New York state declared an imminent threat and San Francisco issued a state of emergency over monkeypox July 28 as the virus continues to spread in the U.S., NBC News reported.
The news comes after the World Health Organization declared monkeypox a global emergency July 23 and as the CDC reported 4,907 confirmed cases nationwide as of July 28. California and New York account for more than 40 percent of the reported cases in the U.S., according to The Washington Post.
In a statement, New York State Commissioner of Health Mary Bassett, MD, said the declaration allows local health departments “to access additional state reimbursement, after other federal and state funding sources are maximized, to protect all New Yorkers and ultimately limit the spread of monkeypox in our communities.” It covers monkeypox prevention response and activities from June 1 through the end of the year.
In San Francisco, the monkeypox public health emergency takes effect Aug. 1, city officials said in a news release. The release, from Mayor London Breed and the San Francisco Department of Public Health, said the declaration “will mobilize city resources, accelerate emergency planning, streamline staffing, coordinate agencies across the city, allow for future reimbursement by the state and federal governments and raise awareness throughout San Francisco about [monkeypox].”
Four other updates:
1. HHS announced July 28 that nearly 800,000 additional monkeypox vaccine doses will be available for distribution to states and jurisdictions. The 786,000 additional doses are on top of the more than 300,000 doses already distributed. This means the U.S. has secured a total of about 1.1 million doses “that will be in the hands of those who need them in the next several weeks,” HHS Secretary Xavier Becerra said during a July 28 news conference. The additional doses will be allocated based on the total population of at-risk people and the number of new cases in each jurisdiction. “This strategy ensures that jurisdictions have the doses needed to complete the second dose of this two-dose vaccine regimen for those who have been vaccinated over the past month,” HHS said in a news release.
2. As of the morning of July 29, the U.S. has held off on declaring a national monkeypox emergency. Mr. Becerra said July 28 that HHS “continue[s] to monitor the response throughout the country on monkeypox” and will weigh any decision regarding a public health emergency declaration based on the response.
3. The monkeypox response is straining public health workers. Health experts are concerned over how the monkeypox response will further deplete the nation’s public health workforce, still strained and burnt out from the ongoing COVID-19 pandemic. Barriers to testing, treatment and vaccine access largely mirror the missteps in the early coronavirus response, Megan Ranney, MD, emergency physician and academic dean of Brown University School of Public Health in Providence, R.I, told The Washington Post. “I can’t help but wonder if part of the delay is that our public health workforce is so burned out,” she said. “Everyone who’s available to work on epidemiology or contract tracing is already doing it for COVID-19.”
4. Monkeypox testing demand is low, commercial laboratories told CNN. In recent weeks, five major commercial laboratories have begun monkeypox testing, giving the nation capacity to conduct 80,000 tests per week. While Mayo Clinic Laboratories can process 1,000 samples a week, it’s received just 45 specimens from physicians since it began monkeypox testing July 11, according to the July 28 CNNreport. “Without testing, you’re flying blind,” William Morice, MD, PhD, president of Mayo’s lab and chair of the board of directors at the American Clinical Laboratory Association, told the news outlet. “The biggest concern is that you’re not going to identify cases and [monkeypox] could become an endemic illness in this country. That’s something we really have to worry about.”
The COVID-19 pandemic is still fresh in the minds of the people around the world, so it comes as no surprise that recent outbreaks of another virus are grabbing headlines.
Monkeypox outbreaks have now been reported in multiple countries, and it has scientists paying close attention. For everyone else, numerous questions come to the surface:
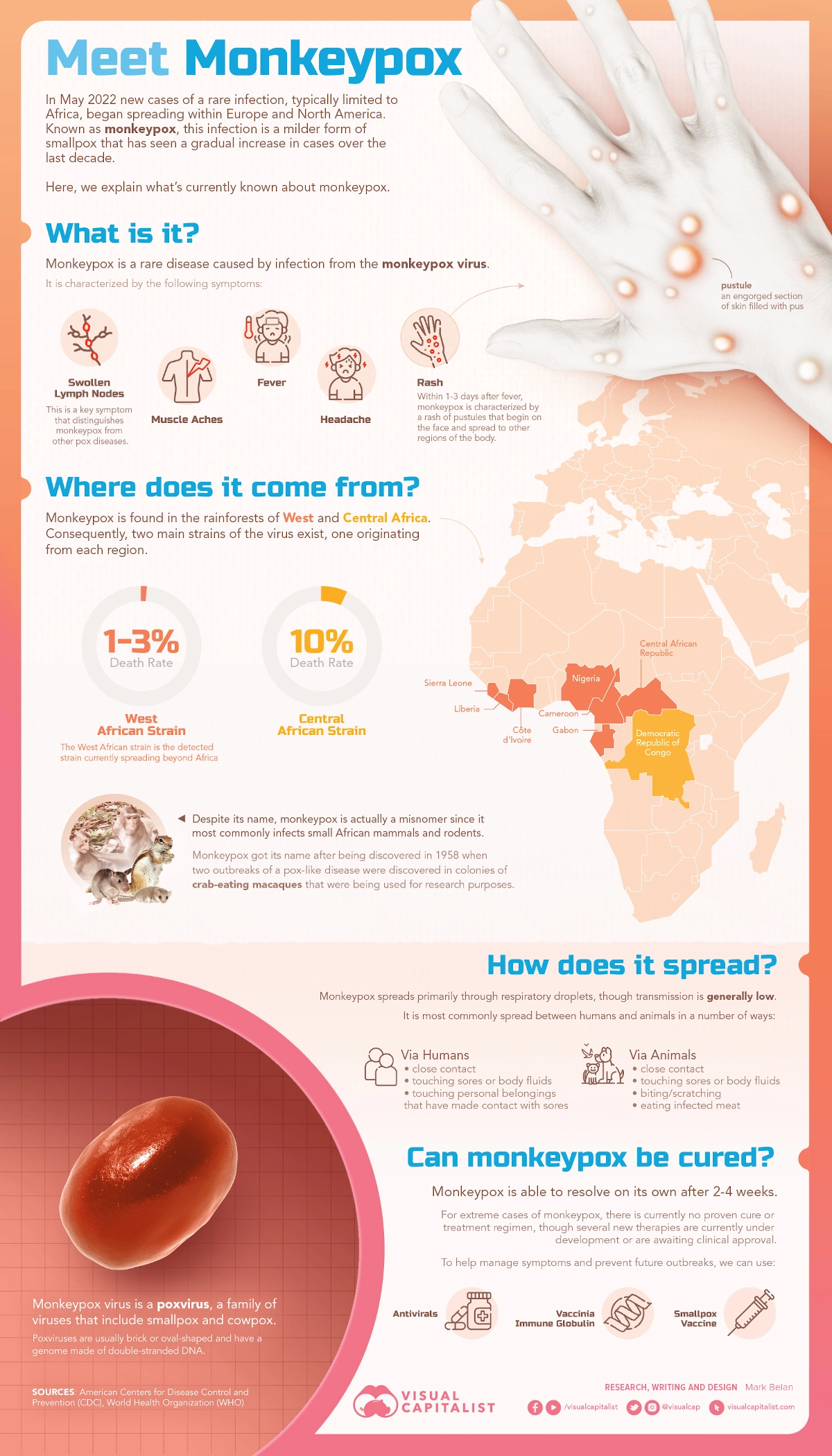
Monkeypox is a virus in the Orthopoxvirus genus which also includes the variola virus (which causes smallpox) and the cowpox virus. The primary symptoms include fever, swollen lymph nodes, and a distinctive bumpy rash.
There are two major strains of the virus that pose very different risks:
