to blame. More on that later.
It’s not a huge surprise that people working in places such as hospitals, dentists’ offices and nursing homes represent the largest growth in hiring: Health care makes up about 18 percent of the overall U.S. economy — which means that $1 out of every $5 that Americans spend goes to health care. Advertisement
But this also highlights how health services hiring is keeping broader U.S. employment from sliding — even as other industries cool. Patients and providers alike are bracing for cost and workforce pressures in 2026.
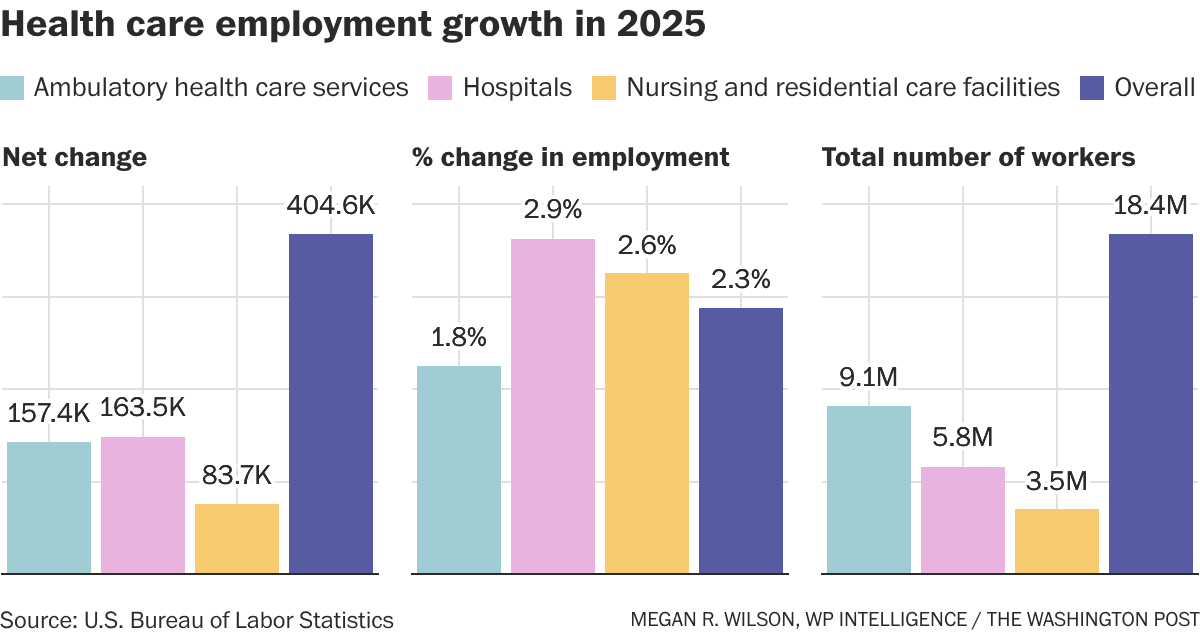
Dive in: Although the number of people working in health services increased by more than 404,000 in 2025, it’s still a slowdown from the level of growth the sector saw the year before. In 2025, the health industry added about 34,000 workers per month, according to federal data, compared to an average monthly gain of 56,000 health jobs in 2024. This included people working in hospitals, residential care facilities or nursing homes, diagnostic labs, and for home health providers .
Here’s how it breaks down:
Hospitals represented the highest employment growth rate — 2.9 percent — in the health services industry, followed by jobs at nursing homes and residential care facilities, at 2.5 percent.
“We’re getting older and sicker. And, on top of that, we’re getting older and sicker in a way [where] we don’t have young people around to take care of the older, sicker people, right?” said Richard Frank, economic studies senior fellow at Brookings and director of its Center on Health Policy. Advertisement
“So what used to be long-term care delivered by family members when we had four or five kids per household, that looks very different today,” Frank said. “You’re going to have to pay people to do that work.
”While economists anticipate health care hiring to continue to grow — in part for that very reason — there two major policy shifts loom as a dark cloud over the industry and may impact the health services workforce.—
Immigration: Providers around the country have said that the Trump administration’s approach to immigration has hampered their ability to hire people. The administration has been cracking down on legal immigration as well as on people who have come to the U.S. illegally. Meanwhile, immigrants make up 28 percent of the long-term care workforce and 32 percent of home care workers, according to KFF.—
Medicaid cuts: The Republicans’ tax-and-domestic-policy law enacted last July is expected to slash nearly $1 trillion from the Medicaid program for low-income Americans. Researchers estimate that this will hammer the balance sheets of many hospitals, which are likely to see an influx in patients seeking care but are unable to pay for it. Hospitals and health clinics are already shutting down or laying off workers across the country. Although the Medicaid policy changes — which won’t fully kick in for years — aren’t the only reason for the closures, it shows how vulnerable many providers already are.
