Douglas MacArthur was one of the finest military leaders the United States ever produced. John Gardner, in his book On Leadership described him as a brilliant strategist, a farsighted administrator, and flamboyant to his fingertips. MacArthur’s discipline and principled leadership transcended the military. He was an effective general, statesman, administrator and corporate leader.
William Addleman Ganoe recalled in his 1962 book, MacArthur Close-up: An Unauthorized Portrait, his service to MacArthur at West Point. During World War II, he created a list of questions with General Jacob Devers, they called The MacArthur Tenets. They reflect the people-management traits he had observed in MacArthur. Widely applicable, he wrote, “I found all those who had no troubles from their charges, from General Sun Tzu in China long ago to George Eastman of Kodak fame, followed the same pattern almost to the letter.”
Do I heckle my subordinates or strengthen and encourage them?
Do I use moral courage in getting rid of subordinates who have proven themselves beyond doubt to be unfit?
Have I done all in my power by encouragement, incentive and spur to salvage the weak and erring?
Do I know by NAME and CHARACTER a maximum number of subordinates for whom I am responsible? Do I know them intimately?
Am I thoroughly familiar with the technique, necessities, objectives and administration of my job?
Do I lose my temper at individuals?
Do I act in such a way as to make my subordinates WANT to follow me?
Do I delegate tasks that should be mine?
Do I arrogate everything to myself and delegate nothing?
Do I develop my subordinates by placing on each one as much responsibility as he can stand?
Am I interested in the personal welfare of each of my subordinates, as if he were a member of my family?
Have I the calmness of voice and manner to inspire confidence, or am I inclined to irascibility and excitability?
Am I a constant example to my subordinates in character, dress, deportment and courtesy?
Am I inclined to be nice to my superiors and mean to my subordinates?
Is my door open to my subordinates?
Do I think more of POSITION than JOB?
Do I correct a subordinate in the presence of others?
BORN in San Gabriel, California, in 1885, George S. Patton, Jr. was the general deemed most dangerous by the German High Command in World War II. Known for his bombastic style, it was mostly done to show confidence in himself and his troops, says author Owen Connelly.
On December 21, 1945, Patton died in Heidelberg, Germany. The following day the New York Times wrote the following editorial:
History has reached out and embraced General George Patton. His place is secure. He will be ranked in the forefront of America’s great military leaders.
Long before the war ended, Patton was a legend. Spectacular, swaggering, pistol-packing, deeply religious, and violently profane, easily moved to anger because he was first of all a fighting man, easily moved to tears because, underneath all his mannered irascibility, he had a kind heart, he was a strange combination of fire and ice. Hot in battle and ruthless, too. He was icy in his inflexibility of purpose. He was no mere hell-for-leather tank commander but a profound and thoughtful military student.
Everyone is to lead in person.
Commanders and staff members are to visit the front daily to observe, not to meddle. Praise is more valuable than blame. Your primary mission as a leader is to see with your own eyes and be seen by your troops while engaged in personal reconnaissance.
Issuing an order is worth only about 10 percent. The remaining 90 percent consists in assuring proper and vigorous execution of the order.
Plans should be simple and flexible. They should be made by the people who are going to execute them.
Information is like eggs. The fresher the better.
Every means must be used before and after combats to tell the troops what they are going to do and what they have done.
Fatigue makes cowards of us all. Men in condition do not tire.
Courage. Do not take counsel of your fears.
A diffident manner will never inspire confidence. A cold reserve cannot beget enthusiasm. There must be an outward and visible sign of the inward and spiritual grace.
Discipline is based on pride in the profession of arms, on meticulous attention to details, and on mutual respect and confidence. Discipline must be a habit so ingrained that it is stronger than the excitement of battle or the fear of death.
A good solution applied with vigor now is better than a perfect solution ten minutes later.
