
Cartoon – Making Healthcare Affordable Again

As open enrollment begins and Congress remains deadlocked on whether to extend the ACA’s enhanced premium subsidies, one question looms large: Where does all the money we pay for health coverage actually go?
It’s a fair question. Premiums and out-of-pocket costs have risen relentlessly over the past decade. Since the Affordable Care Act was fully implemented, the average premium for an ACA marketplace plan has doubled, and the average deductible for a Silver plan has increased by 92%. Every year, families pay more, yet the coverage often feels thinner.
Health insurance companies routinely claim these increases simply reflect rising medical costs and higher utilization. For example, when justifying rate hikes in 2024, Cigna of Texas wrote:
“The increasing cost of medical and pharmacy services and supplies accounts for a sizable portion of the premium rate increases.”
But the financial filings of these same companies tell a different story.
As Wendell Potter recently wrote, from 2014 to 2024 the seven largest publicly traded health insurance companies, UnitedHealth Group, CVS/Aetna, Cigna, Elevance (formerly Anthem), Humana, Centene, and Molina, reported that they collectively made more than half a trillion dollars in profits.
That’s money collected from individuals, employers and taxpayers for health coverage — dollars that didn’t go to medical care but instead flowed to corporate shareholders and executive bonuses. To put this in perspective, those profits alone could fund the enhanced ACA premium subsidies for another ten years, at an estimated cost of $350 billion.
Over the same period, these seven companies spent $146 billion buying back their own stock or, in other words, using premium dollars from patients and employers to boost share prices and executive compensation (the CEOs and many other top executives of big insurers are compensated primarily through stock grants and options).
Stock buybacks don’t lower premiums, expand networks, or improve care. They simply make investors and executives richer. If that same money had been reinvested in enrollees, it could have provided premium-free health coverage to more than 5 million families for an entire year, based on the average employer-sponsored plan cost of $27,000 in 2026.
Insurers aren’t just rewarding shareholders, they’re also shaping the political system that protects their profits. Since 2014, the seven largest insurers and their trade association, AHIP, have spent $618 million on lobbying.
That’s money that could have been used to lower out-of-pocket costs or improve patient care, but instead it’s spent to influence Congress and federal agencies to maintain the status quo.
As the cost of health insurance continues to climb, politicians debate how to control those costs and expand coverage. But the truth is, there’s already enough money in the system to cover everyone. It’s just being siphoned off by insurance corporations for profits, lobbying, and stock buybacks.
Though some have been calling for less regulation of Big Insurance, that is not the answer and is partly how we ended up in this situation. Right now, Big Insurance is allowed to use premium dollars and tax dollars on things that do nothing to improve anyone’s health – such as stock buybacks and lobbying – instead of on medical care.
Rather than asking families and taxpayers to pay more, it’s time to demand accountability from insurers. At a minimum, they should not be allowed to use premium dollars, or taxpayer dollars, to enrich shareholders through stock buybacks (which wasn’t even legal until the 1980s) or lobby for policies that drive up costs.
If we want to contain health care costs, the first step is simple: Stop the profiteering by Big Insurance.
Elevance’s Anthem Blue Cross plans are joining Big Insurance’s latest profit play — cutting payments to hospitals and providers under the pretense of reducing patients’ out-of-pocket costs.
Anthem Blue Cross plans have joined UnitedHealth and Cigna in taking extreme measures to satisfy Wall Street but penalize hospitals and potentially thousands of doctors and physician groups that Anthem excludes from its provider networks.
What Anthem is proposing is not only extreme but brazen in that it goes way beyond what any managed care company I know of has ever undertaken to pad its bottom line by reducing patient choice. It wouldn’t just restrict access to certain providers, it would effectively eliminate access.
Anthem, which is owned by the for-profit corporation Elevance Health Inc., has notified hospitals in 11 of the 14 states where it operates that starting in January it will slash reimbursements by 10% every time a doctor who works in the hospital – but who is not in Anthem’s network – provides care to a patient enrolled in an Anthem health plan.
