Health officials are grappling with how to prevent potential COVID-19 outbreaks from the delta variant that is spreading rapidly across the U.S.
Concern over the highly transmissible delta strain prompted Los Angeles County this week to recommend that all people wear masks indoors, even if they’re vaccinated. The World Health Organization (WHO) has also encouraged fully vaccinated people to continue using masks.
But the Centers for Disease Control and Prevention (CDC) has not signaled any plans to revise its mask guidance, with Biden administration officials and some experts say that fully vaccinated Americans are safe from all existing COVID-19 variants.
“If you have been vaccinated, the message we’re conveying is you’re safe,” White House press secretary Jen Psaki said Wednesday. “Vaccines are effective, and that is something we want to be very clear with the public about.”
Still, the move by officials in Los Angeles County raises the prospect that mask recommendations and even mandates could make a return to certain parts of the country.
The CDC projected the delta variant made up more than a quarter of cases in the U.S. in the most recent two-week period, ending June 19 — a jump from 10 percent the previous two weeks.
Los Angeles County issued a statement Monday saying it “strongly recommends” all people wear masks in indoor settings where they don’t know everyone’s vaccination status.
Barbara Ferrer, director of the county’s Department of Public Health, told The Hill that officials want to take time to get more people vaccinated as research is conducted on delta variant transmission from the fully vaccinated.
“While we’re doing that work with building confidence, we’re going to go ahead and offer as much protection as possible for everyone,” she said.
Leana Wen, an emergency physician and public health professor at George Washington University, praised the county’s decision as the “right move,” saying she hopes other jurisdictions follow suit to protect both vaccinated and unvaccinated residents.
“People who are fully vaccinated are still at risk, albeit a low risk, from those who are unvaccinated,” Wen said.
“Fully vaccinated people can be around others who are fully vaccinated without any limitations,” she added. “However, if they’re going to be around unvaccinated people or vaccination status is not being checked, then those could be high-risk settings” where masks should be worn.
For now, Los Angeles County is an outlier as cities and states continue to loosen mask requirements. Washington’s King County, home to Seattle, and Pennsylvania were the latest jurisdictions to end their mandates, taking that step this week.
CDC Director Rochelle Walensky told NBC’s “Today” on Wednesday that the agency’s guidance that fully vaccinated people don’t need masks in most settings has not changed. She said the WHO has given conflicting instructions, saying the international organization is focused on the global community, which has a lower vaccination rate than the U.S.
“We have always said that local policymakers need to make policies for their local environment,” Walensky said. “But those masking policies are not to protect the vaccinated, they’re to protect the unvaccinated.”
So far, the delta strain has not led to any changes in masking policies at the White House or the Capitol.
The White House does not require masks if a person is vaccinated, although the administration is not checking to see whether all maskless people have gotten their COVID-19 shots.
In recent weeks, the House has ended its universal mask requirement, and few people in the Capitol continue to wear them. The overwhelming majority of lawmakers in both parties have shed masks and freely gather in large groups on the House floor.
The Senate, which never had a mask requirement since nearly all senators voluntarily wore facial coverings when it was recommended, has also relaxed its pandemic restrictions.
But the delta variant threat is influencing other activities in the House. Speaker Nancy Pelosi (D-Calif.) announced this week that proxy voting would be extended through Aug. 17, and House Majority Leader Steny Hoyer (D-Md.) said that was due to the global spread of the delta variant.
“As we know, there are some countries in the world that are seeing a virulent resurgence of this new variant of the COVID-19. Israel is a perfect example of that,” Hoyer told reporters, referring to Israel reimposing its indoor mask mandate despite having one of the world’s highest vaccination rates. “But even in Israel, where they have the vaccine available, they’re seeing a resurgence.”
“So, the Speaker correctly, along with the medical advice that she’s gotten, determined that there was still justification for staying on guard,” Hoyer said.
Recent studies have found that COVID-19 vaccines are effective against the strain. Both doses of Pfizer-BioNTech were found to be 88 percent effective against symptomatic disease.
There is “less data” on how Johnson & Johnson performs, Walensky said Wednesday, but “right now we have no information to suggest that you need a second shot after J&J, even with the delta variant.”
Jen Kates, senior vice president and director of global health & HIV policy at the Kaiser Family Foundation, said research shows the CDC guidance “still stands,” although she acknowledged the agency needs to be prepared to adjust.
Kates expressed concern that the resurgence of the mask debate could affect the vaccination effort, noting the variant is spreading mostly among unvaccinated people.
“The worst outcome, I think, is that people choose not to get vaccinated because they think the vaccines aren’t as effective against variants,” she said.
As most Americans have gotten vaccinated, COVID-19 cases, hospitalizations and deaths have declined significantly. But the U.S. is expected to fall short of President Biden’s goal to have 70 percent of adults receiving at least one vaccine dose by the Fourth of July.
The White House still plans to move forward with Independence Day festivities. The administration sent 1,000 invitations for people to gather at 1600 Pennsylvania Ave. on Sunday, with vaccinated people allowed to go without masks. All guests were instructed to get tested one to three days before arriving.
“We certainly feel comfortable and confident moving forward with our event here at the White House and individuals having barbecues in their backgrounds this week to celebrate the Fourth of July,” Psaki said on Wednesday.
It’s “a trickle that will become a torrent,” Ashish Jha, dean at Brown University’s School of Public Health, tweeted.
More hospitals are likely to require employees receive a COVID-19 vaccine, experts said, to further protect the sick and vulnerable patients who rely on them for care.
A Houston-area hospital captured headlines after taking a firm stance on requiring vaccines that prevent severe illness of the coronavirus, which has killed more than 600,000 in the U.S. and ravaged the economy.