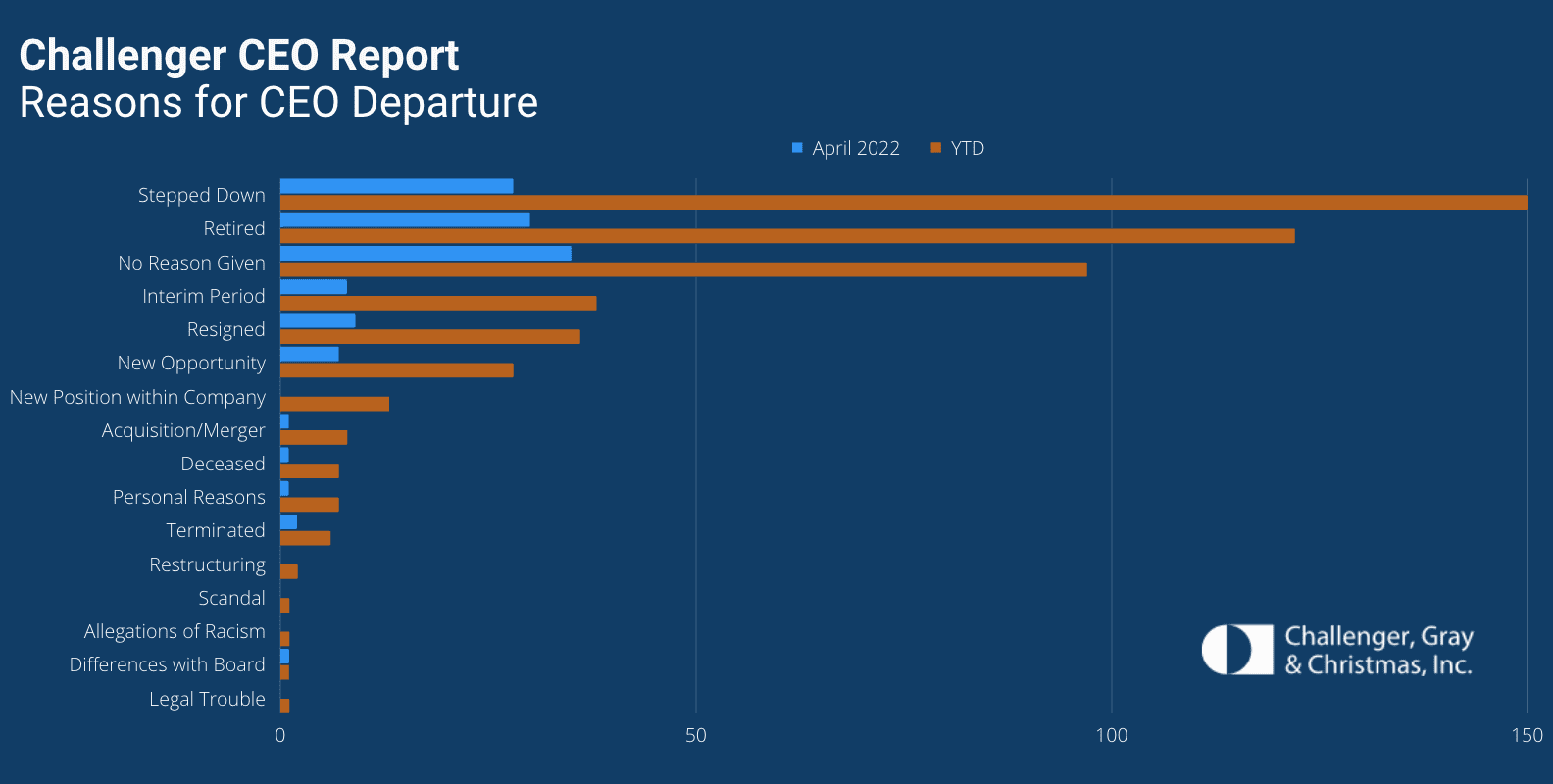
Dozens of hospital CEOs have resigned this year as a record number of chiefs across all industries have exited their roles, according to a May 18 Challenger, Gray & Christmas report.
