


Health care’s administrative back end — services like verifying patients’ insurance, putting patients on payment plans and collecting patient debt — is bigger than ever, Axios’ Bob Herman reports.
The big picture: The U.S.’ fractured insurance system leads hospitals and doctors to spend tens of billions of dollars annually on billing software and services — none of which are tied to actual health care.
Driving the news: For-profit hospital system Tenet Healthcare decided to spin off its billing services unit, Conifer, into its own publicly traded entity in 2021.
Between the lines: Many hospital systems that send out bills have ownership stakes in these companies.
Researchers have cited administrative costs as a sizable source of health care waste. Some startups are trying to address this issue, but traditional billing and service firms are only getting larger and have providers as investors.
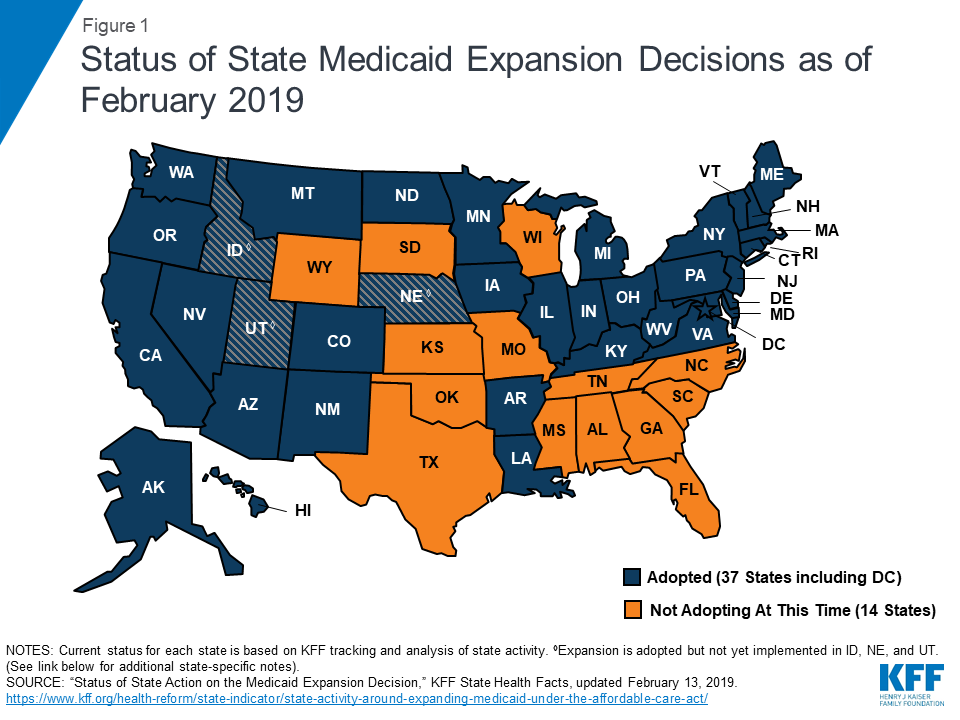
The Trump administration made a very big decision over the weekend: It won’t approve full federal funding for a partial Medicaid expansion.
Why it matters: The partial expansion had looked like a key weapon in red states’ continued resistance to the ACA. Without it, Medicaid enrollment likely will keep growing.
Between the lines: Although the reasoning is different, the Trump administration is now adopting the same policy as the Obama administration — a decision many experts believe the law compels.
Details: Utah voters approved the full ACA expansion last year, but the state legislature overruled them to pass a more limited version.
The intrigue: While the Obama administration rejected these requests on the grounds that federal law dictates the terms of a Medicaid expansion, the Trump administration went a different route, per the Washington Post.
The bottom line: Utah has a backup plan in place — the full Medicaid expansion that Utah residents voted for in the first place.
https://www.cnbc.com/2019/07/28/one-medical-opening-primary-clinics-in-portland-and-atlanta.html

Two years after leaving the traditional health-care world to lead primary care upstart One Medical, Amir Dan Rubin now faces a clear challenge. With competition heating up, he needs to rapidly expand the business into new areas without sacrificing the luxe service that patients have come to expect.
Founded in 2007 by physician-turned-entrepreneur Tom X Lee, One Medical has become popular in and around its hometown of San Francisco by providing on-demand care and easy mobile booking and by selling its services to big companies who offer access as a perk to employees. Google and SpaceX are among those employers, according to a person familiar with the matter who asked not to be named because the relationships are confidential.