Congo Basin strain: 1 in 10 people infected with this strain have died
West African strain: Approximately 1 in 100 people infected with this strain died
At the moment, health authorities in the UK have indicated they’re seeing the milder strain in patients there.
Where did Monkeypox Originate From?
The virus was originally discovered in the Democratic Republic of Congo in monkeys kept for research purposes (hence the name). Eventually, the virus made the jump to humans more than a decade after its discovery in 1958.
It is widely assumed that vaccination against another similar virus, smallpox, helped keep monkeypox outbreaks from occurring in human populations. Ironically, the successful eradication of smallpox, and eventual winding down of that vaccine program, has opened the door to a new viral threat. There is now a growing population of people who no longer have immunity against the virus.
Now that travel restrictions are lifting in many parts of the world, viruses are now able to hop between nations again. As of the publishing of this article, a handful of cases have now been reported in the U.S., Canada, the UK, and a number of European countries.
On the upside, contact tracing has helped authorities piece together the transmission of the virus. While cases are rare in Europe and North America, it is considered endemic in parts of West Africa. For example, the World Health Organization reports that Nigeria has experienced over 550 reported monkeypox cases from 2017 to today. The current UK outbreak originated from an individual who returned from a trip to Nigeria.
Could Monkeypox become a new pandemic?
Monkeypox, which primarily spreads through animal-to-human interaction, is not known to spread easily between humans. Most individuals infected with monkeypox pass the virus to between zero and one person, so outbreaks typically fizzle out. For this reason, the fact that outbreaks are occurring in several countries simultaneously is concerning for health authorities and organizations that monitor viral transmission. Experts are entertaining the possibility that the virus’ rate of transmission has increased.
Images of people covered in monkeypox lesions are shocking, and people are understandably concerned by this virus, but the good news is that members of the general public have little to fear at this stage.
I think the risk to the general public at this point, from the information we have, is very, very low. –TOM INGLESBY, DIRECTOR, JOHNS HOPKINS CENTER FOR HEALTH SECURITY
Epidemiologist Luke Nyakarahuka sprays disinfectant on scientists Jonathan Towner and Brian Amman in Queen Elizabeth National Park, Uganda, in 2018. The scientists were researching how bats transmit the Marburg virus to humans.
After the coronavirus pandemic and the rise of monkeypox cases, news of another virus can trigger nerves globally. The highly infectious Marburg virus has been reported in the West African country of Ghana this week, according to the World Health Organization.
Two unrelated people died after testing positive for Marburg in the southern Ashanti region of the country, the WHO said Sunday, confirming lab results from Ghana’s health service. The highly infectious disease is similar to Ebola and has no vaccine.
Health officials in the country say they are working to isolate close contacts and mitigate the spread of the virus, and the WHO is marshaling resources and sending specialists to the country.
“Health authorities have responded swiftly, getting a head start preparing for a possible outbreak. This is good because without immediate and decisive action, Marburg can easily get out of hand,” said the WHO’s regional director for Africa, Matshidiso Moeti.
Fatality rates from the disease can reach nearly 90 percent, according to the WHO.
Here’s what we know about the virus:
What is the Marburg virus?
Marburg is a rare but highly infectious viral hemorrhagic fever and is in the same family as Ebola, a better-known virus that has plagued West Africa for years.
The Marburg virus is a “genetically unique zoonotic … RNA virus of the filovirus family,” according to the Centers for Disease Control and Prevention. “The six species of Ebola virus are the only other known members of the filovirus family.”
Fatality rates range from 24 percent to 88 percent, according to the WHO, depending on the virus strain and quality of case management.
Marburg has probably been transmitted to people from African fruit bats as a result of prolonged exposure from people working in mines and caves that have Rousettus bat colonies. It is not an airborne disease.