The move clearly will save Elevance money and help it meet its shareholders’ profit expectations, but it will be a potential nightmare and administrative expense for thousands of hospitals and outpatient facilities. And it could put many independent physician practices out of business.
As Fierce Healthcare reported Friday, Anthem will impose an administrative penalty equal to 10% of the allowed amount on a hospital or outpatient facility’s claims that include out-of-network providers. If those facilities don’t meet Anthem’s terms, they will be at risk of being dropped from Anthem’s network.
Anthem’s announcement comes on the heels of UnitedHealth’s disclosure to investors last month that it plans to dump thousands of doctors from its networks to boost profits. A UnitedHealth executive said during the company’s third quarter call with shareholders that there were too many doctors in the company’s network who were not aligned with UnitedHealth’s business model, which he called “value-based care.”
“We are moving to employed or contractually dedicated physicians wherever possible,” said Patrick Conway, CEO of UnitedHealth’s Optum division, which has bought hundreds of physician practices over the past several years. UnitedHealth is already the biggest employer of doctors in the country.
And last month, Cigna began reducing payments to many doctors automatically by resurrecting a practice called downcoding that was banned by a federal court more than two decades ago. Cigna also is threatening to drop hundreds of hospitals and outpatient facilities operated by Tenet Health from its provider network next year.
The stock prices of all three insurers have been under pressure this year as shareholders have sold millions of their shares in reaction to what they consider bad news from the companies. Most investors consider increases in paid medical claims to be bad news and a threat to the value – and earnings potential – of their holdings.
Anthem claimed in its notice to hospitals and other facilities last month that it is implementing the new policy “to support patient care and to help reduce out-of-pocket expenses for our members.” The notice went on to say that, “As a participating facility in Anthem’s care provider network, your role in guiding members to in-network care providers is vital in ensuring members receive high-quality, cost-effective, and coordinated care.”
Sounds good, right? But how is a patient to know that the doctors in Anthem’s network are really the ones that truly deliver high-quality coordinated care? Could it be that the top priority of the insurer is to include providers in its network who agree, first and foremost, to reimbursement terms especially favorable to the insurer?
And for hospitals, this could lead to higher administrative costs in trying to figure out which doctors are available at any given time to treat an Anthem patient. A highly regarded anesthesiologist might be just fine – and available – to treat patients insured by Cigna or Aetna or Humana, but off limits to treat an Anthem-insured patient. The hospital will have to be especially vigilant to keep that doctor out of the operating room when an Anthem patient needs surgery. If it slips up the hospital could get booted out of Anthem’s network. The doctor, however, would not be able to bill the patient for any amount because of the federal No Surprises Act (NSA), which prohibits balance-billing.
Anthem’s claim that it is taking this action to reduce patients’ out-of-pocket expenses is especially rich when you remember that Anthem and other big insurers created the problem Anthem says it is seeking to address. Anthem, Cigna, UnitedHealth and other big insurers led what became an industry-wide strategy in the early 2000s to force as many of their health plan enrollees as possible – and as soon as possible – into high-deductible plans. That strategy was so successful that more than 100 millions Americans – the vast majority of whom have health insurance – are mired in medical debt.
Fierce Healthcare quoted an Elevance executive as saying that the new Anthem policy “was designed in response to provider behavior under the independent dispute resolution (IDR) process” established by the No Surprises Act. He said Anthem had seen “a consistent pattern of IDR being used as a ‘back-door payment channel’ for pricey, nonemergent procedures.”
But as HEALTH CARE un-covered reported recently, research is showing that insurers are manipulating the IDR process to their advantage by exploiting loopholes in the NSA. Doctors have told me that even when they prevail in a dispute, insurers often refuse to pay promptly, if at all, and they report long delays, repeated administrative hurdles, and in some cases outright nonpayment of arbitration awards. And a report published last week in Health Affairs describes the “hidden incentives” of insurers in the IDR process that the authors say add costs to health plans and beneficiaries “and the health care system at large.”
Independent practice physicians have begun raising alarms about Anthem’s new policy. And on Wednesday, medical societies representing thousands of doctors sent a letter to Elevance CEO Gail Boudreaux protesting Anthem’s plans and asking for a meeting.