Houston Methodist employees who refused the vaccine were either terminated or resigned. A judge earlier this month sided with the hospital and tossed out an employee lawsuit that was seeking to block the mandated inoculation. The ruling may give other hospitals the green light to require the jab, and as more facilities put a similar policy in place, others are likely to follow, experts said.
It’s “a trickle that will become a torrent,” Ashish Jha, professor and dean at Brown University’s School of Public Health, posted Thursday on Twitter.
3 large health systems in Massachusetts to require all workers to be vaccinated.
Given the critical need to protect vulnerable patients, its critical all hospitals do this.
Some of the nation’s largest health systems have yet to mandate the shot, including Kaiser Permanente and CommonSpirit Health.
“Vaccination will only be required for Kaiser Permanente employees if a state or county where we operate mandates the vaccine for health care workers,” the company said in an email.
The American Hospital Association continues to hear that a growing number of its members are requiring the vaccine, with some exemptions. However, many member hospitals are waiting until the FDA grants full approval, a time when more safety and efficacy data will be made available.
“Getting vaccinated is especially critical for health care professionals because they work with patients with underlying health conditions whose immune systems may be compromised,”AHA, which has not taken on stance on the requirement, said in a statement.
The mandates raise ethical questions, some say, pointing to the profession’s promise to “do no harm.”
Arthur Caplan, head of medical ethics at New York University School of Medicine, said the codes of ethics that doctors and nurses says to put patients first, do no harm and protect the vulnerable.
“Of course they should be vaccinated,” he said. “If they don’t want to get vaccinated, I think they’re in the wrong profession.”
The Equal Employment Opportunity Commission said employment law does not prohibit employers from requiring the jab, essentially giving the green light to employers to put incentives and requirements in place for their workers. The EEOC is the federal agency tasked with ensuring that workplaces do not discriminate.
Some states are going against the tide and signing legislation that bars vaccine mandates, including Florida. The city of San Francisco will require hospital employees and workers in high-risk settings to get the vaccine. San Francisco, like other employers and universities, will require all city workers get inoculated.
The differing policy stances across the country creates additional hurdles for corporations with a large footprint.
As the delta variant of the coronavirus spreads, especially among the unvaccinated, the Biden administration is gearing up for a new push to vaccinate the so-called “movable middle”—and some public health experts say FDA could advance that goal by fully approving Covid-19 vaccines.
Analysis reveals toll of US Covid-19 deaths among unvaccinated patients
According to an analysis by the Associated Press, nearly all recent Covid-19 deaths have occurred in unvaccinated individuals.
The AP analysis is based on data from CDC, although CDC has not itself released estimates of the share of Covid-19 deaths among unvaccinated patients.
According to the AP analysis, just 0.8% of Covid-19 deaths in May were among the fully vaccinated. Meanwhile, the share of hospitalized patients who were fully vaccinated was just 0.1% in May, with fewer than 1,200 fully vaccinated people hospitalized out of more than 853,000 hospitalizations.
Meanwhile, according to CDC, 54% of the U.S. population, including 66% of American adults, have received at least one dose of a Covid-19 vaccine, while 46.1% of the total population and 56.8% of American adults have received all required doses.
In many places across the United States, COVID-19 feels over. Unmasked citizens run rampant. New York City is planning an August mega-concert in Central Park. I’m as hopeful as the rest of us, but I think we may be suffering from memory loss.
Let’s start from this time last year, when many Americans were exuberantly returning to newly reopened beaches, parks and restaurants after a seemingly eternal three months—three whole months!—of quarantine. Universal observance of safety guidelines was surely going to be sufficient to limit viral spread.
We know how that turned out. By mid-June 2020, there were already signs that our bleary-eyed re-emergence was premature. On June 22, 2020, the number of new daily cases of COVID-19 (33,485) surpassed the high-water mark hit on the worst day of the horrific first surge, when that figure peaked at just over 32,000.