Once someone is infected, the virus can spread easily between humans through direct contact with the bodily fluids of infected people such as blood, saliva or urine, as well as on surfaces and materials. Relatives and health workers remain most vulnerable alongside patients, and bodies can remain contagious at burial.
The first cases of the virus were identified in Europe in 1967. Two large outbreaks in Marburg and Frankfurt in Germany, and in Belgrade, Serbia, led to the initial recognition of the disease. At least seven deaths were reported in that outbreak, with the first people infected having been exposed to Ugandan imported African green monkeys or their tissue while conducting lab research, the CDC said.
Where has Marburg been detected?
The Ghana cases are only the second time Marburg has been detected in West Africa. The first reported case in the region was in Guinea last year. The virus can spread quickly. More than 90 contacts, including health workers and community members, are being monitored in Ghana. The WHO said it has also reached out to neighboring high-risk countries to put them on alert.
Cases of Marburg have previously been reported elsewhere in Africa, including in Uganda, the Democratic Republic of Congo, Kenya, South Africa and Zimbabwe. The largest outbreak killed more than 200 people in Angola in 2005.
The virus is not known to be native to other continents, such as North America, and the CDC says cases outside Africa are “infrequent.” In 2008, however, a Dutch woman died of Marburg disease after visiting Uganda. An American tourist also contracted the disease after a Uganda trip in 2008 but recovered. Both travelers had visited a well-known cave inhabited by fruit bats in a national park.
What are the symptoms?
The illness begins “abruptly,” according to the WHO, with a high fever, severe headache and malaise. Muscle aches and cramping pains are also common features.
In Ghana, the two unrelated individuals who died experienced symptoms such as diarrhea, fever, nausea and vomiting. One case was a 26-year-old man who checked into a hospital on June 26 and died a day later. The second was a 51-year-old man who went to a hospital on June 28 and died the same day, the WHO said.
In fatal cases, death usually occurs between eight and nine days after onset of the disease and is preceded by severe blood loss and hemorrhaging, and multi-organ dysfunction.
The CDC has also noted that around day five, a non-itchy rash on the chest, back or stomach may occur. Clinical diagnosis of Marburg “can be difficult,” it says, with many of the symptoms similar to other infectious diseases such as malaria or typhoid fever.
Can Marburg be treated?
There are no vaccines or antiviral treatments approved to treat the Marburg virus.
However, supportive care can improve survival rates such as rehydration with oral or intravenous fluids, maintaining oxygen levels, using drug therapies and treating specific symptoms as they arise. Some health experts say drugs similar to those used for Ebola could be effective.
Some “experimental treatments” for Marburg have been tested in animals but have never been tried in humans, the CDC said.
Virus samples collected from patients to study are an “extreme biohazard risk,” the WHO says, and laboratory testing should be conducted under “maximum biological containment conditions.”
Anything else to know?
The WHO said this week it is supporting a “joint national investigative team” in Ghana and deploying its own experts to the country. It is also sending personal protective equipment, bolstering disease surveillance and tracing contacts in response to the handful of cases.
More details are likely to be shared at a WHO Africa online briefing scheduled for Thursday.
“It is a worry that the geographical range of this viral infection appears to have spread. This is a very serious infection with a high mortality rate,” international public health expert and professor Jimmy Whitworth of the London School of Hygiene and Tropical Medicine told The Washington Post on Monday.
“It is important to try to understand how the virus got into the human population to cause this outbreak and to stop any further cases. At present, the risk of spread of the outbreak outside of Ashanti region of Ghana is very low,” he added.
As this summer heats up, so has the spread of the hot new version of COVID-19.
Why it matters: This subvariant of Omicron called BA.5 — the most transmissible subvariant yet — quickly overtook previous strains to become the dominant version circulating the U.S. and much of the world.
BA.5 is so transmissible — and different enough from previous versions — that even those with immunity from prior Omicron infections may not have to wait long before falling ill again.
What they’re saying: “I had plenty of friends and family who said: ‘I didn’t want to get it but I’m sort of glad I got it because it’s out of the way and I won’t get it again’,” Bob Wachter, chairman of the University of California, San Francisco Department of Medicine told Axios. “Unfortunately that doesn’t hold the way it once did.”
“Even this one bit of good news people found in the gloom, it’s like, ‘Sorry’,” Wachter said.
State of play: This week, the CDC reported BA.5 became the dominant variant in the U.S., accounting for nearly 54% of total COVID cases. Studies show extra mutations in the spike protein make the strain three or four times more resistant to antibodies, though it doesn’t appear to cause more serious illness.
Hospital admissions are starting to trend upward again, CDC data shows, though they’re still well below what was seen during the initial spread of Omicron.
It’s unclear whether that could be indicating an increase in patients in for COVID, or patients who happen to have COVID, Wachter said. “We’re up in hospitalizations around 20% but with a relatively small number of ICU patients,” Wachter said about COVID cases at UCSF.
In South Africa, the variant had no impact on hospitalizations while Portugal saw hospitalizations rise dramatically, Megan Ranney, academic dean at the Brown University School of Public Health told Axios.
“So the big unknown is what effect it’s going to have on the health care system and the numbers of folks living with long COVID,” she said.
Yes, but: “I’m certainly hearing about more reinfections and more fairly quick reinfections than at any other time in the last two and a half years,” Wachter said.
Zoom in: That is also largely the experience of the surge seen firsthand in New York City by Henry Chen, president of SOMOS Community Care, who serves as a primary care physician across three boroughs of the city.
With this particular variant, he said: “The symptoms are pretty much the same but a little bit more severe than the last wave. It’s more high fever, body ache, sore throat and coughing,” Chen said, adding his patient roster is mostly vaccinated.
But it is occurring among patients who’d gotten the virus only three or four months ago, he said.
