

The Democratic presidential primary might feel like a lifetime ago, but one important storyline in that race was health care — specifically single-payer health care, or the policy that the government should offer universal health insurance to everyone in the country. The nomination of now-President Biden, who opposed single-payer health care during the primary, has put single-payer health care on the backburner nationally. But that hasn’t stopped the issue from impacting state legislators, who have introduced more single-payer health care bills in the last few years than ever before.
Health care policy researchers Erin C. Fuse Brown and Elizabeth McCuskey tracked the number of unique single-payer bills introduced in state legislatures across the country from 2010 to 2019, finding a sharp uptick in bills introduced since 2017. During each of those three years, at least 10 single-payer proposals were introduced, according to Brown and McCuskey’s research, for the first time since 2013. In total, state legislators proposed more single-payer bills from 2017 to 2019 than in the previous seven years combined. And for 2021, we’ve identified 10 single-payer bills that legislators introduced across the country, from liberal states like California and Massachusetts to more conservative ones including Iowa and Ohio.1
What do all these proposals have in common? They’ve all universally failed. In fact, Vermont, the only state that managed to pass single-payer health care in 2011, ended up shelving its plan three years later.
It makes sense why single-payer advocates have tried to take these fights to the states. States have traditionally been seen as the “laboratories of democracy,” and some advocates of single-payer health care have argued that liberal states could provide unique opportunities to advance single-payer health care. But as I’ll explain, passing single-payer health care at the state level is next to impossible, as states are particularly limited in how they can allocate federal and private health care funds. There is, however, evidence that Americans may have an appetite for a public option, or government-run health insurance that people can opt into at the state level. Three states (Colorado, Nevada and Washington) have already passed a public option. It’s not single-payer health care reform, but it’s possible that we might see more states adopt their own public-option reforms.
One big reason single-payer proposals haven’t caught on at the state level is because finding a reliable way to pay for such a program is challenging. Single-payer advocates originally envisioned a federal proposal that would cover all Americans under a more generous version of a preexisting program — that is, Medicare, but now for all. Doing this state-by-state would require each state to apply for waivers to divert federal funds used for Medicare, Medicaid and Affordable Care Act exchanges to be used for their own single-payer plans. And that’s tricky because the Department of Health and Human Services has wide discretion to approve or deny states’ requests, which makes any proposal highly dependent on the national political climate.
This isn’t just a theoretical debate either: Trump’s administrator for the Centers for Medicare & Medicaid Services Seema Verma said in 2018 that she would deny waivers from states to create single-payer systems, while Biden’s Health and Human Services Secretary Xavier Becerra has expressed more favorable sentiments. Almost all single-payer proposals depend on these waivers and states don’t often have fallback plans for if this federal funding gets denied.
Employer-sponsored health insurance plans, which cover 54 percent of Americans, are another hurdle for states trying to pass single-payer health care. Federal law largely prevents states from regulating employer-provided health insurance, so states can’t just stop employers from offering their own health care benefits. The exact scope of this law has been litigated for decades, but suffice it to say that it’s successfully put the kibosh on many statewide health care reforms. Single-payer health insurance is particularly tricky as there’s no way to get everyone onto the plan without first changing how private insurance works. States have tried to address this through measures like increasing payroll taxes or restricting providers’ ability to accept reimbursement from private insurance plans. But the more elaborate these mechanisms get, the more complicated it becomes to implement — and the more people that could slip through the cracks.
Finally, another big financial barrier is that state governments have far less leeway than the federal government to increase budgetary spending. That means tax increases, which come with their own political challenges, are often necessary for states to secure the funding they need.
Take California’s single-payer proposal, which failed in late January. It would have required two-thirds of voters to pass a separate constitutional amendment to implement the necessary tax increases to pay for it. Concerns over tax increases also contributed to the demise of single-payer proposals in Colorado and Vermont. It’s true that a recent analysis of New York’s single-payer health care plan found that it would lower overall health care spending by 3 percent by 2031, but it would also require additional state tax revenue of $139 billion in 2022 — over 150 percent of the current state budget. Politicians facing the next election cycle may be leery of proposing short-term tax increases, even if the end result is long-term savings.
All of this creates a daunting picture for statewide single-payer health care. But the failures of single-payer doesn’t entirely close the door on health care reform, especially if these reforms are supplementing the existing system instead of entirely replacing it. Colorado and Nevada, for instance, successfully passed a public option in 2021, joining Washington, which passed one in 2019. Colorado’s success in advancing a public option is particularly striking, given that almost 80 percent of people voted against its single-payer proposal in 2016.