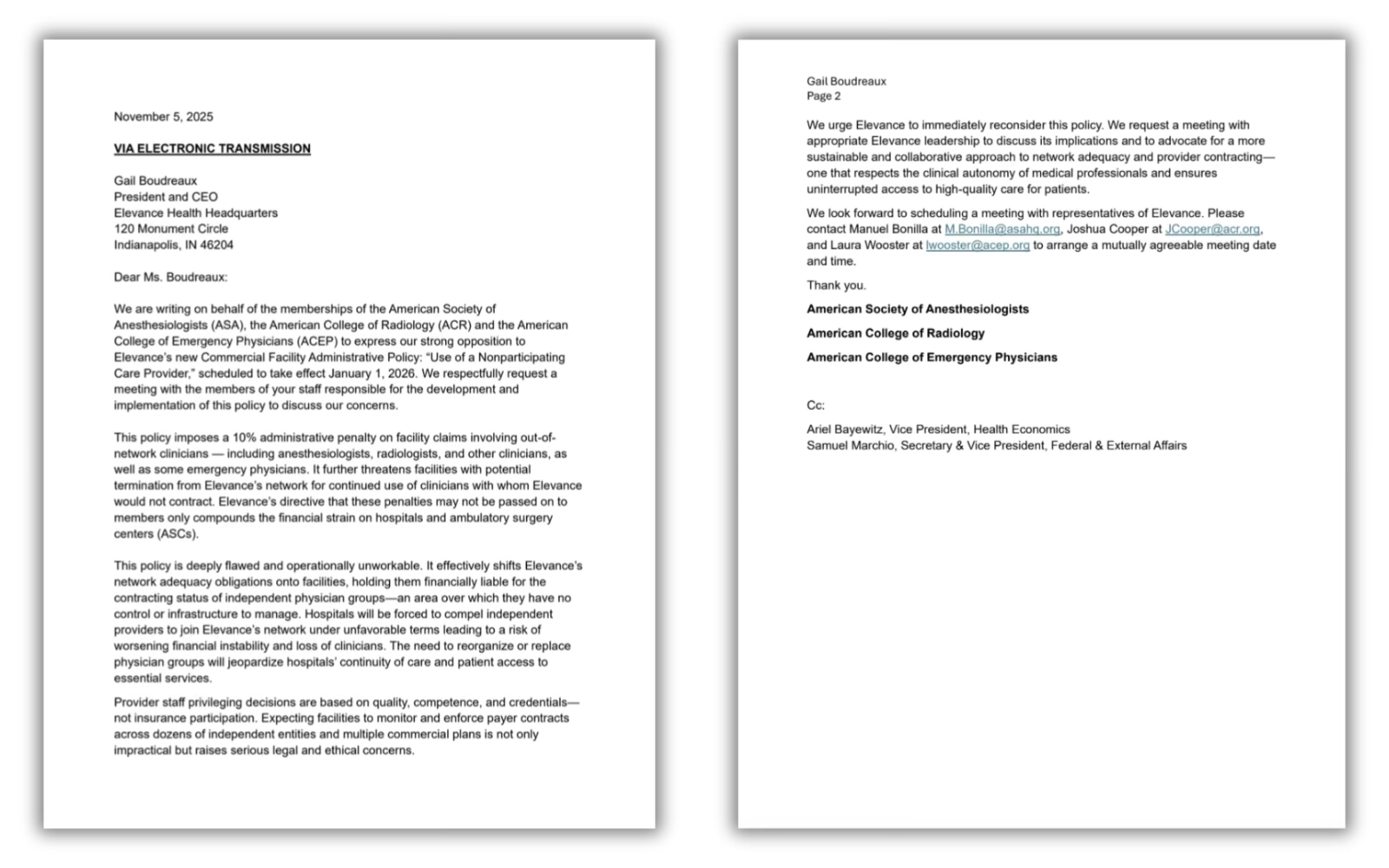
“This policy is deeply flawed and operationally unworkable,” they wrote. “It effectively shifts Elevance’s network adequacy obligations onto facilities, holding them financially liable for the contracting status of independent physician groups–an area over which they have no control or infrastructure to manage. Hospitals will be forced to compel independent providers to join Elevance’s network under unfavorable terms leading to a risk of worsening financial instability and the loss of clinicians. The need to reorganize or replace physician groups will jeopardize hospitals’ continuity of care and patient access to care.”