Other changes, including the proposed cuts to the National Institutes of Health, could trickle down to communities with research hospitals and ultimately impact the labor market, according to research from the Brookings Institution. New Medicare payment policies that aim to shift care away from expensive hospital services and toward primary care could also have an impact, although it likely won’t be large enough to show up in the data, I’m told.
However: Some states are working to offset some of the administration’s immigration policy changes or health program cuts, which could make it hard to evaluate their impact in the next round of employment data. “There are a lot of … crosswinds blowing in the aggregate that might cover up” the overall impact of these policies,” said Frank.
Other data: Employment in what the government calls “individual and family services” — listed under the “social assistance” category — increased by more than 289,000 people in 2025, representing a nearly 9 percent increase over 2024. These jobs include personal care aides, social workers and substance abuse counselors.
Congress returns to DC this week to debate the merits of extending the advanced premium tax credits that enable coverage for 4 million in a climate of high anxiety about U.S. intervention in Venezuela and heightened tension with Russia and China.
For many, these unfolding events are numbing: helplessness, frustration and fear are widespread. As 2026 unfolds for U.S. healthcare, the realities are these:
The healthcare economy will be under pressure to do more with less. The health economy is increasingly controlled by private investors and large publicly traded companies in every sector whose shareholder obligations are primary. Public funding from federal, state and local sources is shrinking as a result of the Big Beautiful Bill and pushback from taxpayers who think the system wasteful and ineffective. The S&P Health Index for 2025 closed the year underperforming the broader market. Private equity investments in healthcare except AI solutions that reduce operating costs at scale are troubled. Thus, in 2026, operating margins in every sector will be stressed, access to private capital will be vital and business as usual obsolete.
Mass populism will magnify attention to the healthcare affordability. Per polls, costs of living are issue one to voters. While prices for gas and groceries have moderated, housing and healthcare prices have escalated unabated. Voters think both essential but the majority think consolidation, corporatization and regulatory protections advantage the biggest players and protect special interests. In housing, it’s simpler for consumers: mortgages, rent and utility costs are straightforward. But healthcare is more complicated: out of pocket costs—premiums, co-pays, deductibles, caregivers, OTC et al—are not easily calculable and price estimator tools, patient support and revenue cycle management policies make it easier for consumers. The net result: a large and growing majority of voters think healthcare is unaffordable and government intervention needed.
The mid-term election November 3, 2026 will be likely be the reset for healthcare’s future in 2028 and beyond. All 435 House Seats, 35 U.S. Senate seats and 39 state/territorial governors will be elected. All will face voters anxious about the future and how they’ll pay their bills. The 2026 results will set the stage for 2028 Presidential campaigns that will feature a wide range of alternatives to the healthcare status quo. Some will be incremental; others labeled radical. But all will promise changes unwelcome to many of its prominent incumbents.
Each sector in healthcare—hospitals, physician services, long-term care, insurers, life science manufacturers, enablers and advisors—is vulnerable. None welcomes unflattering attention and all spend heavily on messaging and advocacy to protect themselves. All recognize the elephant in the room—large employers that have patiently funded the system’s profitability and value protective regulation that limit disruption. And in all, implementation of AI solutions that lower operating costs and streamline performance is THE immediate priority.
The realties of 2026 for healthcare are foreboding: business as usual is not an option.
There’s a good chance your health insurance premiums are going up next year, regardless of where you get coverage.
Why it matters:
The spike in what millions of Affordable Care Act plan enrollees pay will be acute, but workplace insurance is getting more expensive, too — and all at a time when affordability is prominently on Americans’ minds.
ACA premiums have dominated the political discourse in Congress for weeks, but there’s no real sign that any relief is coming from Washington.
Even extending the Biden-era enhanced ACA subsidies — which most Republicans don’t want to do — would do nothing to address what’s driving the surging cost of care or employer insurance affordability issues.
And all signs point to Democrats hammering Republicans for high costs in all forms of health insurance leading up to next year’s midterm elections.
The big picture:
Health insurance gets more expensive almost every year, keeping up with increases in the costs of procedures, tests, drugs and more. But some years see bigger jumps than others, and 2026 is looking like one of those years.
That means tough choices for families, employers and workers all faced with shouldering higher premiums or out-of-pocket spending. Some will conclude it’s prohibitively expensive and go uninsured.
Another thing that’s different about this year is that the white-hot political rancor around ACA premiums is putting health insurance back centerstage politically.