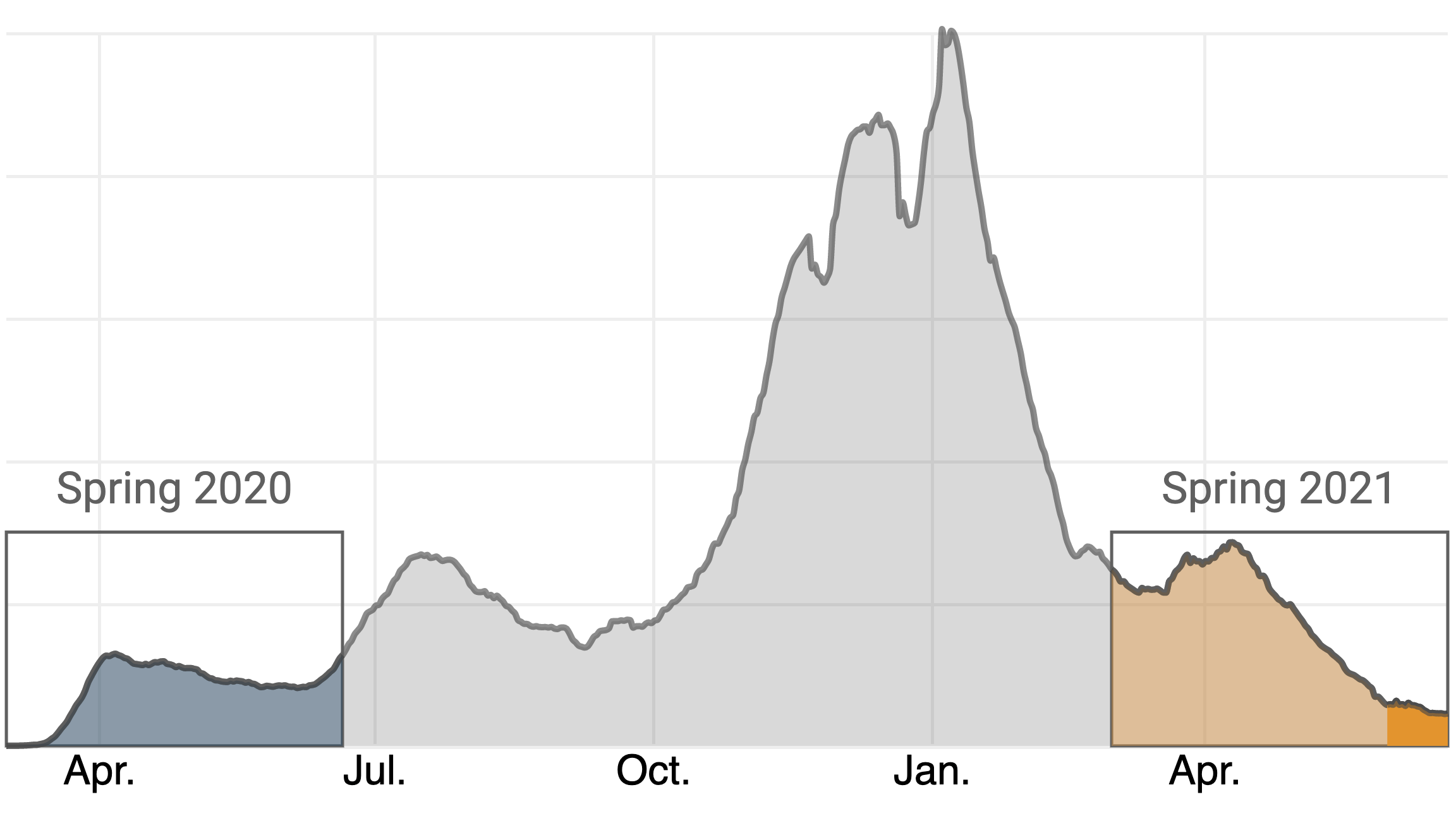
A year later, the daily case count is not as foreboding—nor is it nearly as low it may appear.
You’ll notice that this graph covers only the past 12 weeks, while virtually every chart you’ll find (including the one on TIME’s dashboard) graphs COVID-19 cases from the beginning of the outbreak. This is intentional. The toll of the pandemic in the U.S. has persisted for so long, and reached such catastrophic heights in the first weeks of 2021, that patterns such as this one are nearly impossible to see on the typical chart. Here’s what the same graph looks like against that backdrop:
My fear is that the pandemic remains much more deadly than how it looks on the page. Yes, deaths remain on a steady decline, having recently sunk below 300 people a day on average for the first time since March 24, 2020, right around the time that many offices were shuttering. But a surge in cases, particularly among the large number of unvaccinated Americans, could quickly reverse that decline.
As you can see, it has been less than a month since the 2021 case count sunk below the year-over-year figure, on May 26. The massive nationwide vaccine rollout is undoubtedly a major factor, but it’s difficult to quantify the impact of vaccination on the currently low case and death figures. There are only weak correlations between states’ vaccination rates and some key indicators, like the rate at which cases have risen or fallen in recent weeks.
What we can quantify is that, in the 27 days since the lines crossed, the vaccination rate in the U.S. has only crawled upward, from 39.7% to 45.3% of Americans who have received a complete dosage. While the official vaccination rate applies to the entire population, data from the U.S. Centers for Disease Control and Prevention (CDC) also includes percentages for several age groups. By TIME’s calculations, there are 97.4 million adults age 18 and over who have been eligible for vaccination for two months but who have not yet received even a first dose. This group trends heavily younger, with those 65 and over representing only 7.8% of the unvaccinated population. (These figures do no include those under 18, who constitute a small portion of the eligible population.)
On May 13, two weeks before daily case numbers in 2021 fell below the year-over-year figures from the same day in 2020, the CDC issued guidance liberating fully vaccinated individuals from wearing masks in many scenarios. I do not have conclusive proof that any of the country’s 97.4 million unvaccinated adults have abused this privilege. All I can state with confidence is that, based on the number of people I’ve seen not wearing a mask in places like stores, which often have signs imploring those who are not fully vaccinated to continue to mask up, it is mathematically almost certain that more than a few have done so.
Which is to say: the situation today, if one can momentarily rewind to Memorial Day of 2020, feels very familiar. There appears to be a lambent light at the end of the tunnel, yet cavalier attitudes towards the pandemic, particularly among younger people who, as a group, are under-vaccinated, resembles what we saw last summer just before the second wave.
Watching these trends, I grow more concerned every day that the country is positioned for yet another surge in cases, despite our defensive upgrades in the off-season. I hope I’m wrong, but the numbers are not nearly as comforting as they first look. The fact that the Delta variant, which is both more transmissible and appears to cause more severe disease, is on pace to become the dominant form of COVID-19 in the U.S. in the coming months is further reason for alarm. Moreover, some states have significantly higher vaccination rates than others, leaving those with less protection more vulnerable to future spikes.
Forgive me for being a buzzkill, but unless we can institute a functional vaccine passport system, which appears unlikely, I do not think it is wise to assume that every unmasked individual is fully dosed. Short of a passport system, and with dangerous variants competing for dominance and the duration of vaccine protection still unclear, we ought to continue to ration physical space in public areas—a policy that is hastily being relaxed at places like Major League Baseball parks. I love baseball and eagerly look forward to buzzing up to Philadelphia to take in a game at Citizen’s Bank Park, which is operating at full capacity. But not while the policy is that “Unvaccinated fans are strongly encouraged to wear their masks in all indoor and outdoor areas in and around the ballpark.”