The big picture: Another summertime wave of cases could prolong the pandemic, coming after many public health precautions were lifted and with available vaccines losing their efficacy against the ever-evolving virus.
The bottom line: The messaging isn’t to panic, but to understand the virus is likely spreading in local communities much more than individuals realize due to shrinking testing programs — and without the level of protection they might assume they have.
“If you don’t want to get sick, you still need to be taking at least some precautions,” Ranney said. “[COVID] is still very much among us.”
Numerous viruses that were seemingly dormant during the pandemic are returning in new and atypical ways, CNBC reported June 10.
Flu, respiratory syncytial virus, adenovirus, tuberculosis and monkeypox are among the viruses that have recently surged or exhibited unusual behaviors.
The U.S. saw extremely mild flu seasons in 2020-21 and 2021-22, likely due to high rates of mask-wearing, social distancing and other COVID-19 prevention measures. However, flu cases started to rise this February and continued to climb through the spring as more public health measures receded.
“We’ve never seen a flu season in the U.S. extend into June,” Scott Roberts, MD, associate medical director for infection prevention at Yale New Haven (Conn.) Hospital, told CNBC. “COVID has clearly had a very big impact on that. Now that people have unmasked [and] places are opening up, we’re seeing viruses behave in very odd ways that they weren’t before.”
Washington state is also reporting its most severe tuberculosis outbreak in 20 years, while the world is grappling with a monkeypox outbreak that’s affected more than 1,000 people.
These viruses, suppressed during the pandemic, now have more opportunities to spread as people resume daily life, become more social and travel more. Society, as a whole, also has less immunity against the viruses after two years of reduced exposure to them, according to the report.
The pandemic has also boosted surveillance efforts and public interest in other outbreaks, experts say.
“COVID has raised the profile of public health matters so that we are perhaps paying more attention to these events when they occur,” Jennifer Horney, PhD, professor of epidemiology at the University of Delaware in Newark, told CNBC.
A friend called me for medical advice two weeks ago. He’s single, in his thirties and generally healthy, but he’d developed a dry cough with mild congestion. After a self-administered Covid-19 test turned up negative results, he remained suspicious he could be infected.
He was set to fly west in a couple of days for a conference and dreaded the thought of infecting other passengers. I recommended a PCR test if he wanted to be more certain. When the lab results came back positive, he spent the next five days at home alone (per CDC guidance).
If you were in his shoes, chances are you, too, would make a reasonable effort to avoid infecting others. In the near future, that won’t be the case.
Americans are playing it safe—for now
A whopping 91% of Americans no longer consider Covid-19 a “serious crisis.” Social distancing has reached a low point as public-health restrictions continue to ease up.
Yet, there’s still one aspect of the pandemic Americans are taking very seriously.
As a society, we still expect people who test positive for Covid-19 to stay home and minimize contact with others. As a result of these expectations, 4 in 10 workers (including 6 in 10 low-income employees) have missed work in 2022. Overall, the nation’s No. 1 concern related to Omicron is “spreading the virus to people who are at higher risk of serious illness.”
Most Americans are eager to move on from the pandemic, but those who are sick continue to avoid actions that may potentially spread the virus.
Call it what you will—group think, peer pressure or the fear of violating cultural taboos—people don’t want to put others in harm’s way. That’s true, according to polls, regardless of one’s party affiliation or vaccination status.
What’s immoral today will be appropriate tomorrow
Don’t get used to these polite and socially conscious behaviors. All of it is about to change in the not-distant future. Let me paint a picture of tomorrow’s new normal:
A factory worker tests positive over the weekend for Covid-19 and comes to work on Monday without a mask, informing no one of his infection.
A vacationer with mild Covid-19 symptoms refuses to postpone her spa weekend, availing herself of massages, facials and group yoga classes.
A couple plans an indoor wedding for 200-plus, knowing the odds are likely that dozens of people will get infected and that some of those guests will be elderly and immunosuppressed.
These actions, which seem inappropriate and immoral now, will become typical. It’s not that people will suddenly become less empathetic or more callous. They’ll simply be adjusting to new social mores, brought about by a unique viral strain and an inevitable evolution in American culture.
A crash course in a unique virus
To understand why people will behave in ways that seem so unacceptable today, you must understand how the Omicron variant spreads compared to other viruses.
Scientists now know that Omicron (and its many decimal-laden strains: BA.2, BA.2.12.1, BA.4, BA.5, etc.) is the most infectious, fastest-spreading respiratory virus in world history. The Mayo Clinic calls this Covid-19 variant “hyper-contagious.”
“A single case could give rise to six cases after four days, 36 cases after eight days, and 216 cases after 12 days,” according to a report in Scientific American. As a result, researchers predict that 100 million Americans will become infected with Omicron this year alone—via new infections, reinfections and vaccination breakthroughs.
In addition to Omicron’s high transmissibility, the virus is also season-less. Whereas influenza arrives each winter and exits in the spring, Americans will continue to experience high levels of Covid-19 infection year-round—at least for the foreseeable future.
With its 60-plus mutations, immense transmissibility and lack of seasonality, Omicron is an exceptional virus: one that will infect not only our respiratory systems but also our culture.
Over time, Omicron’s unique characteristics will drive Americans to deny and ignore the risks of infection. In the near future, they’ll make decisions and take actions that they’d presently deem wrong.
A culture shock is coming
Culture—which comprises the shared values, norms and beliefs of a group of people—doesn’t change because someone decides it should. It evolves because circumstances change.
The pandemic has no doubt been a culture-changing event and, as the circumstances of Covid-19 have changed, so too have our underlying values, beliefs and behaviors.