By the numbers:
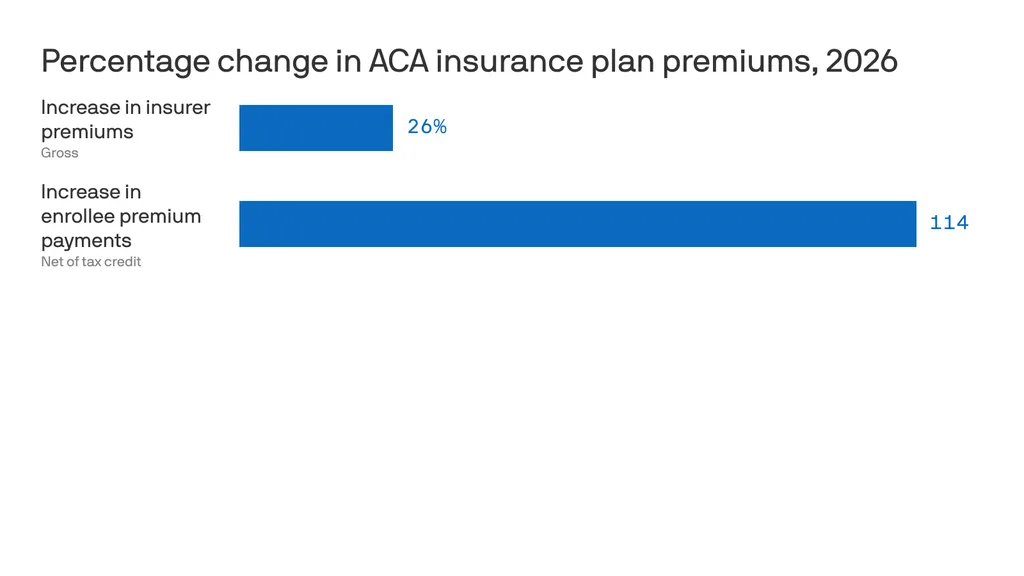
ACA insurers themselves are raising premiums by an estimated 26%, in part due to rising hospital costs, higher demand for pricey GLP-1 drugs like Ozempic, and the threat of tariffs.
But add in the loss of federal subsidies, and the increase is 114% — or more than double what they currently pay, according to KFF. 22 million out of 24 million marketplace enrollees now receive subsidies.
Premiums in the small group employer market will go up by a median of 11%, also per KFF, due to some of the same reasons insurers cite in ACA markets.
For employer health insurance, there’s no comprehensive data yet for 2026, but estimates from earlier this year put the increases in the high single digits.
Policymakers and advocates often promote drug price transparency to lower costs and improve equity. While transparency is an important first step toward accountability and informed public budgeting, it does not guarantee affordable prices or fair access to medicines.
Transparency Has Some Benefits
Drug price transparency helps show how and why medicines cost what they do along the supply chain (i.e., from the manufacturer to the pharmacy), which makes it easier to identify where costs can be reduced or better regulated. By making this information public, transparency allows patients, payers, and policymakers to make more informed decisions and encourage manufacturers to prices drugs more fairly. Ultimately, it supports a fairer system where patients can better afford and obtain the treatments they need, improving access to care.
States with Drug Transparency Laws
While federal policy to improve price transparency is lacking, the states have moved to make things clearer for patients and payers. Vermont was the first U.S. state to enact a drug price transparency law in 2016. Since then, many others have followed suit. At least 14 states have passed some version of transparency legislation, though the details and their enforcement of these laws differ widely.
For example, only Vermont and Maine require drug companies or insurers to disclose the actual prices paid after discounts (called the “net price”). Alternately, Oregon and Nevada require drug manufacturers to publicly report their profit to state government agencies. And Connecticut, Louisiana, and Nevada mandate pharmacy benefit managers (PBMs) to report the total rebates they receive, but not the amounts for each specific drug. Despite these efforts, no state has yet achieved full transparency across the entire drug supply chain.
Transparency is Not Enough
Even with clear pricing, Americans still pay about 2.6 times more for prescription drugs than people in other wealthy countries. Early evidence suggests that these laws have done little to curb drug prices. To date, only four states – California, Maine, Minnesota, and Oregon – have published analyses of their own laws. These reports share common concerns: difficulty tracking pricing across the supply chain and uncertainty about whether state agencies have the authority (or the will) to act when data is incomplete or unreliable.
Most transparency laws fall short on requiring detailed cost or profit data, focusing instead on broad price trends. As a result, this narrow scope makes it difficult to identify the exact drivers of high drug prices. Even when transparency discourages manufacturers from raising prices, these policies do not directly control pricing or define what constitutes an ‘unjustified’ price increase. Manufacturers can simply adjust by setting higher launch prices or implementing smaller, more frequent increases to stay below reporting thresholds. Still, the result is a system where drug costs can vary by as much as $719 for the same 30-day prescription even when prices are publicly listed.
What can also be done?
Creating a consistent national framework could replace the current patchwork of state laws and improve oversight of how drugs are priced. For example, the Drug Price Transparency in Medicaid Act (H.R. 2450) could do just that: it would standardize reporting requirements and reveal how drug prices are set, rebated, and reimbursed. But transparency alone can’t lower costs—it only shows the problem.
To make transparency meaningful, policymakers must address the underlying contracts and incentives that drive high prices.
Hidden rebate deals and opaque pricing structures between PBMs and drugmakers often inflate costs and limit patients from seeing savings. Transparency legislation should also be paired with value-based pricing that links payments to clinical benefits. Federal programs like the Medicare Drug Negotiation Program provide additional leverage, but broader reforms are needed to reach the commercial market (i.e., where most Americans get their prescription drugs and still face high prices).