I also think there might be a backdoor to a digital passport system. Based on polling data, it appears there is a substantial population of people who aren’t categorically opposed to vaccination, just unmotivated to get around to it—what we’ve termedvaccine “meh-sitance,” not hesitance. My proposal is that bars, restaurants and other popular venues merely require each person who enters to verbally affirm that they are fully vaccinated.
This might sound about as effective as asking passengers in the exit row to individually verify that they listened to the instructions. But while it’s one thing to ignore a sign at the grocery store, it’s another to lie in front of your friends. Peer pressure is a powerful motivator, and if even a fraction of the unvaccinated would take the time to resolve that dissonance, or risk missing out on trivia night, it could substantially push up the percentages. I call this the “FOMO method,” and though we are still a long, long way from eliminating the disease altogether, it could help us avert a fourth wave this summer.
The country is reopening. What does the future hold?
The story of the American pandemic has unfolded in three chapters.The first began last January, when the coronavirus emerged and the world was plunged into uncertainty about how covid-19 could be treated, how the virus spread, and when it might be defeated. The second started on the morning of November 9, 2020, when Pfizer-BioNTech announced the extraordinary efficacy of its vaccine. Those results made clear that this pandemic would end not through infection but vaccination. Our goals shifted from merely slowing the spread to beginning immunization as quickly as possible. In America, much of the past half year has been devoted to administering vaccines and gathering evidence on how well they work in the real world.
Earlier this month, the Centers for Disease Control and Prevention ushered in the American pandemic’s third chapter. The agency announced that vaccinated people could go without masks or social distancing indoors and outside, in crowds large and small. It carved out a few exceptions—for hospitals, public transportation, and the like—and noted that people still needed to obey federal and local laws. But the broad message was that vaccinated Americans could resume their pre-pandemic lives. The C.D.C. is an agency known for caution, and its new guidance shocked many public-health experts; just two weeks earlier, it had issued far more restrictive recommendations. During the same period, a survey of nearly six hundred epidemiologists found that more than three-quarters of them believed that indoor mask-wearing might remain necessary for another year or more. Still, immediately after the announcement, a number of states lifted their mask mandates. Others will surely follow, as the pressure to return to normal grows. America is now moving swiftly toward reopening.
Despite the C.D.C.’s early stumbles on communication, masks, and tests, it remains perhaps the world’s preëminent public-health agency. Its recommendations carry unparalleled scientific force in the U.S. and beyond. Ultimately, the C.D.C.’s decision reflects real shifts in the weight of the evidence on several fundamental epidemiological questions: Are the vaccines as effective as they were in the trials? Can they protect us against the coronavirus variants? And do they prevent not just illness but transmission? The answers to these questions give us good reason to think that the pandemic’s newest chapter will be its last. Read The New Yorker’s complete news coverage and analysis of the coronavirus pandemic.
On the first question, the nationwide rollout of covid-19 vaccines has proved, beyond any doubt, that they are astonishingly effective at preventing serious illness, even for the most vulnerable people. So-called breakthrough infections, in which the virus weaves its way around some of an individual’s immune system, do occur. But such infections are extremely rare, and—because a person almost always has some effective antibodies and other immune-system defenses—they usually cause mild or no symptoms. In one study, the C.D.C. examined post-vaccination infections among nearly fifteen thousand nursing-home residents and staff members, and discovered only two covid-19 hospitalizations and one death. Another study, involving half a million health-care workers from around the country, found that getting two shots reduced the risk of a symptomatic infection by ninety-four per cent. Moving forward, we should expect to continue seeing breakthrough infections from time to time—but, for the most part, we shouldn’t worry about them. (At the same time, the covid vaccines have proved exceptionally safe. Few dangerous side effects have been linked to the vaccines from Pfizer-BioNTech or Moderna, and the over-all risk of concerning blood clots after receiving Johnson & Johnson’s vaccine is rare—as of last week, when more than nine million doses had been administered, there were thirty confirmed cases.)
The most striking vaccine-efficacy statistic draws on data shared by state governments. Around a hundred and thirty million Americans are fully vaccinated, and the C.D.C. has said that it has received reports of fewer than fourteen hundredcovid-19 hospitalizations and three hundred deaths among them. This means that, after vaccination, one’s chances of dying of covid-19 are currently about two in a million, with the likelihood of being hospitalized only slightly higher. Statistics reported by hospitals tend to be accurate; still, even if state governments have missed a few cases here and there, the results are staggeringly good. “The evidence on vaccines just keeps getting better and better,” Robert Wachter, a physician and the chair of medicine at the University of California, San Francisco, told me. “When the trial results first came out, I thought, They can’t actually be this good. The real world is always messier than the trials. What we’ve learned since then is that the vaccines are probably even more spectacular than we initially believed.”
The answer to the second question—whether the vaccines work against the major coronavirus variants—is also now clear. Earlier this month, a study conducted in Qatar, where the B.1.1.7 and B.1.351 variants predominate, found that the Pfizer-BioNTech vaccine was ninety-seven per cent effective at preventing severe disease. Vaccines from Moderna and Johnson & Johnson also appear to be highly effective against the variants; in fact, these vaccines are already successfully fighting them here in the United States. The B.1.1.7 variant, which is vastly more contagious than the original virus and caused a devastating surge in the U.K. this past winter, now accounts for three-quarters of new U.S. cases—and yet, largely thanks to vaccination, daily infections in this country have fallen by nearly ninety per cent since their peak in January, and are now lower than at any point in the past eight months. The existence of more contagious variants isn’t a reason to doubt the vaccines but to vaccinate people as quickly as possible.