One Medical is taking on a chunk of the $3.5 trillion health-care industry, which is riddled with inefficiencies, impersonal care and old technologies that don’t talk to each other and leave patients struggling to find and track their medical records. The company is trying to modernize the whole process, and asks patients to pay a $199 annual membership fee.
“The vision and the focus is to delight millions,” said Rubin, in a recent interview at One Medical’s San Francisco headquarters. “In health care, almost every stakeholder group is frustrated and so we looked to solve a lot of these needs simultaneously by starting from scratch and putting the member at the center of the experience.”
One Medical has 72 clinics in seven states, and Rubin said he’s focused on pushing into new areas. The company is opening locations in Portland, Oregon, as well as Orange County, California, and Atlanta. It’s also partnering with health systems Providence St. Joseph (in Portland and Orange County) and Advocate Aurora (in Chicago), which should lead to more referrals from doctors at those hospitals. Three more Southern California locations are slated to open this month in close collaboration with the University of California San Diego.
To fuel its growth, One Medical raised $220million last year in a funding round led by private equity firm Carlyle Group, bringing total capital raised to more than $400 million, which includes early money from Google Ventures (now GV) and venture firm Benchmark. The latest financing valued the company at about $1.5 billion, according to two people familiar with the matter. That valuation has subsequently edged up to closer to $2 billion based on secondary market transactions, said one of the people, who asked not to be named because the terms are private.
Overall, One Medical says it has 4,000 employers now offering the service as a benefit. But there’s a growing number of emerging competitors bidding for these contracts. They include Premise Health, Paladina, Iora Health, and Crossover Health.
One key piece to One Medical’s strategy is to make it an appealing place for doctors to work. It’s not uncommon for physicians in the U.S. to see 30 or more patients a day and keep visits to less than 10 minutes. One Medical limits doctors to 16 a day. The company also built its own medical records technology from the ground up to help doctors manage patient relationships, a big change from the existing systems that medical professionals say aren’t user friendly.
Providing a service that’s attractive to tech companies gives One Medical a big leg up in going after businesses.
“Historically, you’ve seen a lot of health-care services providers lag behind other consumer-facing industries, and that’s held them back with employers,” said Brian Marcotte, president and CEO of the National Business Group on Health, which represents employers. “They’ve done a better job at One Medical. You can feel it’s different when you walk in the door.”
One Medical is also adding mental health and pediatric services. Its providers are training to treat patients with anxiety and depression, and its clinics have started offering group counseling sessions. Kimber Lockhart, One Medical’s chief technology officer, said these group experiences have proven very popular in tests at various clinics.
Lockhart’s tech team, with occasional advisory help from the doctors on staff, developed an app — Treat Me Now — for patients to get advice on whether to see a doctor or stay at home. It also has an online appointment scheduling system, and a video tool for patients to consult with physicians.
Even with One Medical’s efforts to apply elements of Silicon Valley into its business, the reality is that it runs a health-care operation, which is expensive to manage and comes with high administrative and overhead costs and loads of regulation. So investors have been told to remain patient about a potential IPO.
Steve Wise, a One Medical backer from Carlyle, addressed the road to profitability in a recent interview, when he explained the long-term vision.
“You wouldn’t think a firm like us would invest in a venture-style company that still loses money,” he said. “But it’s a space we know well and we believe in. We want to be the Starbucks of primary care. ”
WATCH: Here’s how One Medical is trying to improve patient experiences

A very small group of patients with major illnesses is responsible for an outsized share of health care spending, and new data show that prescription drugs are a big part of the reason their bills are so high.
The big picture: Among people who get their coverage from a large employer, just 1.3% of employees were responsible for almost 20% of overall health spending, averaging a whopping $88,000 per year.

Red states are getting creative as they look for new ways to limit the growth of Medicaid. But in the process those states are taking legal, political and practical risks that could ultimately leave them paying far more, to cover far fewer people.
Why it matters: Medicaid and the Children’s Health Insurance Program cover more than 72 million Americans, thanks in part to the Affordable Care Act’s Medicaid expansion. Rolling back the program is a high priority for the Trump administration, and it needs states’ help to get there.