The letter went on to say that, “Expecting facilities to monitor and enforce payer contracts across dozens of independent entities and multiple commercial plans is not only impractical but raises serious legal and ethical concerns.”
If the doctors can’t persuade Boudreaux to ditch the new policy, people enrolled in Anthem plans who need care in a hospital or outpatient facility next year could face confusion and delays in getting that care, and the facilities currently in their network might be kicked out of it if they make any mistakes.
Doctors’ concern about Anthem’s policy cannot be dismissed as an overreaction to one company’s business decision. It poses an existential threat to physician practices that want to stay independent and not sell out to either a hospital system or an insurance company. If the other health insurers follow Anthem’s lead – and there is no reason to think they will not – the number of doctors in independent practice in the United States will dwindle to extinction. There aren’t many left as it is.
Because of the control Wall Street now has over the health insurance industry, Boudreaux is likely less concerned about physician autonomy than what investors think and want, and she is under the gun to get back into their good graces in a matter of months. Her company’s shares have lost a third of their value since the first of this year. If she can’t demonstrate that she’s getting Elevance back on track to profitable growth, she’ll be out of a job soon.
Lawmakers and regulators at all levels of government need to keep an eye on this and intervene if doctors and Anthem patients can’t change her mind.
In what political pundits called a sweeping win by Democrats in Tuesday’s elections, affordability and costs of living emerged as the issues that mattered most to voters. It’s no surprise.
Since 2019 before the pandemic, prices have increased for American businesses and households due to inflation:
Personal Consumption Expenditures (PCE) inflation which measures monthly business spending increased 3.5% annually. The Consumer Price Index (CPI), which measures monthly changes in household spending increased 3.87% annually over the same period (2019-2025).
But in the same period, prices for healthcare services–hospitals, physician services, insurance premiums and long-term care–have taken an odd turn: for businesses, they’ve decreased but for consumers, they increased.
It reflects the success whereby businesses have shifted health benefits costs to employees or suspended benefits altogether, and it explains why consumers are bearing more direct responsibility for healthcare costs and are increasingly price sensitive.
A proper interpretation of PCE and CPI data points to a bigger problem: household exposure to increased prices hits younger, middle-income households hardest because their housing costs consume 36-60% of their disposable income. Food costs are an additional 13-20%. That doesn’t leave much room for healthcare when child care, student debt and transportation costs are factored.
| Category | PCE | CPI | CPI Weight |
| 2019-2025 CumulativeAnnual change | +17.3%+3.5% | +26%+3.87 | 100% |
| 2019-2025 Cumulative Healthcare Services Annual Change | -11.6%-1.85% | +16.8%+2.56% | 6.7% |
| 2019-2025 Cumulative Food CostAnnual Change | +24.5%+3.7% | +30.98+4.6% | 14.5% |
| 2019-2025 Cumulative Housing CostAnnual Change | +18-22%+3.2% | +25-28%+4.2% | 44.2% |
| 2019-2025 Cumulative Transportation CostAnnual Change | +28-32%+4.8% | +35-40%+5.5-6.0% | 15.1% |
Sources: Personal Consumption Expenditures Price Index | U.S. Bureau of Economic Analysis (BEA), CPI Home : U.S. Bureau of Labor Statistics
Increased attention to household affordability and costs of living is uncomfortable in the healthcare industry. The good news is that expenses for health services represents a small fraction of spending; the bad news is those expenses are increasing along with competing categories and they’re sometimes unpredictable.