As for the final question—whether vaccinated people can spread the virus to others, especially unvaccinated people, including children—the evidence is similarly encouraging. Because vaccinated people are unlikely to contract the virus, the vast majority won’t be passing it on. And even the small number of vaccinated people who experience breakthrough infections have much less of the virus circulating in their bodies, and may be less infectious. Real-world data from Israel, which has mounted one of the world’s fastest and most effective vaccination campaigns, is instructive. The country’s progress in immunizing its adults has been linked to significant declines in infections among unvaccinated people; according to one preliminary estimate, each twenty-percentage-point increase in adult vaccination rates reduces infections for unvaccinated children by half. When vaccinated people remove their masks, they pose little threat to others, and they face little peril themselves.
The shift toward reopening is not without risk. The first issue is timing. Less than half of Americans have received even one shot of a covid-19 vaccine, and only around four in ten have been fully vaccinated. This means that the majority of the country remains susceptible to infection and disease. Meanwhile, the pace of vaccinations has slowed: in April, the U.S. was routinely vaccinating about three million people per day, but the daily average is now nearly two million. It’s unclear whether the new guidance will encourage or deter unvaccinated Americans from getting immunized. In a recent survey, unvaccinated Republicans said that they would be nearly twenty per cent more likely to get the shots if it meant that they wouldn’t have to wear a mask anymore. We’ll now find out how they really feel.
Vaccine hesitancy is only part of the picture. Some thirty million Americans—a group larger than anti-vaxxers or the vaccine-hesitant—say that they want to get immunized but haven’t yet done so. Some face language barriers, or fear immigration problems; others have difficulty navigating the health system, or can’t take time off from work. Many of the willing-but-unvaccinated are working-class Americans; four in five don’t have a college degree. The Biden Administration has sent billions of dollars to health centers serving low-income populations, offered tax credits to businesses that provide paid time off for employees to get immunized, and helped assemble thousands of volunteers—known as the covid-19 Community Corps—to assist with vaccine outreach to underserved populations. States, too, are trying to reduce barriers to vaccination, and offering incentives—including payments in Maryland, a lottery in Ohio, and a “Shot and a Beer” program in New Jersey—for residents who remain on the fence. There are, in short, real efforts under way to sway the vaccine-hesitant and make vaccines more accessible.
Still, the new C.D.C. guidance makes these efforts even more urgent. Until now, unvaccinated people have been shielded from high levels of viral exposure by government mandates and social norms that have kept their friends, neighbors, and colleagues masked and distanced, to varying degrees. But, in the coming weeks, those protections will likely erode. For unvaccinated Americans, this could be the most dangerous moment in the pandemic. In most contexts, there is no reliable mechanism for verifying who has and hasn’t been vaccinated. Inevitably, against the C.D.C.’s advice, many unvaccinated people will resume normal life, too, threatening their own health and that of others. When asked how businesses are to know which customers can enter unmasked, Anthony Fauci, the nation’s top infectious-disease expert, told CNN, “They will not be able to know. You’re going to be depending on people being honest enough to say whether they were vaccinated or not.”
“Unvaccinated people are now going to have much higher levels of exposure,” Wachter told me. “That’s especially true in places with lots of community spread and in places where more contagious variants are circulating.” Wachter suggested that the C.D.C. could be making an epidemiological bet. The move “will cause some additional covid cases that otherwise would not have occurred,” he said—but, “if it leads to even a small uptick in vaccination, it will save lives in aggregate.”
Since the start of the pandemic’s second chapter, public-health officials have been working to prevent a catastrophic collision between the ship of reopening and the iceberg of the unvaccinated. By slowing the speed of the ship or shrinking the size of the iceberg, we have sought to reduce the force of the collision. But barring a hundred-per-cent vaccination rate, or something close to it—an outcome that the U.S. was never likely to achieve—a crash of some sort has been inevitable.India’s collision has been titanic—it reopened with a population of more than a billion, even though hardly anyone was vaccinated. In the U.S., the situation is different. Our iceberg has been melting, and we’ve been approaching it slowly. Now we’re taking off the brakes.
The C.D.C. issues guidance, not laws; there are several quantitative measures that states, counties, cities, companies, and individuals can consult in pacing their reopening and squaring the agency’s broad recommendations with local realities. A community’s immunization rate is perhaps the most obvious statistic to track. Experts have argued for meeting a seventy-per-cent immunity threshold before relaxing masking and distancing requirements. No states have got there yet, although some, such as Vermont and Maine, are well on their way. The Biden Administration has said that it hopes to hit the seventy-per-cent target for first shots by the Fourth of July.
Because the vaccines prevent almost all cases of severe covid-19, the number of covid-19 hospitalizations is another good metric to watch. “With vaccines, cases become uncoupled from severe disease,” Monica Gandhi, an infectious-disease doctor at the University of California, San Francisco, who has studied asymptomatic coronavirus transmission, told me. Gandhi was among the first researchers to show that masks protect not just others but wearers, too; when we spoke, before the C.D.C.’s announcement, she said that, in her view, most precautions could end when half of Americans had received their first shot and covid-19 hospitalizations had fallen below sixteen thousand nationally, or about five per hundred thousand people. (At the peak of most flu seasons, the U.S. records five to ten influenza hospitalizations per hundred thousand.) Hospitalizations appear to be falling, unevenly, across the country. However, there are currently thirty thousand Americans hospitalized with covid-19—roughly a quarter of the January peak, but still about twice Gandhi’s threshold.