Recent news reports indicate that the Trump administration is seeking to authorize states to convert open-ended federal Medicaid funds into a block grant system, and a formal proposal to do so landed at the Office of Management and Budget on June 4. House Democrats have written to Health and Human Services (HHS) secretary Alex Azar to express their concerns about the legal and policy implications of a block grant system.
Not only are there strong legal arguments against efforts to implement a block grant policy, but block grants would also create challenges for states that chose to implement such a program. These legal and policy concerns are foreseeable. The Centers for Medicare and Medicaid Services (CMS) is not only courting yet another legal battle but also threatening access to important health care services—such as prescription drugs, as discussed below—for many of the most vulnerable patients.
The Medicaid Act provides for unlimited federal matching funds for all state spending under Medicaid’s federal rules. This federal match is required by law and encourages states to implement both Medicaid’s mandatory benefits and its optional benefits, such as prescription drugs. This unlimited federal funding also has been central in helping states respond to economic shocks such as recessions and natural disasters and to unplanned programmatic demands such as public health emergencies or expensive new treatments. Switching Medicaid to a block grant program has been proposed by prior administrations and most recently appeared in different bills during the Affordable Care Act repeal-and-replace debates in 2017, but such proposals have been rejected by Congress.
Despite Congress’s refusal to alter Medicaid in this way, and despite long-standing and clear benefits to states of open-ended entitlement funding, the Trump administration has been inviting states, such as Alaska, to discuss capped spending, and other states are poised to respond to the new policy guidance. For example, Alaska commissioned a study of block grants; Tennessee’s legislature enacted a law commanding the governor to seek a block grant; Utah submitted a waiver application seeking per capita caps for Medicaid spending; and Texas commissioned a block grant study in 2017.
To understand this drastic policy change, a little more background is helpful. Medicaid operates through joint funding by states and the federal government, with the federal government matching states’ spending at a set rate that is informed by the per capita income of a state. A poorer state such as Mississippi has a higher federal match rate (76 percent in 2019) than wealthier states (for example, New York at 50 percent). In either case, for every dollar a state spends on Medicaid, it receives a matching amount of federal funds—without limit—making Medicaid a statutory entitlement for states participating in the program.
The federal match developed out of states’ inability to provide adequate medical support for their poor residents. Although the federal government gave states a kind of block grant (grants in aid) before Medicaid was enacted in 1965, the unlimited federal match that the Medicaid Act provides was designed to increase help for poor people while still allowing states to provide for the needs of their particular populations within a federal statutory baseline.
A block grant scheme would be very different from Medicaid’s statutorily required open-ended funding. Caps on spending could be designed in a number of ways, such as a block grant under which states would receive a limited, pre-budgeted amount of money from the federal government, or a per capita cap, which would pre-determine the amount of money spent per person enrolled in Medicaid. No matter the specific form of spending limitation, the administration’s planned policy is not lawful.
More specifically, the administration would have to grant Section 1115 demonstration waivers to states seeking these limits, because the Medicaid Act does not contemplate such spending limitations. Demonstration waivers can be approved under Section 1115 of the Social Security Act, which gives the secretary of HHS authority to waive Section 1902 of the Medicaid Act if a state’s proposed waiver will further the purposes of Medicaid. The goal of these waivers is to allow states to experiment with certain aspects of the Medicaid program to improve beneficiary coverage or care. Section 1115 does not limit federal spending on demonstration waivers, but since the Carter administration, it has been HHS policy to seek federal budget neutrality in 1115 waivers, although states may spend as much as they like.
At least two statutory problems exist for such waivers in this context. First, Medicaid spells out federal payment within Section 1903, which states that the HHS secretary “shall pay to each State…the [federal match] of the total amount expended…as medical assistance under the State plan….” This language is not waivable under Section 1115, which explicitly permits waivers of Section 1902 but not Section 1903. (HHS can approve more spending than Section 1903 contemplates to match a state’s expansion of Medicaid coverage, but it cannot waive Section 1903.) As a result, HHS cannot cap the Medicaid funds it disburses to states, either per person or programmatically, because it must pay the federal match for the “total amount” of a state’s spending. Even if a state wanted to cap its own Medicaid spending, that would necessitate disenrollment and require waiver of many other Medicaid Act requirements such as sufficient state Medicaid funding, equal coverage of beneficiaries across the state, and adequate payment to providers.