If 100 million Americans (one-third of the population) were to become infected with Omicron this year, we can expect that everyone will know someone with the disease. And when dozens of our friends or colleagues say they’ve had it, we will begin to see transmission as inevitable. And since, statistically, most Americans won’t die from Omicron, people will see infection as relatively harmless and they’ll be willing to drop their guard.
We’ll see more and more people going to work even when they’re infected. We’ll see more people on trains and planes, coughing and congested, having never taken a Covid-19 test. And we’ll see large, indoor celebrations taking place without any added safety measures, despite the risks to the most vulnerable attendees.
Amid these changes, health officials will continue to urge caution, just as they have for more than two years. But it won’t make a difference. Culture eats science for breakfast. Americans will increasingly follow the herd and stop heeding public-safety warnings.
The process of change has begun
Cultural shifts happen in steps. First, a few people break the rules and then others follow.
Recall my friend, the one who took two tests out of an abundance of caution. Next time, perhaps he’ll decide he’d rather not miss the conference. Perhaps when he returns home, he will tell his friends that he felt sick the whole trip. Perhaps they’ll ask, “Do you think you might have had Covid?” And perhaps he will reply: “What difference would it have made? I’m fully vaccinated and boosted.”
And so, it will go. The next time someone in his social circle feels under the weather, he or she won’t even bother to do the first test.
This change process has already begun. Take the White House Correspondents’ Dinner, for example. Last year, the event was cancelled. This year, guests had to show proof of vaccination or a negative same-day test. However, that rule didn’t apply to staff at the hotel who worked the event. Unsurprisingly, several high-profile attendees got Covid-19 but, so far, no reports of anyone being hospitalized. A year from now, assuming no major mutations cause the virus to become more lethal, we can expect all restrictions will be dropped.
Culture dictates how people behave. It influences their thoughts and actions. It alters their values and beliefs. The unique characteristics of Omicron will lead people to ignore the harm it inflicts. They won’t act with malicious intent. They’ll just be oblivious to the consequences of their actions. That’s how culture works.
But officials caution that people should not presume they have protection against the virus going forward.
Before omicron, one-third of Americans had been infected with the coronavirus, but by the end of February, that rate had climbed to nearly 60 percent — including about 75 percent of kids and 60 percent of people age 18 to 49, according to federal health data released Tuesday.
The data from blood tests offers the first evidence that over half the U.S. population, or 189 million people have been infected at least once since the pandemic began — double the number reflected in official case counts. Officials cautioned, however, that the data, in a report from the Centers for Disease Control and Prevention, does not indicate people have protection against the virus going forward, especially against increasingly transmissible variants.
“We continue to recommend that everyone be up to date on their vaccinations, get your primary series and booster, when eligible,” CDC Director Rochelle Walensky said during a media briefing.
Kristie Clarke, the CDC official who authored the report, said by February, “evidence of previous COVID-19 infections substantially increased among every age group, likely reflecting the increase in cases we noted as omicron surged in this country.”
Clarke said the greatest increases took place in those with the lowest levels of vaccination, noting that older adults were more likely to be fully vaccinated.
The largest increases were in children and teenagers through age 17 — about 75 percent of them had been infected by February, based on blood samples that look at antibodies developed in response to a coronavirus infection but not in response to vaccination. That’s about 58 million children.
The blood test data suggests 189 million Americans had covid-19 by end of February, well over double the 80 million cases shown by The Washington Post case tracker, which is based on state data of confirmed infections. Clarke said that’s because the blood tests captures asymptomatic cases and others that were never confirmed on coronavirus tests.
With the omicron surge, officials had expected there would be more infections. “But I didn’t expect the increase to be quite this much,” Clarke added.
Separately, CDC is about to publish another study that estimates three infections for every reported case, she said.
A surge in coronavirus infections in Western Europe has experts and health authorities on alert for another wave of the pandemic in the United States, even as most of the country has done away with restrictions after a sharp decline in cases.
Infectious-disease experts are closely watching the subvariant of omicron known as BA.2, which appears to be more transmissible than the original strain, BA.1, and is fueling the outbreak overseas.
In all, about a dozen nations are seeing spikes in coronavirus infections caused by BA.2, a cousin of the BA.1 form of the virus that tore through the United States over the past three months.
In the past two years, a widespread outbreak like the one now being seen in Europe has been followed by a similar surge in the United States some weeks later. Many, but not all, experts interviewed for this story predicted that is likely to happen. China and Hong Kong, on the other hand, are experiencing rapid and severe outbreaks, but the strict “zero covid” policies they have enforced make them less similar to the United States than Western Europe.
A number of variables — including relaxed precautions against viral transmission, vaccination rates, the availability of antiviral medications and natural immunity acquired by previous infection — may affect the course of any surge in the United States, experts said.
Most importantly, it is unclear at this point how many people will become severely ill, stressing hospitals and the health-care system as BA.1 did.
Another surge also may test the public’s appetite for returning to widespread mask-wearing, mandates and other measures that many have eagerly abandoned as the latest surge fades and spring approaches, experts said.
“It’s picking up steam. It’s across at least 12 countries … from Finland to Greece,” said Eric Topol, director of the Scripps Research Translational Institute in San Diego, who recently posted charts of the outbreak on Twitter. “There’s no question there’s a significant wave there.”
Topol noted that hospitalizations for covid-19, the disease caused by the virus, are rising in some places as well, despite the superior vaccination rates of many Western European countries.
At a briefing Monday, White House press secretary Jen Psaki said about 35,000 cases of BA.2 have been reported in the United States to date. But she offered confidence that “the tools we have — including mRNA vaccines, therapeutics and tests — are all effective tools against the virus. And we know because it’s been in the country.”