Herd immunity offers a third benchmark for reopening. The idea is that, once about eighty per cent of the population has been vaccinated or infected, the virus will struggle to spread. Recently, some experts have argued that we might never get to herd immunity because of variants, vaccine hesitancy, and the fact that children under twelve, who make up some fifteen per cent of the U.S. population, are unlikely to be immunized for some time. But the C.D.C.’s recommendation could change the equation. As states lift restrictions and unvaccinated people face higher levels of exposure, more of them are likely to get infected, pushing us closer to the herd immunity threshold. In all likelihood, the U.S. will be able to reach sixty-per-cent vaccination in the coming weeks; meanwhile, perhaps a third of Americans have already been infected. Even assuming significant overlap between the two groups, the combination of vaccination and infection is likely to make it harder for the virus to find new hosts. Marc Lipsitch, the director of Harvard’s Center for Communicable Disease Dynamics, emphasized that, because some parts of the country may reach herd immunity, or something close to it, before others—Connecticut’s current covid-19 immunization rate, for instance, is nearly twice Mississippi’s—unvaccinated adults will face different levels of risk depending on where they live. “There won’t be one national end,” Lipsitch told me. “We’re going to see a fundamental change in terms of what it means to live in this country, but there’s also going to be a lot of local variation.”
Covid-19 deaths give us another way of tracking the pandemic. Experts have argued that the U.S., with a population of three hundred and thirty-two million, should aim for fewer than a hundred coronavirus deaths daily—roughly the toll of a typical flu season. Right now, America is seeing about six hundred covid-19 deaths each day; according to the Institute for Health Metrics and Evaluation, which generates one of the country’s most widely cited pandemic models, that number will likely fall to about a hundred in August. “Things will look very good this summer,” Christopher Murray, the director of the I.H.M.E., told me. “A lot of people will think that we’re done, that it’s all over. But what happens in the fall is the tricky part.” Murray believes that a confluence of factors—the spread of variants, in-person schooling, meaningful numbers of still-unvaccinated people, and the seasonality of the virus—will produce a small winter spike, concentrated in communities with low vaccination rates. It won’t be the apocalyptic surge of New York City in the spring of 2020—or, more recently, those of India or Brazil—but, each week, several thousand unvaccinated Americans could die.
It’s possible, given all this, to imagine a plausible scenario for the conclusion of the American pandemic. The coronavirus disease toll continues to fall throughout the summer. States do away with mask mandates and capacity restrictions; people increasingly return to bars, spin classes, and airports, then to stadiums, movie theatres, and concerts. By midsummer, in communities with high vaccination rates, covid-19 starts to fade from view. In those places, even people who remain unvaccinated are protected, because so little of the virus circulates. But, in other parts of the country, low immunization rates combined with reopening allow the disease to register again. Hospitals aren’t overwhelmed—there’s no need to build new I.C.U.s or call in extra staff—but the collision between ship and iceberg is forceful, and each week thousands of people fall ill and hundreds die. Some victims are vaccine-hesitant; others were unable, for whatever reason, to get vaccinated. Still, perhaps unfairly, these outbreaks come with an aura of culpability: to people in safe parts of the country, the ill seem like smokers who get lung cancer.
In the fall, many unvaccinated children return to school. Scattered infections among them capture headlines, but serious illnesses are exceedingly rare; the overwhelming majority of children remain safe, and, with time, they, too, are immunized. The U.S. approaches something like herd immunity. Some people may still fall ill and die of covid-19—perhaps they are immunocompromised, elderly, or just unlucky—but, by and large, America has gained the upper hand. Meanwhile, in poor nations with few vaccines, the pandemic continues. As crisis wanes in one country, catastrophe ignites in another. Every so often, we learn of a new variant that’s thought to be more contagious, lethal, or vaccine-resistant than the rest; we rush to institute travel bans, only to learn that the variant, or a close cousin, is already circulating in the U.S. and has been largely subdued by the vaccines, as all previous variants have been. In the fall, Americans line up for covid booster shots alongside flu vaccines. The pandemic’s final chapter comes to a close not through official decree but with the gradual realization that covid-19 no longer dominates our lives.
Reopening a country after a pandemic isn’t like flipping a giant switch. It’s more like lighting a series of candles, illuminating one part, then another, until the whole place shines. Many states, counties, cities, and businesses will further loosen their restrictions; others will wait. Communities and individuals will approach the end of the crisis differently, as they’ve approached the rest of it. Some unvaccinated people have already been forgoing precautions; on the other hand, I’ve been vaccinated for months and, since the C.D.C. announcement, have yet to leave my mask behind—whether because of a lingering, irrational fear or simply to avoid dirty looks, I can’t say. Social norms take time to change, even when one of the world’s most respected public-health agencies is telling you to change them.
The pandemic has created not just chaos and suffering but uncertainty. It’s easy, therefore, to be doubtful about the fortunate position in which we seem to find ourselves now. As a physician, I spent the early months of the pandemic caring for covid-19 patients in New York City; they streamed into the hospital day after day, deathly ill. We raced to build covid wards, I.C.U.s, and hospice units. At the time, we had little to offer. There were no proven therapies, and certainly no vaccines. There were weeks when thousands of New Yorkers died, many of them alone in their final moments, while more people were dying across the world. I felt fear, anxiety, and sometimes despair. The scale of the damage—the lives lost, businesses shuttered, dreams shattered, children orphaned, seniors isolated—was crushing, and the path forward was both frightening and unknown.
As good news began to arrive, I greeted it with a blend of guarded skepticism and cautious optimism. First came evidence that outdoor transmission was unlikely. Then we learned that contaminated surfaces rarely spread disease; that some patients can breathe better simply by lying on their bellies; that P.P.E. works; that dexamethasone saves lives. We discovered that immunity lasts many months, perhaps years; that repeat infections are unlikely; and that variants present a surmountable challenge.
Now, study after study, in country after country, has shown that the vaccines are capable of transforming a lethal pathogen into a manageable threat. Examining and reëxamining the vaccine results, I’ve gone through stages, too—caution, hope, and, finally, clarity. We really are that close. The beginning of the end is here.