Nearly 520 CEOs left their posts between Jan. 1 and the end of April, the highest total since the executive outplacement and coaching firm began tracking CEO changes in 2002. The total is up 18 percent from the 440 CEO exits announced in the same period of 2021.
Thirty-six hospital CEOs exited their roles in the first four months of this year. That’s up from the 20 hospital chiefs who resigned in the same period last year, according to the report.
CEOs are leaving their positions and businesses are making changes at the top for several reasons, Challenger, Gray & Christmas Senior Vice President Andrew Challenger said.
“Inflation, staffing shortages, and possible recession concerns are giving more cause for companies to reevaluate leadership,” Mr. Challenger said. “This, after years of companies trying to figure out the right formula to attract and retain talent and create a culture of inclusion, issues that often start at the top.”
A San Jose jury convicted Theranos founder Elizabeth Holmes on four counts of fraud, deciding that she lied to investors while raising more than $700M in funds for the company. Holmes was found not guilty on four other counts relating to defrauding patients, though Theranos ended up voiding tens of thousands of erroneous test results. Each conviction carries a maximum twenty-year sentence, although Holmes is widely expected to appeal.
The Gist: It’s rare that tech executives are convicted of fraud. Investors, including many health systems, have been flooding healthcare startups with large sums of cash in hopes of big returns. But the Theranos debacle is a reminder that Silicon Valley’s “fake it till you make it culture” is not always the best fit for healthcare. Providers must continue to hold new medical technologies to high standards, regardless of how much promise they hold to “revolutionize” aspects of patient care.
We find the questions, “What makes a great leader?” and “What does great leadership mean in practice?” to be really interesting.
We have seen, for example, the following types of people as leaders: (1) people who appear to have been born to lead and excel as leaders, (2) people anointed as leaders or future leaders who had bold personalities, a certain presence and/or great charisma disappoint completely as leaders, (3) hardworking, organized people without bold personalities who organizations may not have expected to be top leaders grow into their roles and lead organizations to great results.
The greatest leaders leave an organization better than they found it. They leave it in a position to thrive long after they are gone. They have the ability to deliver results today while improving and preparing the organization for tomorrow. Great leaders, as stated by some, have a vision and plan, can build great teams, can motivate the team to pursue and achieve the plan, can take in feedback and adjust the plan as needed.
Here are seven thoughts on great leadership.
1. Great leaders are engaged, excited and passionate about success. Great leaders remain excited about what they are doing and what their team is trying to accomplish. Teams sense whether a leader is engaged or not. It does not take long to detect. It is the unusual leader who can stay enthusiastic and in top form in a position for more than 10 to 20 years; for many, the attention span is less. The phrase “lame duck leader” often applies to those who are still in office despite losing their spark. When leaders find they are losing excitement or engagement, it is time to step down from leadership or take time to rediscover themselves. An excited and engaged leader is critical to success.
We should not confuse passion and excitement with a huge or “rah-rah” personality. A great leader can have a winning personality, and most have excellent people skills, but those two things are only part of the picture. Great leaders are more than mascots or faces of a company — they are engaged with their teams. They are constantly talking to, communicating with, seeing and visiting their teams. They know what is going on with their teams, they know what is going on with their key customers, and they know what is going on with the business.
2. Great leaders build teams and the next level of leaders. The greatest accomplishment of a leader may be building the next level of leadership in a way where the leader is less needed. This is so important to the organization and requires tremendous energy from current leadership, yet it’s not always a leader’s first and foremost goal.
An elite team can go exponentially further and accomplish a great deal more than an elite leader. Anyone who has built an organization beyond a few people understands the importance of great teams and colleagues. When a high-performing team is built, the leader remains important. However, more and more, you can identify a great leader or manager by how special their team is. When a team is magnificent, it is a lot easier to be a great leader or manager. A core concept in Jim Collins’ Good to Great is to build great teams and then set plans. If one has great people, a company or team can then accomplish all kinds of things.
