California hospitals are providing significantly less free and discounted care to low-income patients since the Affordable Care Act took effect.
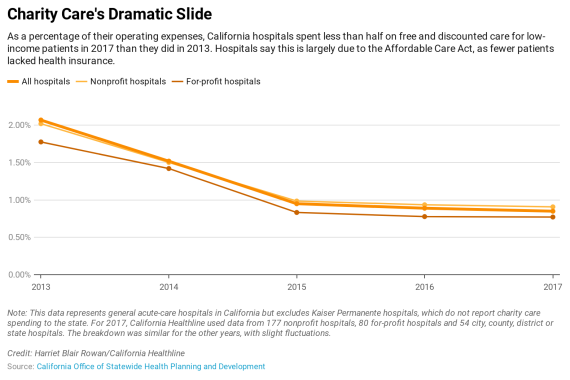
As a proportion of their operating expenses, the state’s general acute-care hospitals spent less than half on these patients in 2017 than they did in 2013, according to data the hospitals reported to California’s Office of Statewide Health Planning and Development.
The biggest decline in charity care spending occurred from 2013 to 2015, when it dropped from just over 2% to just under 1%. The spending has continued to decline, though less dramatically, since then.
The decline was true of for-profit hospitals, so-called nonprofit hospitals and those designated as city, county, district or state hospitals.
Health experts attribute the drop in charity care spending largely to the implementation of the federal Affordable Care Act, popularly known as Obamacare. The law expanded insurance coverage to millions of Californians, starting in 2014, and hospitals are now treating far fewer uninsured patients who cannot pay for the care they receive.
With fewer uninsured patients, fewer patients seek financial assistance through the charity care programs, according to the California Hospital Association.
Cori Racela, deputy director at the Western Center on Law & Poverty, countered that many people still need financial assistance because — even with insurance — they struggle to pay their premiums, copays and deductibles.
“The need for charity care has changed,” she said, “but it still exists.”
The data on charity care comes from most of the state’s general acute-care hospitals but does not include Kaiser Permanente hospitals, which are not required by the state to report their charity care totals. (Kaiser Health News, which produces California Healthline, has no affiliation with Kaiser Permanente.)
For 2017, California Healthline used data from 177 nonprofit hospitals, 80 for-profit hospitals and 54 city, county, district or state hospitals. The breakdown was similar for the other years, with slight fluctuations.
Nonprofit hospitals, whose charity care spending dropped from 2.02% of operating expenses to 0.91% over the five-year period, are required by state and federal law to provide “community benefits” in exchange for their tax-exempt status.
They can meet that requirement beyond providing free and discounted care in a variety of ways: They can offer community public health programs, write off uncollected patient debt and claim the difference between what it costs to provide care and the amount that they are reimbursed by government insurance programs.
Nonprofit “hospitals get tax-exempt status, but they don’t get it for free,” said Ge Bai, associate professor of accounting and health policy at Johns Hopkins University. Charity care “is part of the implicit contract between hospital and taxpayers.”
Bai sees the reduced spending on charity care as part of a trend of nonprofit hospitals acting more like their for-profit counterparts.
Many nonprofit hospitals “no longer consider charity care their primary mission,” she said. “They are making more and more money but they are dropping their charity care.”
The state and federal governments set no minimum requirements for charity spending by hospitals, although the California Attorney General has created standards for a few nonprofit hospitals that have changed ownership in recent years.
Jan Emerson-Shea, a spokeswoman for the California Hospital Association, said hospitals are giving back to their communities in ways beyond charity care.
“You see charity care declining, but Medi-Cal losses are increasing,” Emerson-Shea said. She pointed to the growing shortfalls many hospitals report from caring for more patients covered by the public insurance program. “Every Medi-Cal patient we treat we lose money on.”
Medi-Cal, the state’s Medicaid program for low-income residents, increased its rolls by 5.6 million — or about 70% — from 2013 to 2017.
Racela, of the Western Center on Law & Poverty, would like to see changes in California’s charity care rules to address high out-of-pocket costs.
And she wants hospitals to abide by the state law that requires them to inform patients that they may be eligible for charity care based on their income.
“There is still a big unmet need for charity care across the state,” Racela said.