Second, block grants are not “likely to assist in promoting the objectives” of Medicaid, the legal standard for HHS to authorize states’ proposals for demonstration waivers. Medicaid’s statutory purpose is to “furnish medical assistance” to eligible beneficiaries, a phrase that recently has been dissected in the context of HHS’s authorization of several 1115 waivers for Medicaid work requirements. The federal court hearing challenges to the legality of work requirements has interpreted “furnish medical assistance” to mean that Medicaid must pay for care, not simply promote a generalized idea of “health” or decrease cost. Spending caps would certainly decrease enrollment (like work requirements already have in Arkansas) and limit care across all kinds of Medicaid coverage, the opposite of furnishing medical assistance.
Any new CMS policy will likely follow the same pattern as the 2018 State Medicaid Director policy letter authorizing work and other conditions of eligibility. That letter promotes waivers for work requirements under the guise of “health” and cost concerns (although, more generally, CMS has been clear that it disagrees with Medicaid expansion). HHS is likely to offer similar reasoning here, allowing new limitations with a predictable impact on the “undeserving” expansion population.
HHS’s recent losses in the work requirement cases may pose an obstacle to capped spending proposals. A recent US Supreme Court case may also create barriers. In Department of Commerce v. New York, the Court concluded that an agency cannot engage in sham regulatory processes. The Roberts-led majority expressed deep concern about the secretary of commerce’s predetermined goal of adding a citizenship question to the 2020 census, calling the secretary’s reasons for adding the question a “pretext” and “contrived” because the publicly stated reason for adding the question was totally unrelated to the actual rationale.
This kind of mismatch is likely to exist in the block grant context as well. No state would be able to serve the purposes of Medicaid, that is, to furnish medical assistance, through a cap on spending, because no matter the structure, such a cap would foreseeably result in disenrollment. But HHS cannot permit state waiver applications that seek to disenroll beneficiaries, which means that HHS and states may offer pretextual reasons for authorizing block grants.
Even putting aside legal obstacles to a capped spending system, block grants are simply bad policy. Proposals of this kind are predictably harmful to both beneficiaries and to state economic interests. The Congressional Budget Office has recognized that block grants encourage states to take actions that include restricting enrollment for legally eligible beneficiaries, limiting mandatory and optional benefits, decreasing already low reimbursement rates (which may lead providers to abandon the program), a combination of all three, and more. In some cases, states may pursue such restrictions but then face unexpected economic pressures, such as a natural disaster or a recession. For example, Puerto Rico, which already exists under an alternative and limited Medicaid program, has experienced these problems acutely in the wake of terrible hurricane damage to the island.
Take just one example of a foreseeable area in which a state might seek to limit benefits under a capped spending regime: prescription drug coverage. Prescription drugs have always been an optional category of care under the Medicaid program, but all states have chosen to cover them. That choice comes with a set of obligations as well as a set of benefits for states and beneficiaries. States must cover essentially all Food and Drug Administration-approved drugs, so that beneficiaries are able to access medically necessary products. However, because this coverage requirement limits states’ bargaining power with drug manufacturers, state Medicaid programs are legally entitled to preferred pricing benefits. Medicaid programs receive large statutory discounts off the average market prices of the products they purchase, obtain the “best price” among private market payers if that price is lower, and are protected if the price of a drug increases faster than inflation.
Even with these discounts, Medicaid prescription drug spending is projected to grow faster than spending on other health care services, putting steady pressure on limited state budgets. These pressures are likely only to increase, as new drugs are introduced at ever-higher launch prices. Indeed, Novartis has just launched a drug with a list price of $2.1 million, setting a new standard. Even if these drugs represent good value for the price, states will struggle even harder to pay for these products if they are operating within an inherently limited monetary environment.
Capped spending would prompt states to make dangerous choices for patients. Initially, states might try to exclude individual drugs from coverage, if only to increase their bargaining power and obtain greater discounts on particular drugs. Massachusetts recently requested a waiver to do just that, asking CMS to allow it to exclude particular drugs from its Medicaid formulary that have demonstrated little or no evidence of efficacy. Massachusetts was undoubtedly concerned that spending on some of these high-cost, low-value drugs was crowding out valuable spending elsewhere in its Medicaid program.
However, CMS denied Massachusetts’ waiver request. Although CMS did not explain the legal reasoning behind its denial, it did suggest that a state may choose to exclude drugs if it forgoes Medicaid’s statutory discounts. This strategy, though, is unlikely to lead to savings larger than the program was able to obtain already. Only if a state severely restricts the drugs it will cover, and therefore severely restricts patients’ access to care, could cost savings occur.