“A vaccinated friend attended an indoor gathering of 35 people, half of which were unvaccinated. Nobody wore masks or socially distanced. I am vaccinated, but should I avoid contact with this person for some period of time? I am concerned that my friend may have inadvertently been exposed to variants, although no problems as of three days post-event.”
The scenario you describe is likely to be low risk to you and your friend because you’re both vaccinated. It’s not ideal — mostly from the perspective of the people at the meet-up who weren’t vaccinated yet. When non-immunized and immunized people gather in a space, precautions should account for those who haven’t had their shots yet, the Centers for Disease Control and Prevention advises. Those precautions include everyone wearing masks inside in public or indoors if there’s a multi-household mix of people who aren’t vaccinated.
Mingling indoors without masks or distancing is “likely low risk for the vaccinated people,” the CDC writes (the emphasis is the agency’s). That’s because the vaccines are so protective.
Real-world results continue to support clinical trial conclusions that coronavirus vaccines are highly effective at preventing symptomatic covid-19. In a CDC study of almost 2,500 fully vaccinated health-care workers, only three had confirmed infections. “Front-line workers were 90 percent less likely to be infected with the virus that causes covid-19,” an epidemiologist and author of that study told The Post last month.
Emerging reports also suggest vaccines hinder asymptomatic infection. Two doses of an mRNA vaccine reduced that by 92 percent in Israel, according to a study published this week in The Lancet. And there’s encouraging news that vaccines protect against variants of concern. As we mentioned above, and reported Wednesday, research in the New England Journal of Medicine showed the Pfizer-BioNTech vaccine was “90 percent effective at blocking infections caused by the B.1.1.7 variant,” which is the more transmissible variant first detected in the U.K. The vaccine was slightly less effective, at 75 percent, against the B.1.351 variant identified in South Africa.
It’s good to hear that there haven’t been any problems in the days after this gathering. From what you’ve described, it doesn’t sound as though your friend needs to take any actions like quarantining. In fact, the CDC advises quarantine is generally unnecessary for fully vaccinated people, even after known exposure, unless an immunized person begins to show symptoms.
That said, you’ve asked journalists, not doctors — here’s our usual disclaimer to consult your primary-care physician if you have specific concerns about your susceptibility to the virus. If you’re wary about jumping back into social life, that’s okay, too, and not unusual after living through an ongoing pandemic. Some psychologists suggest easing into social situations post-vaccination, borrowing from principles of exposure therapy; for instance, if you’re anxious and would like to take extra precautions for your next visit with your friend, you might suggest meeting up while outside or you can wear a mask.
Cambridge-based Massachusetts Institute of Technology professors Martin Bazant and John Bush, PhD, developed a model to calculate indoor exposure risk to COVID-19 by factoring in the amount of time spent inside, air filtration and circulation, immunization, variant strains, mask use, and respiratory activity such as breathing, eating or talking.
“We argue there really isn’t much of a benefit to the six-foot rule, especially when people are wearing masks,” Mr. Bazant told CNBC. “It really has no physical basis because the air a person is breathing while wearing a mask tends to rise and comes down elsewhere in the room so you’re more exposed to the average background than you are to a person at a distance.”
As with smoking, even people wearing masks can be affected by secondhand smoke that makes its way around the enclosed area and lingers. The same logic applies to airborne droplets of the virus, according to the study. However, the study did note that mask use by both infected and susceptible people reduces “respiratory plumes” and thus increases the amount of time people may safely spend together indoors.
When crafting guidelines, the CDC and World Health Organization have overlooked the amount of time spent indoors, Mr. Bazant claims.
“What our analysis continues to show is that many spaces that have been shut down in fact don’t need to be,” Mr. Bazant said. “Oftentimes, the space is large enough, the ventilation is good enough, the amount of time people spend together is such that those spaces can be safely operated even at full capacity, and the scientific support for reduced capacity in those spaces is really not very good.”
Opening windows or installing new fans to keep air moving may be just as effective or more effective than purchasing a new filtration system, Mr. Bazant said.
The CDC currently recommends staying at least 6 feet away from other people and wearing a mask to slow the spread of COVID-19, citing the fact that the virus spreads mainly among people who are in close contact for a prolonged period.
“The distancing isn’t helping you that much and it’s also giving you a false sense of security, because you’re as safe at six feet as you are at 60 feet if you’re indoors. Everyone in that space is at roughly the same risk, actually,” Mr. Bazant said.
After three rounds of peer review, Mr. Bazant says he hopes the study will influence social distancing policies.
All the things that could prolong the COVID-19 pandemic — that could make this virus a part of our lives longer than anyone wants — are playing out right in front of our eyes.
Driving the news: The British variant is driving another surge in cases in Michigan, and Gov. Gretchen Whitmer has resisted reimposing any of the lockdown measures she embraced earlier in the pandemic.
Variants are beginning to infect more kids — “a brand new ball game,” as University of Minnesota epidemiologist Michael Osterholm recently put it.
New research confirms that our existing vaccines don’t work as well against the South African variant.
And some experts fear the pace of vaccinations in the U.S. is about to slow down.
Between the lines:The concern isn’t necessarily that the facts on the ground right now could end up being disastrous, but rather that we’re getting a preview of the longer, darker coronavirus future the U.S. may face without sufficient vaccinations.
If we don’t control the virus well enough, then even years into the future, we could be living through more new variants — some of which might be more deadly, some of which might be more resistant to vaccines, some of which might be more dangerous for certain specific populations.
That would translate into an ongoing risk of illness or potentially death for unvaccinated people and new races to reformulate vaccines as new variants keep emerging.