The fundamental operating model in healthcare is ‘Business to Business/B2B’ transactions between producers (physicians, hospitals, drug and device makers), middlemen (insurers, PBMs, employers) and users (consumers) reinforced by state and federal regulation that protect the status quo. And ‘users’ are treated as patients or enrollees, not a market that makes buying decisions based on value and costs. Thus, lack of price transparency in healthcare coupled with lack of predictability when services are used lends to public confusion or, in extreme cases, contempt. The public reaction to the murder of UnitedHealth Executive Brian Thompson last year surfaced the public’s latent animosity toward healthcare’s business practices that treat consumers as pawns on a complicated chessboard.
Shifting direct financial responsibility to consumers is the blunt instrument touted by economists who rightly argue informed decision-making by consumers is necessary to lower costs and improved value from the system. It won’t happen overnight if at all, and the system’s affordability in working age households will be the impetus.
The near-term implications are clear:
Increased household discretionary spending for necessities (food, transportation, and housing) will shrink discretionary spending for healthcare products and services:
Consumers (voters) will support policy changes to the health system that increase its accountability for affordability.
Final thought:
Throughout my career, ‘patient centeredness” has been the fundamental presumption on which service delivery by providers has been justified. Affordability has been neglected though increasingly acknowledged in rhetoric. Executives in healthcare services are not compensated for setting household affordability targets and publicly reporting results. Most compensation committees and Boards have marginal understanding of household economics in their communities and depend on “revenue cycle management” to address consumer payment obligations at arms-length. Even the medical community is not immune: one in 5 medical students is food insecure, 4 of 5 medical residents is financially insecure, and their career choices are increasingly dependent on their earning potential. So, calls for greater attention to affordability in healthcare will originate from insiders and outsiders tired of excuses and lip service.
Insecurity about household finances is significant and growing. Per the University of Michigan Index of Consumer Sentiment (50.3 in November 2025) is near an all-time low. It’s reality in the majority of U.S. households. The federal shutdown, discontinuance of SNAP benefits, cuts to ACA subsidies for insurance, corporate layoffs and higher costs for child care, groceries, gas and housing are a tsunami to American households.
Last week, voters elected: Zohran Mamdani, 34 (NYC); Abigail Spanberger, 46 (VA); and Mikie Sherrill, 53 (NJ) in races touted as a weather-vane for elections in 2026 and beyond. It is bigger than partisan elections. Voters in both parties and across the country are worried about affordability. It’s especially true among younger generations who worry about making ends meet and think institutions like the political system, higher education, organized religion and healthcare are outdated.
Healthcare service providers can ill afford to neglect affordability. It more than measuring medical debt, posting prices and referencing concern on websites. It’s about earning the trust and confidence of future generations through concrete actions that increase household financial security beginning with healthcare spending.
Paul
PS As never before, the voices of younger generations are being heard across the country though social media and demonstrations. The health system is among their major concerns as they ponder how they’ll be able to pay for their bills While Medicare seems the focus to policymakers and beltway pundits who rightly recognize seniors as its most costly population, the working age population has been taken for granted. Here’s a voice I follow closely. Fresh Perspective Is Sometimes Needed – by K. Pow
Navy SEAL Turned Hospital CEO: Jeff Mengenhausen Exposes Healthcare’s Failures

https://www.buzzsprout.com/1828354/episodes/18121411
What do a struggling student, a decorated Navy SEAL, and a hospital CEO all have in common? The answer: Jeff Mengenhausen.
In this explosive episode of the Crackin’ Backs Podcast, we sit down with the only Navy SEAL in the country running a hospital—a man who’s rewriting the rules of leadership, resilience, and what healthcare should really be.
Jeff’s story is anything but ordinary. Once labeled a “poor student,” he went on to earn Navy SEAL honors, a Purple Heart, and combat commendations. Today, he’s transforming Montrose Regional Health into one of the most respected community hospitals in the nation. But his mission doesn’t stop there—Jeff is exposing the cracks in America’s hospital culture and challenging the grip Big Pharma and profit-driven systems have on patient care.
Inside this episode, we ask:
This conversation isn’t just about medicine. It’s about survival, clarity under pressure, and the courage to flip a broken system on its head.