There is a common misconception that leaders welcome their team’s elite performance because it means the leader can work less. We find this could not be further from the truth. Great leaders know that nobody likes working harder than their boss. This adage holds true whether a leader has been in the field for five years or 50. The scope and role of the leader may change as the team grows more adept, elite and accomplished. Exceptional leaders give others space to lead, opportunities to shine and chances to succeed, but this should not be misinterpreted as leaders stepping away out of ambivalence or putting their feet up.
3. Great leaders have big goals and set clear plans. Great leaders set goals for their teams and organizations that are exciting, interesting and far bigger than themselves. The leader needs a goal that one can point to as, “This is what we are trying to be,” or, “This is what we are trying to accomplish.” There’s nothing worse than leaders who transparently appear to get ahead for themselves or accomplish their own goals versus the organization’s or team’s goals.
The late Apple CEO and co-founder Steve Jobs and former GE CEO Jack Welch are examples of great leaders who set big goals. Mr. Welch had the core goal to be No. 1 or No. 2 in any market — or not be in the market at all. It is also critical that the goal is well communicated to the team and that key decisions are consistent with the goal. No plan or strategy is perfect. However, most organizations and teams do far better with a plan and strategy than without. Often, the plan is imperfect but adjusted over time. Either way, in nearly every situation, an imperfect plan is far superior to no plan.
4. Great leaders generally don’t micromanage. High-caliber leaders develop great leaders and teams and allow their teams to excel, perform and grow. They constantly look at benchmarks, hold people accountable and follow up with them. However, on a day-to-day and moment-to-moment basis, their teams are given lots of latitude and autonomy. This is coupled with follow-up and looking at what is accomplished. Warren Buffett may be the world’s best example of a leader who has great CEOs, holds them accountable and doesn’t micromanage them.
Some of the best leaders we have seen recognize when they have an amazing leader working with them. In those situations, the best of leaders can set their egos aside and largely allow the next in line to take credit and lead.
5. Great leaders praise often and recognize contributions. A great leader understands that part of team-building is constantly looking for what people are doing well and encouraging more of it. Great leaders provide praise, recognize what is done well and motivate more of that to be done. They look for what people do exceptionally well, and they look to promote those doing great things. They are constantly looking for the next opportunity for people.
6. Great leaders are not afraid to make hard personnel decisions. The best leaders understand that not everyone is a fit for every job. They are not willing to tolerate mediocrity or toxicity. This doesn’t mean they have a quick trigger. It does mean that they constantly compare current performance to great performance and try to fit people in spots where their performance can excel. For example, someone who is not great at something might be given another try at a different role where they may shine. One of the best leaders I ever witnessed subscribed to the view that it was very hard to change people. He counseled to be fair and patient, but that it was easier to change the person than change a person. In essence, sometimes it’s easier to replace a person than change how a person behaves.
7. Great leaders are emotionally mature. Great leaders do not fly off the handle or make rash decisions, but they do follow their instincts. A remarkable leader does not react to every issue with a great deal of stress. Rather, he or she can take things in, move forward and keep a team on board. A leader’s ability to manage emotions — both his or her own and those of team members — is critical. While great leaders often act with urgency and intent, they too embrace common sense approaches of “sleep on it” or “no sudden movements” when faced with volatility, uncertainty, complexity and ambiguity. They recognize the repercussions of their decisions and movements, and in turn give them the time, thought and reflection they deserve.
The healthcare industry’s staffing shortage crisis has had clear consequences for care delivery and efficiency, forcing some health systems to pause nonemergency surgeries or temporarily close facilities. Less understood is how these shortages are affecting care quality and patient safety.