Kristen Nordlund, a spokeswoman for the Centers for Disease Control and Prevention, said in an email Tuesday that “although the BA.2 variant has increased in the United States over the past several weeks, it is not the dominant variant, and we are not seeing an increase in the severity of disease.”
The seven-day average of cases in the United States fell 17.9 percent in the past week, according to data tracked by The Washington Post, while the number of deaths dropped 17.2 percent and hospitalizations declined 23.2 percent.
Predicting the future course of the virus has proved difficult throughout the pandemic, and the current circumstances in Europe elicited a range of opinions from people who have closely tracked the pathogen and the disease it causes.
In the United States, just 65.3 percent of the population, 216.8 million people, are fully vaccinated, and only 96.1 million have received a booster shot, according to data tracked by The Post. In Germany, nearly 76 percent are fully vaccinated, according to the Johns Hopkins data, and the United Kingdom has fully vaccinated 73.6 percent.
That lower vaccination rate is very likely to matter as BA.2 spreads further in the United States, especially in regions where it is significantly lower than the national rate, several experts said. And even for people who are fully vaccinated and have received a booster shot, research data is showing that immunity to the virus fades over time. Vaccine-makers Pfizer and BioNTech asked the Food and Drug Administration on Tuesday for emergency authorization to offer a fourth shot to people 65 and older.
“Any place you have relatively lower vaccination rates, especially among the elderly, is where you’re going to see a bump in hospitalizations and deaths from this,” said Céline Gounder, an infectious-diseases physician and editor at large for public health at Kaiser Health News.
Similarly, as the public sheds masks — every state has dropped its mask mandate or announced plans to do so — another layer of protection is disappearing, several people tracking the situation said.
“Why wouldn’t it come here? Are we vaccinated enough? I don’t know,” said Kimberly Prather, a professor of atmospheric chemistry and an expert on aerosol transmission at the University of California at San Diego.
“So I’m wearing my mask still. … I am the only person indoors, and people look at me funny, and I don’t care.”
Yet BA.2 appears to be spreading more slowly in the United States than it has overseas, for reasons that aren’t entirely clear, Debbie Dowell, chief medical officer for the CDC’s covid-19 response, said in a briefing Saturday for clinicians sponsored by the Infectious Diseases Society of America.
“The speculation I’ve seen is that it may extend the curve going down, case rates from omicron, but is unlikely to cause another surge that we saw initially with omicron,” Dowell said.
One reason for that may be the immunity that millions of people acquired recently when they were infected with the BA.1 variant, which generally caused less-severe illness than previous variants. Yet no one really knows whether infection with BA.1 offers protection from BA.2.
“That’s the question,” said Jeffrey Shaman, an epidemiologist at the Columbia University Mailman School of Public Health. “Better yet, how long does it provide protection?”
Topol said the United States needs to improve its vaccination and booster rates immediately to protect more of the population against any coming surge.
“We have got to get the United States protected better. We have an abundance of these shots. We have to get them into people,” he said.
Biden administration officials said that whatever the further spread of BA.2 brings to the United States, the next critical step is to provide the $15.6 billion in emergency funding that Congress stripped from a deal to fund the government last week. That money was slated to pay for coronavirus tests, more vaccines and antiviral medications.
“That means that some programs, if we don’t get funding, could abruptly end or need to be pared back, Psaki said at Monday’s briefing. “And that could impact how we are able to respond to any variant.”
In May 2020, a 33-year-old mother of three in North Carolina started experiencing symptoms of COVID-19. Four days later, a different set of symptoms set in. She stopped sleeping well and started having paranoid delusions that people were tracking her through her cell phone—culminating in a frantic scene at a fast-food restaurant, in which she tried to pass her children through the drive-through window, where they’d be safe from the phones and other dangers.
A restaurant employee called 911, and emergency medical services workers arrived, gathered up the family, and hurried to the nearby emergency department of the Duke University Medical Center in Durham, where the mother was quickly attended to by physicians. “She was physically in the room, but she wasn’t making consistent eye contact,” says Dr. Colin Smith, who is now chief resident of the hospital’s internal medicine psychiatry program but was a second-year resident when he took care of the patient. “She was not really engaging all that much. Her thought processes were disorganized.”
Despite that, the patient acknowledged two things to Smith and the other doctors: She knew her behavior was out of character, and the changes all happened quickly after she was diagnosed with COVID-19.
There’s growing evidence that COVID-19 and new psychotic episodes are connected. The North Carolina case, reported in the British Medical Journal in August 2020, joins a slew of case reports published in medical journals during the pandemic that detail psychotic episodes following a COVID-19 diagnosis. In the July 2020 issue of BJPsyh Open, researchers reported that a 55-year old woman in the U.K., with no history of mental illness, arrived at a hospital days after recovering from a severe case of COVID-19 with delusions and hallucinations, convinced that the nurses were devils in disguise and that monkeys were jumping out of the doctors’ medical bags. In April 2021, other researchers wrote in BMJ Case Reports of a middle-aged British man, also with no prior mental health disorders, who had appeared at a London hospital experiencing auditory and visual hallucinations and banging his head against walls until he bruised his skin. (Weeks before, he had recovered from a bout with COVID-19 that had landed him in the intensive care unit.) In yet another case, published in the Journal of Psychiatric Practice in March 2021, a 57-year-old-man turned up at Columbia University’s New York Presbyterian Hospital insisting that his wife was poisoning him, that cameras had been planted throughout his apartment, and that the patients in the hospital’s emergency department were being secretly murdered.
“The situation was strikingly similar to one we’d expect from someone who had a schizophrenia spectrum illness,” says Dr. Aaron Slan, now a fourth-year psychiatry resident at Columbia University, who cared for the patient and co-authored the report. But this patient too had no history of mental health disorders and was too old for a first-onset case of schizophrenia, which typically occurs between ages 20 and 30 for men, Slan notes. What the patient did have, as a test in the hospital revealed, was COVID-19.