Learn more about Jeff Mengenhausen and Montrose Regional Health:
Episode 460 Navy SEAL Secrets for Healthcare Leadership with Jeff Mengenhausen

In this episode of the Lead Up Podcast, host Mike Harbour interviews Jeff Mengenhausen, CEO of Montrose Regional Hospital and Health System.
Jeff shares insights from his unique journey from Navy SEAL to healthcare executive, discussing how military leadership principles can be applied to civilian healthcare.
The conversation covers topics like maintaining team morale, the importance of culture in retaining talent, and the strategies Jeff employs to foster a winning mindset among his staff.
For anyone interested in leadership, resilience, and healthcare management, this episode offers valuable lessons and applicable insight.
If you enjoyed this episode, be sure to leave a 5-star review on your streaming platform. Mike encourages you to reach out to him through Mike@harbourresources.com to share your thoughts on this episode & to share some topics you would like him to cover in the future.

“The true character of society is revealed in how it treats its children.”- Nelson Mandela
Elected officials of both parties have proposed new and better government support for families with children. President Trump’s One Big Beautiful Bill Act includes some of these proposals, but overall, because of the law’s benefit cuts for working class and lower-income families, it will likely end up hurting roughly as many families with children as it helps.
This note describes some key changes embedded in OBBBA, some related proposals by Democrats, and some improvements that might be made in the future.
Politicians of both parties, who once made a show of kissing babies, have progressed to making a range of proposals to improve children’s lives and prospects. In some cases, perhaps frustrated by ongoing political polarization, they’ve chosen to support the same or similar approaches, including extra tax credits or actual payments for children and child savings accounts. For example, both Senator Ted Cruz (R-TX) and Senator Cory Booker (D-NJ) have proposed savings accounts be started for every child at birth.
Although the recently enacted OBBBA was in no way bipartisan, it included some proposals endorsed by both Republicans and Democrats. At the same time, however, the Act reduced the scope of the previously bipartisan SNAP safety net program and of Medicaid.

Furthermore, despite claims by representatives of both parties to support working families with children, the changes in OBBBA overwhelmingly help families that are already better off. After the temporary tax benefits end, roughly half of U.S. families will be worse off, with most benefits of the bill going to the top 40% of the income distribution.
Below, we discuss two kinds of assistance for families for children: those that provide immediate resources and those that support saving for children’s futures.
Congress has subsidized children through the tax code for at least a century, starting with dependent exemptions from income1 and following with the Earned Income Tax Credit in 1975 and the Child Tax Credit (CTC) in 1997. By far the most significant action benefitting some children in OBBBA is an increase in the CTC. However, most low-income children are excluded from these higher benefits. At the same time, the Act would dramatically reduce other previously bipartisan safety net programs that support low-income children, particularly SNAP.
The CTC is a tax credit for families with children. It was originally conceived as an anti-poverty program, though for much of its history most of the CTC’s benefits have gone to middle class or wealthier families. The CTC phases in with earnings and the credit is only partially refundable, meaning that if the credit exceeds a filer’s tax liability, families can receive a portion of the credit as a tax refund. Approximately 60 million children benefit from the current credit. In response to the COVID-19 recession, for one year the credit provided families with as much as $3,600 per child and allowed low-earnings families to get the full benefit, but that expired and the maximum returned to the pre-OBBBA maximum of $2,000. Because of the phase-in and other limitations on refundability, an estimated 17 million children in families with low incomes receive less than the full $2,000-per-child credit or no credit at all.
Under OBBBA, the maximum credit was raised to $2,200 per child and then indexed to inflation. Because the bill did not make any changes to the CTC’s refundability or phase-in with earnings, this change will not benefit any of the estimated 17 million children who were left out under pre-OBBBA law. Furthermore, the act’s increase in the standard tax deduction and other changes will increase the number of children whose families don’t get the full credit.
The OBBBA CTC expansion primarily benefits families with above average income. As this graph from the The Budget Lab shows, the bottom 40% receive little or no benefit.
There are many possible changes to broaden the CTC’s reach and help more children. (See Crandall-Hollick, Maag, & Jha 2025.):
Under current law, adoption expenses of up to $17,280 per child can be credited against income taxes. In practice, few families get the full credit because the credit is nonrefundable and few families have an income tax bill greater than this amount.