Still, transparency can have downsides, especially globally. Fully public drug prices could push companies to stop offering lower prices in low- and middle-income countries. To avoid cross-country comparisons, they could raise prices across the board, making medicines less affordable where they’re needed most. To make transparency more equitable, policymakers should combine disclosure with protections that preserve affordability worldwide.
Conclusion
In short, transparency is necessary but an incomplete fix for America’s drug pricing system. Simply shining a light on how prices are set isn’t enough. Policymakers need to be paired with other reforms, such as removing the incentives that encourage high prices, holding PBMs and manufacturers accountable, extending the negotiating power beyond Medicare, and protecting prescription drug access both at home and abroad. Without these other steps, transparency laws risk highlighting unfairness without actually improving it.
2025 was one of the most turbulent years in modern U.S. healthcare. The headlines were explosive, the rhetoric dramatic and the controversies nonstop. Yet for all the hoopla and upheaval, the medical care Americans received this month looked almost identical to what they experienced on January 1 — except more expensive.
That yearlong pattern (of intense disruption followed by little improvement) played out across nearly every major healthcare storyline.
Luigi Mangioli is preparing to stand trial almost exactly twelve months after the fatal shooting of UnitedHealth CEO Brian Thompson. The killing sparked fears for major health insurers and raised questions about the fragility of the nation’s largest payer. In a February article, I called it a defining moment for UnitedHealth: an opportunity for the company to start competing on health, not denials. But despite the initial shock and ongoing scrutiny, nothing has shifted in how UnitedHealth pays for (or denies) medical care.
Then, in late fall, the nation endured the longest government closure in U.S. history, driven largely by conflicts over healthcare spending and the Affordable Care Act’s health exchanges. However, the eventual resolution to reopen the government came with no respite for the 24 million Americans currently enrolled in an exchange.
For a broader view of the year, here are five major areas of healthcare that generated chaos, confusion and conflict in 2025 – but little meaningful improvement.
1. Political chaos: Turning science into a battleground
No aspect of healthcare saw more volatility in 2025 than in the political arena. The tone was set in January when President Trump returned to office and began reshaping federal health agencies with unprecedented speed.
Within days, he issued a record flurry of executive orders targeting the Affordable Care Act, Medicaid waivers, Medicare Advantage oversight, prior-authorization rules and federal nutrition standards.
He replaced long-entrenched leaders at HHS, NIH, CDC and FDA with political outsiders, many of whose views on vaccines, chronic disease and scientific evidence diverged sharply from the career experts they superseded. The nomination of RFK Jr. to lead HHS became a flashpoint. His reluctance to confront the measles outbreak in Texas, combined with mixed messaging on vaccine policy, have deepened concern for public health.
2. Economic crisis: Costs soar as coverage grew more fragile
Beneath the political theatrics of 2025 was a sobering reality: Americans will once again pay far more for healthcare next year than the year before. And for many, the financial protections that once softened those increases are disappearing.
Insurers on the Affordable Care Act (ACA) marketplace requested median premium hikes of 18% for 2026, the steepest jump since 2018 and well above this year’s 7% hike. If Congress fails to extend the enhanced ACA subsidies, families who once paid affordable monthly premiums will see their costs double or even triple.
The broader economic picture makes these pressures unavoidable. The United States is now spending $5.6 trillion annually on healthcare. National health expenditures are projected to climb another 7.1% this year, far outpacing economic growth. At the same time, federal debt service continues to soar, consuming more of the national budget than Medicaid itself.
The result is an economic crisis hiding in plain sight, one that will increasingly strain the financial, physical and mental health of Americans in the year to come.
3. Regulatory confusion: Agencies rebooted but didn’t improve health
This year shook the foundations of America’s public-health architecture and left yawning gaps where trust, clarity and expert oversight once stood. Politics has replaced science as the primary driver of healthcare policy.
The Centers for Disease Control and Prevention lost its director just weeks after her confirmation. Within days, top-level scientists and center heads resigned en masse, citing political interference and a collapse of scientific independence. Months later, there still is no permanent CDC head.
At the Food and Drug Administration, career reviewers say they’ve been forced to reconsider or abandon scientific best practices. Across both the CDC and FDA, advisory committees that once evaluated evidence through rigorous, peer-driven processes now rely on anecdote and ideology. One striking example is the FDA’s decision to stop requiring hepatitis B vaccination at birth, a move that public-health experts warn could lead to tens of thousands of additional infections for a disease that had been reduced to fewer than 20 annual cases.
Meanwhile, the administration’s sweeping “health-freedom agenda” (under the banner Make America Healthy Again) has identified food packaging, additives, school-lunch standards and “ultra-processed” diets as public-health priorities. But the proposals to improve nutrition remain largely unformed, as the likelihood of meaningful improvements fade.
What remains at year’s end is a set of agencies still functioning, but with public trust weakened and no clear path to rebuilding it.