And it would lead to a world in which today’s vaccine-eager population would have to stay on top of those emerging risks, get booster shots when they’re available, and perhaps revive some of the pandemic’s social-distancing measures, in order to stay safe.
Centers for Disease Control and Prevention (CDC) Director Rochelle Walensky finds herself in a delicate position as she seeks to balance the optimism of increasing vaccinations with the reality that the U.S. is still very much in the grip of a deadly pandemic.
Walensky started the CDC job with a reputation as a savvy communicator, tasked with salvaging the reputation of an agency that took a beating under the Trump administration.
“When I first started at CDC about two months ago, I made a promise to you: I would tell you the truth, even if it was not the news we wanted to hear,” Walensky told reporters recently.
Walensky’s expertise is in HIV research, like her predecessor Robert Redfield, and before being appointed to lead the CDC, she was head of infectious diseases at Massachusetts General Hospital.
While former colleagues say Walensky is the perfect fit for the CDC post, her skills are now being put to the test as she faces criticism for being both too negative and too hopeful.
“She is quite a compelling and clear communicator, but it’s a challenging set of messages to try and get out there,” said Chris Beyrer, a professor of epidemiology at Johns Hopkins Bloomberg School of Public Health.
Public health messaging during a global pandemic is complicated enough, but experts say this particular moment is especially difficult.
After weeks of decline and then stagnation, the rate of coronavirus infections has once again started to climb across much of the country. Cases are up about 12 percent nationally compared with the previous week, averaging around 62,000 cases per day, according to the CDC.
At the same time, nearly 100 million Americans have received at least one dose of a coronavirus vaccine. Many states are expanding vaccine eligibility, in some instances to all adults, and federal health officials say there will be enough supply for everyone to be vaccinated by the end of May.
Walensky tried to emphasize both aspects this week when she issued an emotional appeal to the public.
“We have so much to look forward to, so much promise and potential of where we are, and so much reason for hope. But right now I’m scared,” Walensky said, adding that she had a “sense of impending doom” if people continued to ignore public health precautions.
Yet almost in the next breath, she talked about a “tremendously encouraging” new study showing that vaccinated people were 90 percent protected from infection, meaning they pose an extremely low risk of spreading the virus.
While that may come across as mixed messaging, experts say it accurately reflects not only where things stand right now but also how the country has been reacting to the virus for the past year.
“Whiplash is a true reflection of how we’re all experiencing the epidemic and the response to it. So I’d rather she be honest about that and others be honest about that than give people something that they want … to make them feel better,” said Judith Auerbach, a professor in the University of California San Francisco School of Medicine.
Auerbach, who previously worked with Walensky on HIV research, praised the director’s openness, which she said had been missing from agency leadership during the Trump administration.
“She’s being really honest about her own emotions. That’s hard for a fed to do and get away with,” Auerbach said. “The science that says we all still need to be, in fact, quite scared because we’re in this race between the vaccines … versus the emergence of these variants, and she felt it at a visceral level, and she conveyed that in a way that I thought was quite telling.”
Glen Nowak, director of the Center for Health and Risk Communication at the University of Georgia and a former CDC media relations director, said Walensky’s candor helps establish credibility.
“She has embraced the fact that credibility comes from being transparent and honest and genuine about your fears and your concerns,” Nowak said.
The CDC declined to make Walensky available for an interview, but in a statement to The Hill, an agency spokesman said every communication reflects the latest science and epidemiology.
“At times, moments must balance hope that we will move out of the pandemic with the reality that we are not out of it yet,” the spokesman said.
“We acknowledge the challenge of conveying such hope and promise that vaccines offer with the reality that cases and deaths are rising. While we are sending the critical message that people cannot and should not let up on their prevention measures, we do remain very optimistic about what the future of a fully vaccinated public will offer,” the spokesman added.
On Friday, Walensky again came under criticism for her messaging. In updated guidance, the CDC said it is safe for people who have been fully vaccinated to travel.
But Walensky struck a cautionary tone by saying the CDC still recommends anyone, vaccinated or not, avoid nonessential travel because infection numbers are so high.
“We know that right now we have a surging number of cases,” Walensky said during a White House briefing. “I would advocate against general travel overall. Our guidance is silent on recommending or not recommending fully vaccinated people travel. Our guidance speaks to the safety of doing so.”
Nowak said part of what makes public health messaging so difficult is the fact that science doesn’t always deal in absolutes and that the public overall doesn’t do well with nuance.
“Often people don’t want to listen to the nuance; they want advice and guidance to be stable. They get frustrated with the changes or when it seems to be contradictory. They also get frustrated if it doesn’t match their everyday living experiences,” Nowak said.
With the travel guidance, Walensky attempted to spell out the balance she was trying to strike and asked the public for patience and understanding.
“I want to acknowledge today that providing guidance in the midst of a changing pandemic and its changing science is complex,” Walensky said.
“The science shows us that getting fully vaccinated allows you to do more things safely, and it’s important for us to provide that guidance, even in the context of rising cases.At the same time, we must balance the science with the fact that most Americans are not yet fully vaccinated, which is likely contributing to our rising cases,” she said.
Jen Kates, director for global health and HIV policy at the Kaiser Family Foundation, who has known Walensky for decades, said she thinks the CDC director is aware that she can’t escape criticism, especially when so many people have pandemic fatigue.
If the CDC is too strict and refuses to endorse relatively normal behavior, especially after people get vaccinated, it could risk others refusing to get the shot, Kates said.
But if the agency paints too rosy a picture, more people could act like the pandemic is over and risk further spread of the virus.
“It behooves public officials to always be cognizant that their words are being listened to and can be taken out of context or may be hard for people to grasp,” Kates said. “So I think Dr. Walensky is a great communicator, but that doesn’t mean that this is always easy to do and the balance is always straightforward.”