Under OBBBA2 up to $5,000 of qualified adoption expenses will be refundable, thereby increasing the available adoption credit for approximately 45,000 children per year.3
Congress could broaden the benefits of the adoption credit by reducing the total credit and increasing the refundable amount, e.g., reducing the maximum to $12,000 while increasing the refundable amount to $6,000.
Some observers, concerned about declining birthrates, have proposed a cash payment for newborns soon after birth. Although President Trump has expressed support for a $5,000 “baby bonus”, the administration made no specific proposal and none was included in any version of the OBBBA. (A baby bonus could be implemented via a change in the CTC, as described above.)
There are many federal safety net programs that provide cash or in-kind benefits to families based on having children and the number of children. The largest near-cash program, SNAP, will be cut back very substantially by OBBBA. An Urban Institute report estimated that the SNAP cuts would affect 3.3 million families with children and reduce their benefits by an average of $840 per year.
With multiple rationales, policymakers with varying perspectives have concluded that children and their families would benefit from starting life with a nest egg, a savings account to be created early in a child’s life, to be then held and used well in the future for education, homebuying, or other purposes. States, cities, counties, and nonprofits have started programs that both establish child savings accounts and provide a starter contribution to those accounts. According to the Congressional Research Service, over 100 such programs had been started by 2023, in addition to the education savings account programs operated by many states under Section 529 of the Internal Revenue Code.
These programs draw from work in the early 1990s by academic Michael Sherraden which proposed a national program of “Individual Development Accounts” for the poor. This led to local programs in many cities and some states. A similar approach using the term “baby bonds” was proposed by scholars in 2010 as a means to reduce racial gaps in wealth, and this proposal was adapted into the American Opportunity Accounts Act introduced by Senator Cory Booker (D-NJ) in 2018. Under those proposals every child would receive a grant at birth, with additional government grants to children in poorer families in later years. Some child investment programs, such as New York City’s RISE program also incorporate philanthropic gifts.
The approach became bipartisan this year when Senator Ted Cruz (R-TX) proposed that each newborn child receive a one-time $1,000 grant in an “Invest America Account.” Cruz’s rationale was less about reducing wealth disparities and more that such accounts would give children a stake in the future and an understanding of investment markets. In place of ongoing government contributions, he proposed that parents, employers, philanthropies, and others could contribute to the child accounts. The Cruz proposal was, with modifications, adopted in OBBBA.
Advocates of these accounts see several advantages. First, they note with some evidence that having a personal account early in life that can only be accessed later substantially increases a child’s and family’s interest in education and personal betterment. Some believe that these accounts will also improve financial literacy and understanding of the economy and investment.
Other advocates, noting that disparities in wealth are associated with differences in educational opportunities, attainment, and future income and that wide racial differences in wealth persist, believe these programs could reduce wealth disparities at the start of life. The original child savings programs focused on this rationale, with payments or participation incentives that favored the poor. There is research that finds higher wealth associated with better educational and health outcomes, as well as stronger protection against material hardship following disruptive events, suggesting that policies that facilitate wealth-building could have profound effects.
OBBBA permits4 the secretary of the Treasury and/or private financial institutions to offer “Trump accounts,” savings accounts for children under 18 that offer some limited tax benefits if invested and not used until age 18. Contributions to these accounts, limited to $5,000 per year from family members, would be taxed as ordinary income. In addition, there is a 10% penalty for withdrawals before age 59½, with certain exceptions for education, home buying, adoption, disaster relief, etc. Contributions are also permitted from employers, up to $2,500 per year, and as part of a general program from government or philanthropies supporting all children in an approved geographic area.
The act also creates a pilot program of $1,000 government grants for any child born in the years 2025-28 (with a Social Security number) if the parent or Treasury elects5 and if there is an account established for that child. Although the government funds to be provided are given only at birth and are generally much smaller than the CTC, if made universally available they will reach some poor families with children that the Child Tax Credit does not.