4. Technological contradiction: AI leapt ahead while medicine stood still
No field generated more excitement, or exposed more contradictions, in 2025 than generative artificial intelligence.
In the broader economy, GenAI models transformed finance, logistics, law, retail and customer service. New large language models, including GPT-5, DeepSeek and Gemini 3, demonstrated near-expert performance on clinical reasoning, interpretation of complex symptoms and risk prediction. Ambient listening matured into a reliable documentation tool, and with the emergence of Artificial General Intelligence (AGI), Americans are relying on large language models when they have medical questions.
Yet inside traditional medicine, progress remains stalled. Clinicians continue to be encouraged to use AI for administrative shortcuts (coding, charting, prior authorization claims) but national specialty organizations haven’t pushed them to use GenAI for diagnosing disease, reducing medical errors or improving clinical outcomes.
Fear of liability has discouraged technology companies from offering GenAI tools that would allow patients to evaluate symptoms or manage their chronic diseases. Yet usage continues to grow. In polling I conducted this fall, 77% of patients and 63% of healthcare professionals reported using a generative-AI tool in the past three months for health-related information or decision support. Meanwhile, medical schools still teach pre-AI workflows, even as medical students and residents turn to GenAI for clinical knowledge and case analysis. The divide between institutional practice and the behaviors of patients and the next generation of physicians is expanding at an accelerating pace.
5. Cultural conflict: A growing divide between the public & the profession
If 2025 revealed anything about American healthcare, it was a widening cultural rift: between younger patients and medical professionals, and between science and public belief.
This rift is felt particularly among Gen Z and Millennials, generations that grew up online, accustomed to second-screen verification and skeptical of traditional authority. As I wrote in 3 Ways Doctors Can Win Back Gen Z And Millennial Patients, younger Americans expect shared decision-making, transparency and digital-first convenience — expectations medicine failed to fulfill in 2025.
At the same time, disinformation and political rhetoric seeped deeper into public life. Social media spread half-truths faster than public-health leaders could correct them. Vaccine skepticism rose thanks to political disinformation. Basic nutritional science became partisan, too. And the public’s confusion only intensified.
What 2025 reveals about the road ahead
By year’s end, one truth became impossible to ignore: despite unprecedented political turmoil, economic instability, scientific breakthroughs and cultural upheaval, the basic structure of American healthcare remained unchanged.
The incentives driving the system, the chronic diseases afflicting the population and the unaffordability confronting families all persist as we enter 2026. At the same time, as generative AI transforms nearly every other sector of the economy, the fax machine remains the most common method physicians use to exchange vital medical information.
The question now is whether mounting economic, political and cultural pressures will finally force American medicine to transform care delivery next year. For more on that, follow me on Forbes and look for my next article on January 5, featuring my healthcare predictions for 2026.
There’s likely to be one more round of health care votes in the House next week after the Senate votes down two rival Affordable Care Act subsidy proposals Thursday — but they won’t get any closer to extending the enhanced subsidies.
Why it matters:
Those subsidies now appear certain to expire at the end of the year, short of a last-minute breakthrough — and out-of-pocket premium costs will more than double on average for roughly 20 million ACA enrollees.
Driving the news:
The Democratic proposal that will get a Senate vote Thursday would extend the enhanced subsidies for three years, while the Senate GOP proposal would not extend the subsidies but instead provide money for health savings accounts.
Both will fail to get the needed 60 votes.
Senate Majority Leader John Thune (R-S.D.) has left the door open for further bipartisan talks after both votes fail, but there is deep skepticism in both parties that any such deal is possible.
Sen. Tim Kaine (D-Va.) said it’s possible there is “additional discussion” after the failed votes, but said the issue also might end up in a “political solution in November when people pick the side that’s for them.”
The latest:
House GOP leaders outlined a range of possible health care options on Wednesday morning, but they have little to do with the subsidies, which weren’t included in their plans.
GOP leaders will bring “consensus” bills to the floor next weekthat aim to lower health care costs, a source who attended House Republicans’ Wednesday morning conference meeting told Axios.
Those could include expanding health savings accounts and association health plans, which allow employers to band together to purchase coverage.
Overhauling pharmacy benefit managers with the goal of lowering drug costs was also discussed, along with funding ACA payments known as cost-sharing reductions (CSRs).
The intrigue:
On the House side, a bipartisan group of moderates including Reps. Brian Fitzpatrick (R-Pa.) and Jared Golden (D-Maine) filed a discharge petition, a procedural move to force a vote on a compromise extension plan.
But that effort to go around House GOP leadership faces long odds against getting the required majority of the chamber to sign on.
Modifications to the subsidies in that plan designed to win over GOP votes, like a crackdown on zero premium plans that backers say fuel fraud, could lose Democratic support due to concerns about coverage loss.
Democratic leaders havebeen focused on a clean three-year extension, saying that is the clearest way to address the issue with little time remaining to implement changes before the new coverage year starts Jan. 1.