COVID-19-related psychotic breaks are rare—though researchers say that it’s too early to say exactly how rare—and plenty of experts believe that the connection between the two conditions, if any, is not causal. In a review published in 2021 in Neurological Letters, a group of researchers in the U.K. casts doubt on the emerging body of work on the COVID-19-psychosis link as “beset by both small sample size, and inadequate attention to potential confounding factors,” such as heightened stress, substance abuse, and socioeconomic hardship.
Still, researchers are investigating the link. One U.K. study published in the Lancet in October 2020 found that of 153 people who were diagnosed with COVID-19 early in the pandemic, 10 suffered new-onset psychotic episodes following their COVID-19 diagnosis, and seven exhibited the onset of psychiatric disorders, including catatonia and mania.
A study published last August in General Hospital Psychiatry took a broad view of the phenomenon, analyzing 40 scientific articles, which included 48 adults from 17 different countries who suffered psychotic episodes associated with COVID-19 infection, and tried to find commonalities among them. As with the Neurological Letters paper, the authors of this study found plenty of other variables that might muddy the link between COVID-19 and psychosis—like stress, substance use, and medications—but the relationship still held.
“We see post-infectious neuroinflammatory disorders associated with a variety of different viral illnesses,” says Dr. Samuel Pleasure, a neurology professor at the University of California, San Francisco (UCSF). “Normally we see it in very small numbers, but here we have [COVID-19] infecting tens of millions of people at the same time.” Even rare cases of psychiatric conditions will start to show themselves when the sample group of infected people is so large.
There are more questions than answers at this point. It’s still unclear whether the severity of COVID-19 symptoms plays any role in the likelihood of a psychotic break. “There seem to be clearly cases of neuropsychiatric consequences of COVID that are linked to cases that are not severe,” Pleasure says. “I believe that the quality of the studies at this point are so preliminary, and the ability to really capture these patients to study is really at early stages, so it’s hard to be definitive.” Similarly, Pleasure says, it’s impossible to say whether people suffering from Long COVID—symptoms that last for months after the infection is over—are more susceptible to psychotic symptoms.
There are multiple possible mechanisms at work, any one of which—or a combination—could be contributing to the neuropsychiatric symptoms associated with COVID-19. The most straightforward would be direct infection of brain tissue itself, according to Pleasure. If that’s so, the number of COVID-19 patients who suffer loss of the sense of taste and smell would suggest that the brain’s olfactory bulb may be struck by the virus first.
“There are documented cases where people have done MRIs early in the [COVID-19 disease] process and have seen some local inflammation in the olfactory bulb,” Pleasure says. “That has contributed further to the idea that maybe that’s the portal of entry.” Once that portal has been breached, the brain at large could be exposed.
Just how the COVID-19 infection reaches the brain is unclear, but Pleasure and his colleague Dr. Michael Wilson, associate professor of neurology at UCSF, conducted lumbar punctures of three teens with COVID-19 who had developed neuropsychiatric symptoms to examine their cerebrospinal fluid. In two cases, they found antibodies in the fluid that target neural antigens. That presented an apparent puzzle: the patients had SARS-CoV-2; if anything, they should be exhibiting antibodies to the virus, not to their own neural tissue. But Pleasure cites one study he conducted with a group from Yale University showing that antibodies specific to the coronavirus spike protein could also cross-react with nerve cells, attacking them as well.
“There was molecular mimicry between the spike protein and a neural antigen,” he says. “One of the main hypotheses is that if there’s an antibody that targets the virus, then, out of bad luck, you also see damage to the host.” In other words, he says, you start with an immune response adaptive to fighting the virus, and that turns into an autoimmune response.
That’s just one theory. There are still other routes by which COVID-19 can affect the brain. Upper respiratory infections can, on occasion, cause the immune system to go awry and develop antibodies against parts of the brain known as NMDA (N-methyl-D-aspartate) receptors, which are the main excitatory receptors that react to neurotransmitters. A broad attack on receptors spread throughout the brain can lead to quick and severe symptoms, says Dr. Mudasir Firdosi, a Consultant Psychiatrist at the Kent and Medway NHS and Social Care Partnership Trust and a co-author of the 2021 BMJ paper.
“[NMDA involvement] presents a very, very florid way to be psychotic,” Firdosi says. Slan agrees: “When someone has an abrupt onset of psychosis following a viral illness, NMDA antibodies are frequently invoked,” he says.
Yet another suspect in the development of neuropsychiatric symptoms is the so-called cytokine storm that often follows infection with SARS-CoV-2. Cytokines are proteins critical for cell signaling that are produced by the immune system and give rise to inflammation that in turn can fight infection. But if cytokine production spins out of control, extreme body-wide inflammation can follow, and brain tissue would not be spared the impact.
“The neurons themselves are not being invaded,” says Slan, “but what happens is that the systemic inflammatory response causes both stress and changes in signaling throughout the body. That includes the brain, and can precipitate these types of [psychotic] symptoms.”
One other bit of evidence that COVID-19 is linked to psychotic breaks comes not from the current scientific literature, but from history. Following the influenza pandemic of 1918 and 1919, there was a spike in what was called encephalitis lethargica, which was essentially a form of early-onset Parkinson’s disease that often didn’t appear for a number of years after the infection—but left patients in what was effectively a state of catatonia.
“That flu virus caused a post-infection inflammation that killed brain cells that in turn led to the Parkinson’s,” says Pleasure. The book and movie Awakenings, about patients who temporarily recovered consciousness and lucidity after treatment with l-dopa—a precursor of the neurotransmitter dopamine—was based on cases of people suffering from that form of Parkinson’s.