While both Republicans and Democrats have endorsed at least the outlines of child savings accounts and a universal starting grant, there are many potential supporters who have questioned the design of Trump Accounts as enacted by Congress. A comprehensive review of child savings accounts systems undertaken by the Aspen Institute’s Financial Security Program raised a series of challenges, only some of which were responded to by the Congress. The Aspen publication noted ominously that similar program in the U.K. had been regarded as a failure and had in effect “poisoned the well” so that other efforts were unlikely to be considered for many years. That may have been a warning for Trump accounts.
Making Trump Accounts and the $1,000 per newborn pilot program work will require:
Since the program has the president’s name on it, Treasury is likely to make every effort to help Trump Accounts succeed and be widely adopted and used. Some changes have already been suggested:
Unsurprisingly, there are differences of opinion whether additional resources should be devoted to immediate financial relief (using the CTC or a child grant) or instead to child savings accounts and wealth building for the longer term. There are advocates of both approaches and both have been shown to benefit children and families. However, there isn’t yet enough experience with child savings accounts to form judgments about the appropriate balance of resources between them.
Given the broad public support to help children and families with children, elected officials from both parties will claim their efforts do so. As the distinctly non-bipartisan experience with OBBBA shows, however, many programs fall short of the rhetoric: overall, OBBBA seems likely to harm as many families with children as it helps.
Future bipartisan efforts can and should do better, supporting all families with children, including those who are more in need.

“Value-based care” in UnitedHealth’s Optum division apparently means fewer doctors for fatter margins.
UnitedHealth Group announced last week that it plans to cut thousands of doctors from its network, a move CEO Stephen Hemsley said will increase profits for the country’s richest health care conglomerate.
UnitedHealth assembled a network of nearly 90,000 physicians across the country as it bought hundreds of physician practices, began managing the Medicaid program in many states and became the biggest Medicare Advantage company. It also owns one of the nation’s largest pharmacy benefit managers, Optum Rx.
Of those 90,000 doctors, the company says fewer than 10,000 are currently directly employed by UnitedHealth. The company has been gobbling up a broad range of medical facilities in recent years, buying or creating nearly 2,700 subsidiaries and gaining direct control or affiliation with 10% of doctors working in the U.S. in the process.
The announcement by Hemsley came during a third-quarter earnings call with investors last week, when UnitedHealth announced it made $4.3 billion in profit in the last three months by generating revenues of $113 billion.
Read more here on how they did that. Spoiler alert: It involves raising health care premiums and collecting billions more from the Medicare Trust Fund and seniors.
Hemsley said the company’s health care services division, Optum Health, needed to consolidate its physician rolls to improve its bottom line.
He passed questions about how that will be done to Optum’s CEO Patrick Conway, who said too many doctors in the network weren’t aligned with UnitedHealth’s business model, which he called “value-based care.”
“We are moving to employed or contractually dedicated physicians wherever possible,” Conway said.
Overseeing an empire that offers health insurance, pharmacy benefits and doctors who provide care and write prescriptions, UnitedHealth has become America’s third-richest company behind Walmart and Amazon. There are 29.9 million Americans enrolled in UnitedHealthcare’s commercial plans, 8.4 million in its Medicare Advantage plans and 7.5 million in state-run Medicaid programs.
In 2024, the company brought in more than $400 billion in revenue, according to its financial filings.
Americans’ health care premiums are expected to rise drastically in 2026 after climbing as much as 6% on average this year compared to 2024.
UnitedHealth’s decision to remove doctors from networks means that many of its patients will have to find new, in-network physicians unless they change their insurers.
UnitedHealth isn’t alone in taking steps to trim its medical expenses to boost its bottom line. Both CVS Health, which owns Aetna, the PBM CVS Caremark and more than 9,000 retail pharmacies, and Cigna, which owns the PBM Express Scripts, also told investors they are implementing plans to improve earnings next year.
CVS Health is just behind UnitedHealth at No. 5 on the country’s Fortune 500 list, bringing in nearly $373 billion in revenue last year. Cigna is 13th with $247 billion in revenue.



{kind=link}