House Democratic Leader Hakeem Jeffries (N.Y.) told reporters Wednesday he has no position on the discharge petition.
The bottom line:
There is also deep resistance to a subsidy extension among many Republicans.
Thune has said he thinks Democratic leadership is more interested in a “political messaging” vote this week than in entertaining reforms to the subsidies that Republicans point to.
Even if members in either chamber are able to make progress on a consensus compromise subsidy plan, which in theory could be attached to a government funding bill needed before Jan. 30, the divisive issue of abortion hangs over all of the discussions.
Many Republicans insist on new limits preventing the subsidies from going to insurance plans that cover abortion. Democrats say that is a dangerous expansion of safeguards that already require taxpayer funds to be segregated and not pay for abortion coverage.
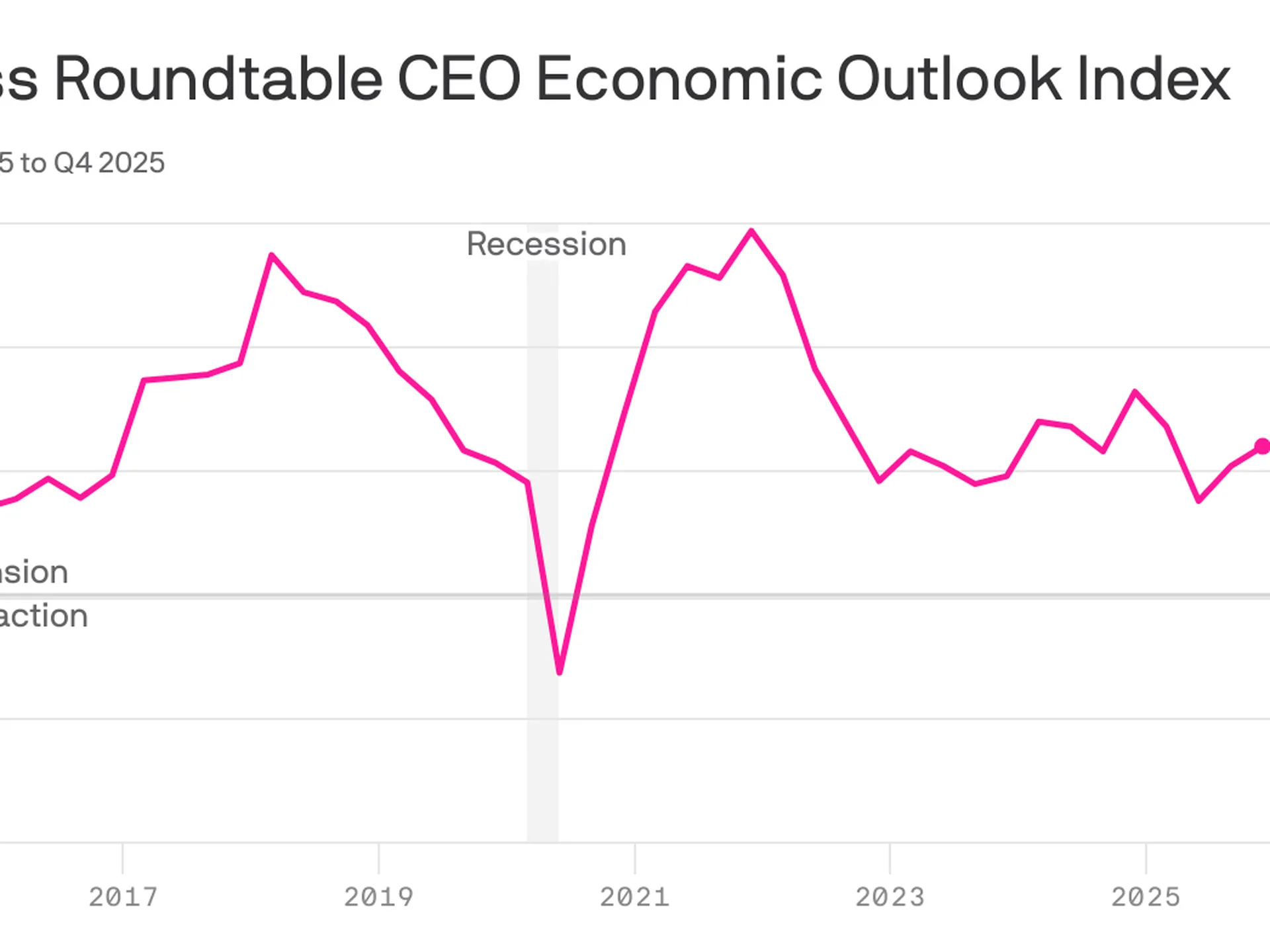
CEO sentiment increasedfor the third consecutive quarter, even as America’s most prominent executives expect underlying job market conditions to remain weak.
Why it matters:
The economic outlook among CEOs has steadily improved since plunging in the aftermath of President Trump’s initiation of the global trade war.