A mix of high COVID-19 patient volume and staff departures amid the pandemic has put hospitals at the heart of a national staffing shortage, but there is little national data available to quantify the shortages’ effects on patient care.
The first hint came last month from a CDC report that found healthcare-associated infections increased significantly in 2020 after years of steady decline. Researchers attributed the increase to challenges related to the pandemic, including staffing shortages and high patient volumes, which limited hospitals’ ability to follow standard infection control practices.
“That’s probably one of the first real pieces of data — from a large scale dataset — that we’ve seen that gives us some sense of direction of where we’ve been headed with the impact of patient outcomes as a result of the pandemic,” Patricia McGaffigan, RN, vice president of safety programs for the Institute for Healthcare Improvement, told Becker’s. “I think we’re still trying to absorb much of what’s really happening with the impact on patients and families.”
An opaque view into national safety trends
Because of lags in data reporting and analysis, the healthcare industry lacks clear insights into the pandemic’s effect on national safety trends.
National data on safety and quality — such as surveys of patient safety culture from the Agency for Healthcare Research and Quality — can often lag by several quarters to a year, according to Ms. McGaffigan.
“There [have been] some declines in some of those scores more recently, but it does take a little while to be able to capture those changes and be able to put those changes in perspective,” she said. “One number higher or lower doesn’t necessarily indicate a trend, but it is worth really evaluating really closely.”
For example, 569 sentinel events were reported to the Joint Commission in the first six months of 2021, compared to 437 for the first six months of 2020. However, meaningful conclusions about the events’ frequency and long-term trends cannot be drawn from the dataset, as fewer than 2 percent of all sentinel events are reported to the Joint Commission, the organization estimates.
“We may never have as much data as we want,” said Leah Binder, president and CEO of the Leapfrog Group. She said a main area of concern is CMS withholding certain data amid the pandemic. Previously, the agency has suppressed data for individual hospitals during local crises, but never on such a wide scale, according to Ms. Binder.
CMS collects and publishes quality data for more than 4,000 hospitals nationwide. The data is refreshed quarterly, with the next update scheduled for October. This update will include additional data for the fourth quarter of 2020.
“It is important to note that CMS provided a blanket extraordinary circumstances exception for Q1 and Q2 2020 data due to the COVID-19 pandemic where data was not required nor reported,” a CMS spokesperson told Becker’s. “In addition, some current hospital data will not be publicly available until about July 2022, while other data will not be available until January 2023 due to data exceptions, different measure reporting periods and the way in which CMS posts data.”
Hospitals that closely monitor their own datasets in more near-term windows may have a better grasp of patient safety trends at a local level. However, their ability to monitor, analyze and interpret that data largely depends on the resources available, Ms. McGaffigan said. The pandemic may have sidelined some of that work for hospitals, as clinical or safety leaders had to shift their priorities and day-to-day activities.
“There are many other things besides COVID-19 that can harm patients,” Ms. Binder told Becker’s. “Health systems know this well, but given the pandemic, have taken their attention off these issues. Infection control and quality issues are not attended to at the level of seriousness we need them to be.”
What health systems should keep an eye on
While the industry is still waiting for definitive answers on how staffing shortages have affected patient safety, Ms. Binder and Ms. McGaffigan highlighted a few areas of concern they are watching closely.
The first is the effect limited visitation policies have had on families — and more than just the emotional toll. Family members and caregivers are a critical player missing in healthcare safety, according to Ms. Binder.
When hospitals don’t allow visitors, loved ones aren’t able to contribute to care, such as ensuring proper medication administration or communication. Many nurses have said they previously relied a lot on family support and vigilance. The lack of extra monitoring may contribute to the increasing stress healthcare providers are facing and open the door for more medical errors.
Which leads Ms. Binder to her second concern — a culture that doesn’t always respect and prioritize nurses. The pandemic has underscored how vital nurses are, as they are present at every step of the care journey, she continued.