States could make other choices that are even more harmful to patients. For example, nearly half of states impose limits on the number of prescriptions Medicaid beneficiaries are able to fill at one time. States that do not have such policies might adopt them, and states that have already implemented such limitations might seek to tighten them—even though recent research suggests that such limits may be harmful to patients. An extreme cost-cutting decision would be to drop prescription drugs from coverage, although this likely would not be states’ first choice for constraining Medicaid expenditures.
States already have significant flexibility within the Medicaid program, which always has been state specific. The administration’s desired policy change attempts to bypass the law, raising serious separation of powers concerns. And capped spending would very likely involve disenrollment and other cost-cutting measures that endanger the lives of the most vulnerable patients. Under a capped spending policy, it is foreseeable that states would face cost-cutting choices that harm the health of Medicaid beneficiaries of all kinds and especially those relying on access to care such as the medications necessary to manage chronic diseases and other life-threatening conditions.

The Affordable Care Act (ACA) transformed the US health care system by increasing coverage, expanding federal involvement in private health insurance, and changing public expectations for access to affordable coverage. Yet, the ACA did not provide universal coverage and has proven unstable under political and legal attacks since its enactment in 2010. While proposals for replacing the ACA with single-payer health care have attracted national political attention, discussions of a federal single-payer system such as “Medicare for All” remain light on specifics. At the state level, however, state legislators have drafted and introduced dozens of detailed bills to implement single-payer systems. Our study of state single-payer proposals in the ACA era highlights the extent to which states must contort their health reforms to overcome federal legal hurdles—particularly the threat of preemption by the Employee Retirement Income Security Act (ERISA) of 1974—and prompts questions about whether states can actually implement single-payer health care.
We define state single-payer bills as legislative attempts to achieve universal health care coverage for all residents in a state by combining financing for health care services into a single, state-administered payer. Using this definition, we collected and coded bills introduced in state legislatures since 2010, identifying the number of unique proposals by excluding substantially similar legislation introduced in different chambers or with different designations in the same session. From 2010 through 2019, legislators in 20 states have proposed 59 unique single-payer bills (Exhibit 1).
Most, but not all, of the single-payer proposals come from states that expanded Medicaid under the ACA, leaving only a small fraction of the population uninsured. Thus, it appears that beyond achieving universal coverage, state single-payer bills also seek to control health spending through expansive rate-setting authority and streamlined administration, as well as to relieve individuals of their growing out-of-pocket expenses. These state single-payer bills share many common elements: They all provided universal eligibility for state residents, and most also included expansive provider eligibility, rate-setting for health care services and prescription drugs, low or no cost sharing for patients, comprehensive benefits, and limits on the ability of health insurers (but not employers) to offer coverage that duplicates the single-payer benefits.
To finance these universal and comprehensive benefits, state single-payer bills use several strategies to capture health expenditures from the existing multipayer system, while navigating a number of financial and legal impediments. First, the state bills would consolidate federal funds from Medicare, Medicaid, and the ACA exchanges into the state single-payer plan using waiver provisions in those federal programs. The Department of Health and Human Services has considerable discretion to deny state applications for each of these federal waivers; however, and the state bills generally lack fallback plans for capturing federal funds should the agency deny the waivers. Nor do the state single-payer bills confront financial obstacles from state constitutional prohibitions on deficit spending, which constrain state plans when tax revenues fall during economic recession.
Second, but perhaps more crucially, state single-payer bills must find ways to redirect the employer-sponsored health plans that currently cover 49 percent of Americans—a daunting legal task under ERISA. ERISA preempts all state laws that “relate to” employer-sponsored benefits, so states cannot simply mandate that employers cease offering health benefits. States do retain broad power to regulate health care providers and health insurers, but ERISA preempts the application of state insurance regulations to employers’ self-funded health plans, which now comprise more than 60 percent of all employer-sponsored health benefits. ERISA challenges states’ abilities to capture employer health spending—a source of funding that would be critical to the viability of a single-payer system.