Under the hood, however, there is evidence that structural economic changes — including the proliferation of AI — are weighing on hiring intentions, a warning sign for the labor market.
By the numbers:
The Business Roundtable’s CEO Economic Outlook Index rose by 4 points in its fourth-quarter survey, which was fielded from the final weeks of November through earlier this month.
The index is still shy of the highest level of the Trump 2.0 era and slightly below the historical average of 83.
Zoom in:
The increase reflects a more upbeat view of company revenue in the next six months: Expectations for sales rose 6 points, though the survey does not ask respondents to adjust for the prospect of higher prices.
Plans for capital expenditures — investments in equipment, buildings or software — ticked up 2 points, following a 10-point surge in the previous quarter.
Hiring plans also improved relative to last quarter — up 4 points — though it is the survey’s lone indicator below the level that signals growth.
What they’re saying:
“Notably this quarter, more CEOs plan to reduce employment than increase it for the third quarter in a row – the lowest three-quarter average since the Great Recession,” Business Roundtable CEO Joshua Bolten said in a statement.
About one-quarter of CEOs say they will increase hiring, while 35% say employment will shrink at their respective firms. The remaining 40% plan to keep hiring steady.
A smaller share of CEOs plan to slash workers relative to last quarter, but the figures still show a notable shift among top executives.
Consider the results from this time last year: A similar share of CEOs expected no change in employment levels, but just 21% said they anticipated cutting jobs, while 38% planned to increase hiring.
“CEOs’ softening hiring plans reflect an uncertain economic environment in which AI is driving sizeable [capital expenditures] growth and productivity gains while tariff volatility is increasing costs, particularly for tariff-exposed companies, including small businesses,” Bolten said today.
The big picture:
The in-the-dumps hiring plans signaled by big firm CEOs — alongside a string of layoff announcements in recent months — signal a possible shift for the steady-state labor market that has persisted in recent years.
Powell raised the possibility that the labor market might be even weaker than government data suggests.
The economy has added a monthly average of 40,000 payroll jobs since April. But “we think there’s an overstatement in these numbers, by about 60,000, so that would be negative 20,000 per month,” Powell said at yesterday’s press conference.
“The labor market has continued to cool gradually, maybe just a touch more gradually than we thought,” he added.
The bottom line:
CEOs feel more optimistic, though that confidence boost is not expected to translate into more hiring — an unusual dynamic for the economy.
“Although the results signal that CEOs are approaching the first half of 2026 with some caution, they are starting to see opportunities for growth,” Cisco CEO Chuck Robbins, who chairs the Business Roundtable, said in a statement.
“With the Index near its average, it reflects the resilience of the U.S. economy,” he added, citing pro-growth tax policies and fewer regulations.
The Senate will vote tomorrow on dueling health care plans: Democrats’ proposal to extend enhanced Affordable Care Act subsidies for three years, and a plan from two Republican chairmen that would instead give enrollees funds in health savings accounts.
Why it matters:
The move gives the GOP an alternative to point to if the ACA subsidies expire at the end of the year and health care costs spike for millions of people.
But neither plan is expected to get the 60 votes to advance.
Driving the news:
The plan from Finance Committee chair Mike Crapo (R-Idaho) and health committee Chair Bill Cassidy (R-La.) wouldn’t extend the tax credits past their year-end expiration, instead providing $1,000 to $1,500 in health savings accounts to help certain marketplace enrollees with out-of-pocket costs.
It’s drawn sharp criticism from some Democrats for leaving working-class Americans saddled with high health costs.
Senate Majority Leader John Thune (S.D.) left open the possibility of talks after both votes fail on Thursday, though there is deep skepticism about the chances of reaching a bipartisan agreement.
“If neither proposal gets 60 then we’ll see where it goes from there,” Thune said.
President Trump, asked later about the Crapo-Cassidy bill and whether Republicans should vote for it, told reporters, “I like the concept. … I love the idea of money going directly to the people.”
Between the lines:
On the House side, GOP leadership, committee chairs and leaders of House GOP factions met yesterday to discuss health proposals, with an eye toward a possible House vote this year.
Members left the meeting tight-lipped, saying discussions are ongoing.
The full House Republican conference is expected to discuss health proposals in its meeting this morning ahead of potential votes next week.
For an economy that’s rapidly expanding, the usual drivers of job creation sure aren’t carrying their weight.
Why it matters:
Anemic job growth in key sectors is a sign that there is more underlying weakness in worker demand than the low unemployment rate might suggest.
It makes for a weaker starting point, as companies see new opportunities around the corner to use AI to automate their work.
It’s not a new trend: These sectors showed weak job creation or outright job losses for the last couple of years of the Biden administration.
But it is striking that a GDP surge fueled by data center and AI investment hasn’t been enough to generate more robust hiring.
By the numbers:
Overall employment is up 0.8% over the 12 months ended in September, but the hiring has been driven in significant part by health care, state and local government, and other less cyclical sectors.
