One year after the World Health Organization declared COVID-19 a pandemic, the end of that pandemic is within reach.
The big picture: The death and suffering caused by the coronavirus have been much worse than many people expected a year ago — but the vaccines have been much better.
Flashback: “Bottom line, it’s going to get worse,” Anthony Fauci told a congressional panel on March 11, 2020, the day the WHO formally declared COVID-19 to be a global pandemic.
- A year ago today, the U.S. had confirmed 1,000 coronavirus infections. Now we’re approaching 30 million.
- In the earliest days of the pandemic, Americans were terrified by the White House’s projections — informed by well-respected modeling — that 100,000 to 240,000 Americans could die from the virus. That actual number now sits at just under 530,000.
- Many models at the time thought the virus would peak last May. It was nowhere close to its height by then. The deadliest month of the pandemic was January.
Yes, but: Last March, even the sunniest optimists didn’t expect the U.S. to have a vaccine by now.
- They certainly didn’t anticipate that over 300 million shots would already be in arms worldwide, and they didn’t think the eventual vaccines, whenever they arrived, would be anywhere near as effective as these shots turned out to be.
Where it stands: President Biden has said every American adult who wants a vaccine will be able to get one by the end of May, and the country is on track to meet that target.
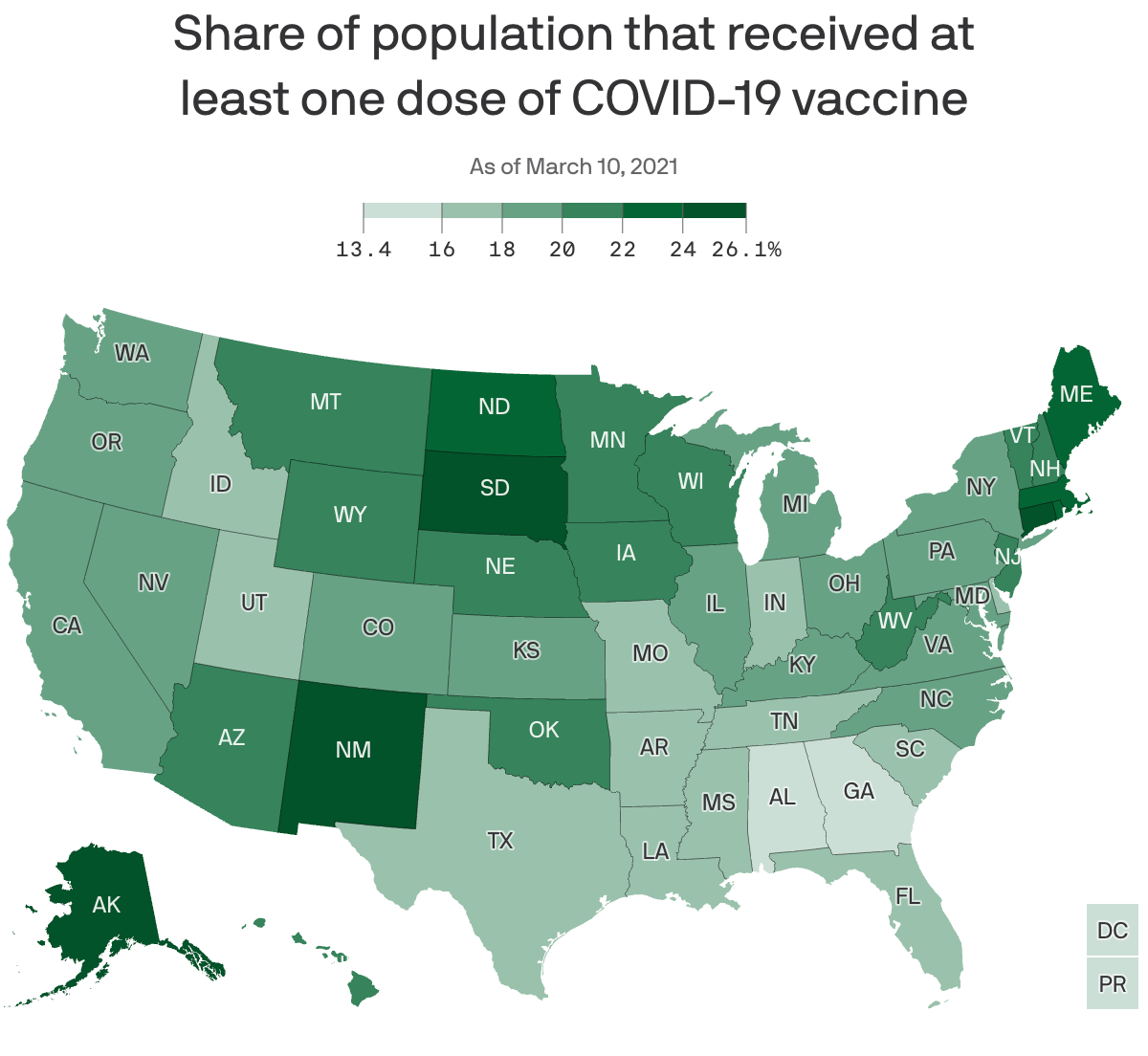
- The U.S. is administering over 2 million shots per day, on average. Roughly 25% of the adult population has gotten at least one shot.