To be sure, though, efforts to implement a public option aren’t without their own challenges. In 2021, during its first year of implementation, Washington state’s public option struggled to enroll people and get health care providers to agree to lower payment rates. State lawmakers have tried to fix this problem by introducing legislation that would require more providers to participate and bring down premiums by increasing subsidies. Proponents have also cautioned that it might take years before the public option really gains a foothold with Washington state residents.
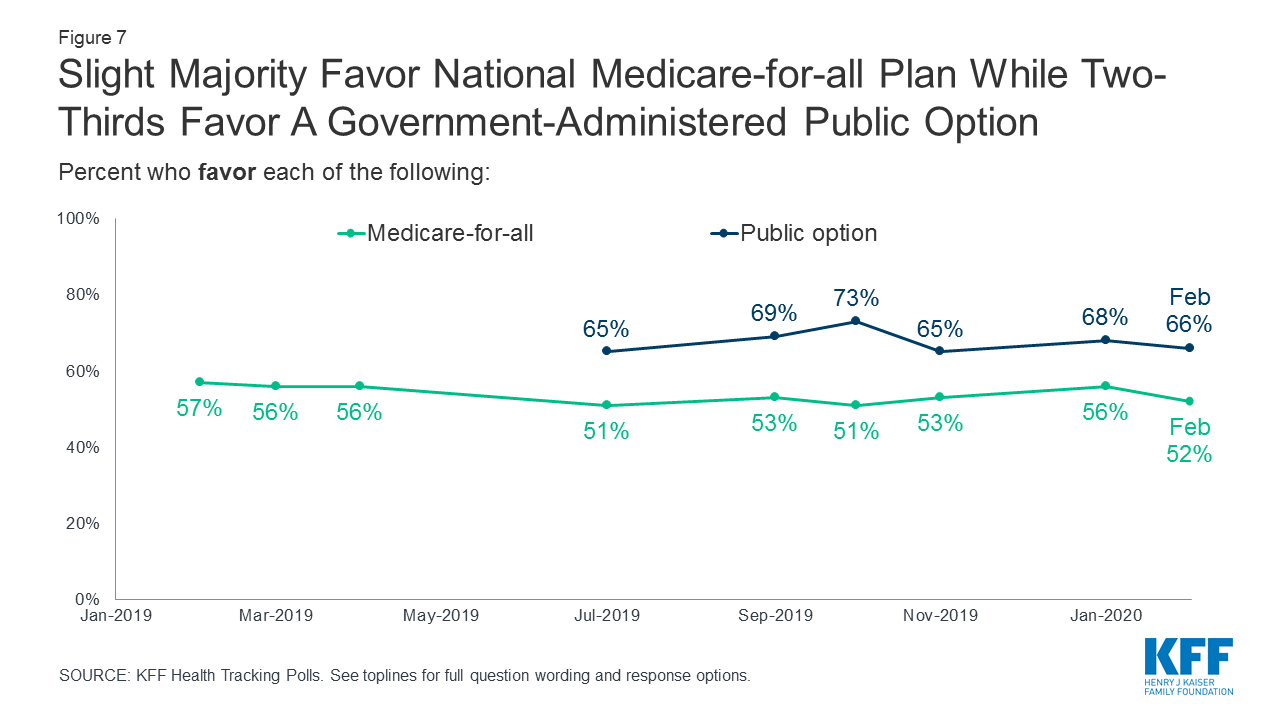
It’s not clear yet how successful these state-run public option plans will be, but it is possible that a public option may prove more popular than single-payer. For starters, while single-payer health care is popular among Democrats, the public option still polls much better among Republicans and independents. According to a Morning Consult/Politico poll from March 2021, the public option was roughly as popular as Medicare for All among Democrats — about 80 percent said they supported each. But support for the public option was much higher than support for Medicare for All among both Republicans and independents. Just 28 percent of Republicans and 50 percent of independents supported Medicare for All versus 56 percent of Republicans and 63 percent of independents who supported a public option.
Moreover, a public option may align more naturally with Americans’ existing views on the role of government in health care. Polls have long found that Americans still want a choice in their health care, even though they believe that providing health insurance to the uninsured is the government’s responsibility.
Ultimately, any health care reforms would be easier to implement on a federal level than a patchwork, state-by-state approach. But Washington, Colorado and Nevada remain important tests of state governments’ ability to implement a public option in lieu of action by the federal government. It’s not single-payer, but it’s still some of the most consequential health care reforms in decades — and a potential sign of where the debates over health care are heading.








{kind=link}