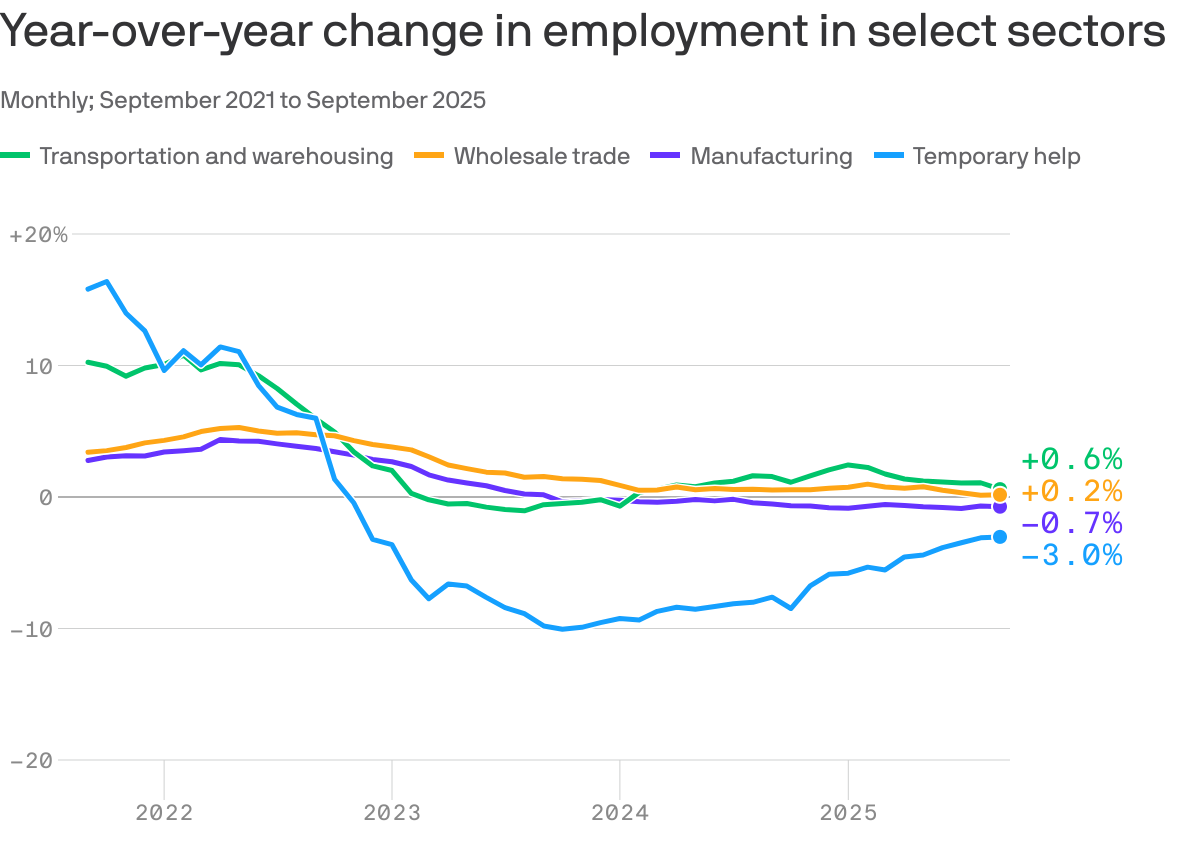
Manufacturing employment is down 0.7% over the last 12 months. Tariffs are weighing on the sector, but its job losses long predate the Trump trade wars, with year-over-year job losses for more than two years.
Temporary help employment, which tends to be a volatile indicator underlying growth trends, is down 3%. It has been losing jobs for three consecutive years.
Two other sectors that tend to correlate with overall economic momentum, transportation and warehousing and wholesale trade, are also adding jobs at rates below that of overall job growth (0.6% and 0.2%, respectively).
Stunning stat:
As Bloomberg flagged, two sectors — health care and social assistance, and leisure and hospitality — accounted for more than 100% of net job gains so far in 2025.
Excluding those sectors, employment dropped by 6,000 jobs in the first nine months of the year.
Zoom out:
There’s not much reason to think these numbers are driven by AI-related opportunities for companies to increase productivity and rely on fewer human workers, particularly given that the phenomenon isn’t new.
But it is more plausible that seeing such opportunities on the horizon has made companies more reluctant to hire in the absence of overwhelming need.
BlackRock chief investment officer for global fixed income Rick Rieder wrote in a note after last week’s jobs report that “what we think we are seeing now is … essentially a hiring pause in anticipation of AI.”
Of note:
A report out this morning from the McKinsey Global Institute finds that AI and robotics technologies could, in theory, automate 57% of U.S. work hours.
“AI will not make most human skills obsolete, but it will change how they are used,” the authors find. “As AI takes on common tasks, people will apply their skills in new contexts,” they write, such as less time researching and preparing documents and more time framing questions and interpreting results.
The bottom line:
Beneath the headline numbers, there is some good reason that attitudes toward the job market are glum.