The labyrinth of ERISA preemption has inspired creative drafting of state single-payer bills to do indirectly what ERISA prohibits them from doing directly. Our survey revealed three strategies for state bills to capture employer expenditures and move employees into the state single-payer system: levy payroll taxes on employers and income taxes on employees; restrict providers from accepting private-insurer reimbursement; and allow the single-payer plan to pay for all eligible patients’ care, then recoup those payments from other coverage a patient may have. The taxes fund the single-payer plan’s coverage of resident employees and nudge employers to cease offering private coverage. The provider reimbursement restriction further encourages a shift to single-payer coverage by shrinking provider networks for private insurance. The pay-and-recoup provision enables those employers who wish to continue providing benefits to do so without fully eroding the administrative advantages of the single-payer system.
Nearly all states’ bills include one of these strategies; most include a combination of them. Vermont is the only state that has actually enacted single-payer legislation, before abandoning its implementation largely due to the cost of its payroll and income taxes.
To gird against the looming threat of ERISA preemption, state legislatures have resorted to elaborate measures that may dilute their broader aims of achieving universality, solidarity, and efficiency in health care coverage. There are strong legal arguments why provisions to capture employer health spending should survive ERISA preemption. States have wide latitude to levy taxes and regulate health care in general, and providers in particular. The bills’ provisions do not require employers to alter their employee benefit plans, they merely encourage a shift to the state’s health plan. But federal appellate courts have split over the extent to which states may use financial incentives to affect employers’ health benefit decisions. In short, state single-payer plans should survive ERISA preemption, but courts’ unpredictable applications of ERISA cast a pall of uncertainty over the viability of single-payer plans.
State single-payer proposals face formidable legal uncertainties that a federal single-payer plan would not. On the other hand, health reform of this scale presents an experiment well-suited to the laboratories of the states. States’ experimentation with single-payer care could test various models and inform federal health reform debates about the benefits of single-payer over more incremental reforms, or about structuring a single-payer system to minimize disruption for health care providers and patients. The road to reform often starts with the states. This was the path for the ACA, which was first modeled in Massachusetts, and for Canada’s single-payer system, which got its start in Saskatchewan. Significant health reforms tested at the state level may pave the road to better policy at the national level.
While ERISA preemption has bedeviled state health reforms for decades, this wave of state single-payer legislation highlights the depth of the problem. At a time when states are the engines of health policy innovation, ERISA continues to unnecessarily thwart state health reform efforts. Thus, any meaningful health reform should start with ERISA reform. For example, Congress could amend ERISA to narrow its preemption provisions or add a waiver provision similar to other federal health care statutes. While states may successfully contort their health reform efforts to avoid ERISA preemption, they should not have to do so. The time has come to remove ERISA’s obstructions and to unlock states’ capacities as laboratories of health reform.
Most, but not all, of the single-payer proposals come from states that expanded Medicaid under the ACA, leaving only a small fraction of the population uninsured. Thus, it appears that beyond achieving universal coverage, state single-payer bills also seek to control health spending through expansive rate-setting authority and streamlined administration, as well as to relieve individuals of their growing out-of-pocket expenses. These state single-payer bills share many common elements: They all provided universal eligibility for state residents, and most also included expansive provider eligibility, rate-setting for health care services and prescription drugs, low or no cost sharing for patients, comprehensive benefits, and limits on the ability of health insurers (but not employers) to offer coverage that duplicates the single-payer benefits.

Michael Drobot, former owner and CEO of Pacific Hospital in Long Beach, Calif., is currently imprisoned for his role in a kickback scheme, and prosecutors say he has now agreed to plead guilty to new charges.
Mr. Drobot pleaded guilty to charges of conspiracy and paying illegal kickbacks in 2014. He admitted paying millions of dollars in bribes to physicians in exchange for referring thousands of patients to his hospital for spinal surgeries. He was one of several defendants charged for their roles in the kickback scheme, which resulted in the submission of more than $950 million in fraudulent claims.
In January 2018, Mr. Drobot was sentenced to more than five years in prison and ordered to forfeit $10 million to the government, which included the profits from the sale of a 1965 Aston Martin, a 1958 Porsche and a 1971 Mercedes-Benz. Federal prosecutors allege Mr. Drobot violated the order by transferring the Aston Martin to an auction company. Profits from the sale of the vehicle were allegedly transferred to Mr. Drobot’s personal bank account and used for personal expenses, according to MyNewsLA.com.
Prosecutors charged Mr. Drobot with wire fraud, engaging in monetary transactions in property derived from unlawful activity and criminal contempt of court. He is expected to plead guilty to the new charges, which carry a maximum sentence of 50 years, in coming weeks, according to the report.