The good news is that unlike more chronic forms of psychosis, most cases seemingly related to COVID-19 do not appear to last. The symptoms can respond to antipsychotic medications like Risperdal (risperidone) and Zyprexa (olanzapine), say Smith and Slan. Intravenous immunoglobulin infusions—which reduce the overall load of abnormal cells and inflammatory agents—and steroids, which also reduce inflammation, can be effective as well.
By no means is the case for virus-triggered psychosis closed. Even Slan, who has first-hand experience treating a patient suffering from a seemingly virus-linked psychotic break believes that there is more work to be done—and acknowledges the doubts of the researchers who believe other psychological factors might be at play.
“Given the stress of COVID,” he says, “given the concerns about mortality, seclusion, all of these things represent huge psychosocial stressors, and they have the potential to precipitate oftentimes short-lived psychotic symptoms.”
Of course, even a transitory psychosis is still a psychosis—something no one wants to experience even fleetingly. That puts a premium on avoiding infection in the first place. “The best way to treat COVID-19 and the risk of psychosis is to prevent it,” says Smith. “Even if neurological complications are rare, getting vaccinated remains the smartest choice.”
The website for the group Physicians for Informed Consent (PIC) reads like an apolitical, educational resource that provides information on vaccines and why they shouldn’t be government-mandated. Its mission is “that doctors and the public are able to evaluate the data on infectious diseases and vaccines objectively, and voluntarily engage in informed decision-making about vaccination.”
The group’s accompanying social media accounts, however, tell a different story. On PIC’s Facebook, Twitter, Instagram, and LinkedIn feeds, you’ll find post after post about reasons to be scared of vaccines – especially for children – often highlighting selective portions of scientific research that contain vaccination risks.
Who’s Behind PIC?
The group was founded in 2015 after California passed a law that prohibited the use of personal belief exemptions from vaccinations required for children to attend any public or private school in the state.
Three years later, the number of waivers issued by doctors to parents seeking medical exemptions for their children tripled. As a result, another law was passed in 2019, cracking down on the inappropriate use of medical exemptions.
The group’s founder, Shira Miller, MD, is a concierge integrative medicine doctor based in Los Angeles, specializing in menopausal care. On her own Twitter profile, she describes herself as “Facebook’s Most Popular Menopause Doctor.”
Miller earned her medical degree in 2002 from Technion-Israel Institute of Technology in Haifa, Israel, and has reportedly been working as a concierge physician since 2010.
PIC’s leadership team also includes 20 physicians from a wide range of specialties, most of whom, like Miller, don’t specialize in infectious diseases.
Among its leaders is Paul Thomas, MD, an Oregon-based pediatrician. Thomas, who is listed as one of PIC’s founding directors, was issued an emergency suspension order of his medical license in 2021 by the state medical board, in which they cited at least eight cases of alleged patient harm. In line with PIC’s philosophy, Thomas maintains that he isn’t “anti-vax” – he’s pro-informed-consent.
Also on the team is Jane Orient, MD, internist and executive director of the Association of American Physicians and Surgeons (AAPS), a group that also opposes vaccine mandates. Orient received her medical degree from Columbia University and currently practices in Arizona. In 2020, the AAPS sued the federal government for withholding its stockpile of hydroxychloroquine from COVID patients, despite research showing that the drug is ineffective. The complaint was dismissed in September 2021.
Doug Mackenzie, MD, a plastic surgeon who graduated from Johns Hopkins University of Medicine, is PIC’s treasurer. He has previously identified himself as an “ex-vaxxer” rather than an anti-vaxxer when speaking on a panel in 2019.
The only RN on the team is Tawny Buettner. After California mandated vaccinations for healthcare workers, Buettner organized a protest outside of her place of work, Rady Children’s Hospital in San Diego; she later sued the hospital after she was dismissed from her job. According to the complaint, Buettner and the 36 other plaintiffs alleged that their requests for religious exemptions from the COVID-19 vaccine were all denied.
Kenneth Stoller, MD, also listed on the leadership team, graduated from the American University of the Caribbean School of Medicine and completed pediatric residency training at the University of California Los Angeles. Stoller was disciplined in 2019 for doling out medical exemptions to children without adequate evidence. According to state records, his license in California has since been revoked; he currently holds a medical license in New Mexico.
What’s PIC?
The most notable physician groups accused of spreading COVID-19 misinformation since the vaccine rollout have been affiliated with right-wing media, if not overtly proclaiming conservative, anti-vaccination beliefs.
For example,America’s Frontline Doctors, a group notorious for its support of hydroxychloroquine as a treatment for COVID-19, has made its values well-known. The group’s founder, Simone Gold, MD, JD, was arrested for participating in the Jan. 6 capitol riot and has openly opposed mask-wearing. Similarly, physician leaders of theFront Line COVID-19 Critical Care Alliance, known for promoting the use of ivermectin to treat COVID-19, tout their appearances on the ultra-conservative Newsmax on the website’s homepage.
PIC wants to be different. The group’s focus, according to its general counsel Greg Glaser, JD, of Copperopolis, California, is on the “authoritative citations that show, or calculate, the risks [of vaccines] to the public,” he told MedPage Today.
“We are pro-informed consent, pro-ethics, pro-health. PIC is not anti-vaccine, and PIC is not pro-vaccine – PIC is neutral,” Glaser said on behalf of the group.
In August 2021, Glaser submitted an amicus brief to the Supreme Court PIC’s behalf, arguing against the implementation of vaccine mandates. The document claims that “government statements confirm there is no evidence that COVID-19 vaccines prevent the spread of SARS-CoV-2 or COVID-19,” ignoring the breadth of existing literature that says otherwise.