- The federal government has purchased more doses than this country will be able to use: 300 million from Pfizer, 300 million from Moderna and 200 million from Johnson & Johnson.
- The Pfizer and Moderna orders alone would be more than enough to fully vaccinate every American adult. (The vaccines aren’t yet authorized for use in children.)
Yes, millions of Americans are still anxiously awaiting their first shot — and navigating signup websites that are often frustrating and awful.
- But the supply of available vaccines is expected to surge this month, and the companies say the bulk of those doses should be available by the end of May.
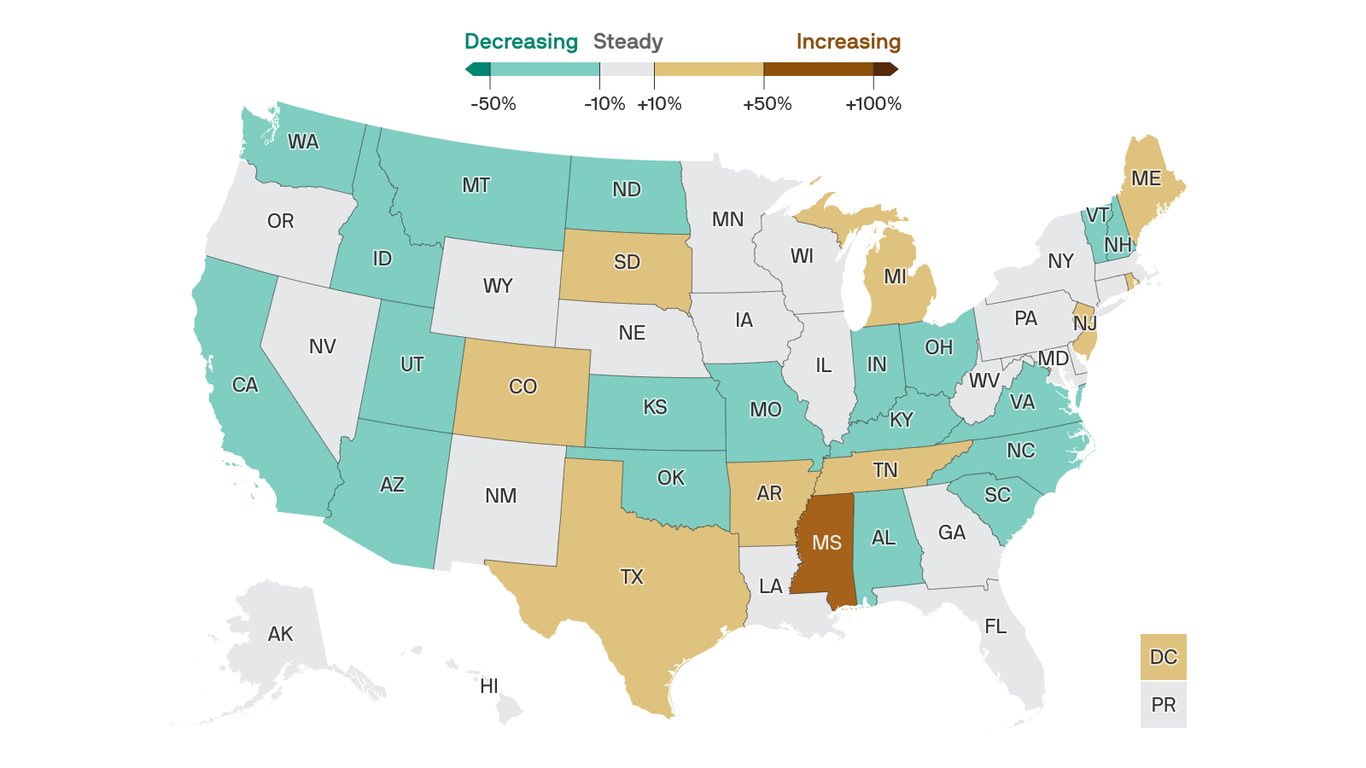
- Cases, hospitalizations and deaths are all falling sharply at the same time vaccinations are ramping up.
The bottom line: Measured in death, loss, isolation and financial ruin, one year has felt like an eternity. Measured as the time between the declaration of a pandemic and vaccinating 60 million Americans, one year is an instant.
- The virus hasn’t been defeated, and may never fully go away. Getting back to “normal” will be a moving target. Nothing’s over yet. But the end of the worst of it — the long, brutal nightmare of death and suffering — is getting close.