To promote optimal care, hospitals “need a vibrant, engaged and safe nurse workforce,” Ms. Binder said. “We don’t have that. We don’t have a culture that respects nurses.”
Diagnostic accuracy is another important area to watch, Ms. McGaffigan said. Diagnostic errors — such as missed or delayed diagnoses, or diagnoses that are not effectively communicated to the patient — were already one of the most sizable care quality challenges hospitals were facing prior to the pandemic.
“It’s a little bit hard to play out what that crystal ball is going to show, but it is in particular an area that I think would be very, very important to watch,” she said.
Another area to monitor closely is delayed care and its potential consequences for patient outcomes, according to Ms. McGaffigan. Many Americans haven’t kept up with preventive care or have had delays in accessing care. Such delays could not only worsen patients’ health conditions, but also disengage them and prevent them from seeking care when it is available.
Reinvigorating safety work: Where to start
Ms. McGaffigan suggests healthcare organizations looking to reinvigorate their safety work go back to the basics. Leaders should ensure they have a clear understanding of what their organization’s baseline safety metrics are and how their safety reports have been trending over the past year and a half.
“Look at the foundational aspects of what makes care safe and high-quality,” she said. “Those are very much linked to a lot of the systems, behaviors and practices that need to be prioritized by leaders and effectively translated within and across organizations and care teams.”
She recommended healthcare organizations take a total systems approach to their safety work, by focusing on the following four, interconnected pillars:
Culture, leadership and governance
Patient and family engagement
Learning systems
Workforce safety
For example, evidence shows workforce safety is an integral part of patient safety, but it’s not an area that’s systematically measured or evaluated, according to Ms. McGaffigan. Leaders should be aware of this connection and consider whether their patient safety reporting systems address workforce safety concerns or, instead, add on extra work and stress for their staff.
Safety performance can slip when team members get busy or burdensome work is added to their plates, according to Ms. McGaffigan. She said leaders should be able to identify and prioritize the essential value-added work that must go on at an organization to ensure patients and families will have safe passage through the healthcare system and that care teams are able to operate in the safest and healthiest work environments.
In short, leaders should ask themselves: “What is the burdensome work people are being asked to absorb and what are the essential elements that are associated with safety that you want and need people to be able to stay on top of,” she said.
To improve both staffing shortages and quality of care, health systems must bring nurses higher up in leadership and into C-suite roles, Ms. Binder said. Giving nurses more authority in hospital decisions will make everything safer. Seattle-based Virginia Mason Hospital recently redesigned its operations around nurse priorities and subsequently saw its quality and safety scores go up, according to Ms. Binder.
“If it’s a good place for a nurse to go, it’s a good place for a patient to go,” Ms. Binder said, noting that the national nursing shortage isn’t just a numbers game; it requires a large culture shift.
Hospitals need to double down on quality improvement efforts, Ms. Binder said. “Many have done the opposite, for good reason, because they are so focused on COVID-19. Because of that, quality improvement efforts have been reduced.”
Ms. Binder urged hospitals not to cut quality improvement staff, noting that this is an extraordinarily dangerous time for patients, and hospitals need all the help they can get monitoring safety. Hospitals shouldn’t start to believe the notion that somehow withdrawing focus on quality will save money or effort.
“It’s important that the American public knows that we are fighting for healthcare quality and safety — and we have to fight for it, we all do,” Ms. Binder concluded. “We all have to be vigilant.”
Conclusion
The true consequences of healthcare’s labor shortage on patient safety and care quality will become clear once more national data is available. If the CDC’s report on rising HAI rates is any harbinger of what’s to come, it’s clear that health systems must place renewed focus and energy on safety work — even during something as unprecedented as a pandemic.
The irony isn’t lost on Ms. Binder: Amid a crisis driven by infectious disease, U.S. hospitals are seeing higher rates of other infections.
“A patient dies once,” she concluded. “They can die from COVID-19 or C. diff. It isn’t enough to prevent one.”