The trope is currently abuzz in anti-vaccine circles, said Nicole Baldwin, MD, a pediatrician who has been a target of attacks by the anti-vaxxer community.
“It’s amazing, and sad, what people will believe,” Baldwin told MedPage Today.
Essentially, they believe that people who’ve had the vaccine can somehow shed the spike protein, which in turn can cause menstrual cycle irregularities, miscarriages, and sterility in other women just by being in close proximity.
“This is a new low, from the delusional wing of the anti-vaxx cult,” said Zubin Damania, MD, a.k.a. ZDoggMD, in a video he recently posted to bust vaccine shedding myths.
Damania said the misinformation originates from an earlier claim that syncytin, a protein involved in placental formation, bears some structural similarities to the spike protein, and therefore vaccination would interfere with women’s reproductive systems. Many a fact check has shown that vaccines don’t target the protein.
Once injected, the vaccines prompt cells to make the spike protein, but it’s usually cleared in 24 to 48 hours, leaving little opportunity for “shedding,” even if it could occur — which it can’t, Damania emphasized.
Another logical fallacy he pointed out: “Why, then, wouldn’t natural spike protein do the same thing? Wouldn’t you be more scared of natural coronavirus infection? Oh, but it’s ‘natural.'”
Damania noted that there are legitimate questions and research about whether the coronavirus itself and vaccines have an impact on women’s menstrual cycles. Since the beginning of the pandemic, women who’ve had COVID-19 reported changes to their menstrual cycle, and Damania said that researchers are assessing reports of changes to the menstrual cycle following vaccination.
Regarding the potential relationship to vaccination, “we don’t understand, first, if it’s true, and if it were true, what is the mechanism?” he said. “Anything that causes stress, inflammation, and an immune response may have an effect on the menstrual cycle. … Could it be that the vaccine causes a temporary change in menses? Sure, it’s possible, and it’s being looked at.”
Leila Centner, co-founder and CEO of Centner Academy, the Miami school that has banned vaccinated employees, told NBC News in a statement that “tens of thousands of women all over the world” have reported reproductive issues from being around someone who has been vaccinated.
Baldwin pointed out an Instagram video, now marked as misinformation, in which a nurse, Maureen McDonnell, RN, and a physician, Lawrence Palevsky, MD, discuss the effect of vaccines on women’s menstrual cycles.
“This isn’t just a trivial thing,” Damania said. “It’s quite harmful.”
One hesitates to elevate obviously bad arguments, even to point out how bad they are. This is a conundrum that comes up a lot these days, as members of the media measure the utility of reporting on bad faith, disingenuous or simply bizarre claims.
If someone were to insist, for example, that they were not going to get the coronavirus vaccine solely to spite the political left, should that claim be elevated? Can we simply point out how deranged it is to refuse a vaccine that will almost certainly end an international pandemic simply because people with whom you disagree think that maybe this is a good route to end that pandemic? If someone were to write such a thing at some attention-thirsty website, we certainly wouldn’t want to link to it, leaving our own readers having to figure out where it might be found should they choose to do so.
In this case, it’s worth elevating this argument (which, to be clear, is actually floating out there) to point out one of the myriad ways in which the effort to vaccinate as many adults as possible has become interlaced with partisan politics. As the weeks pass and demand for the vaccine has tapered off, the gap between Democratic and Republican interest in being vaccinated seems to be widening — meaning that the end to the pandemic is likely to move that much further into the future.
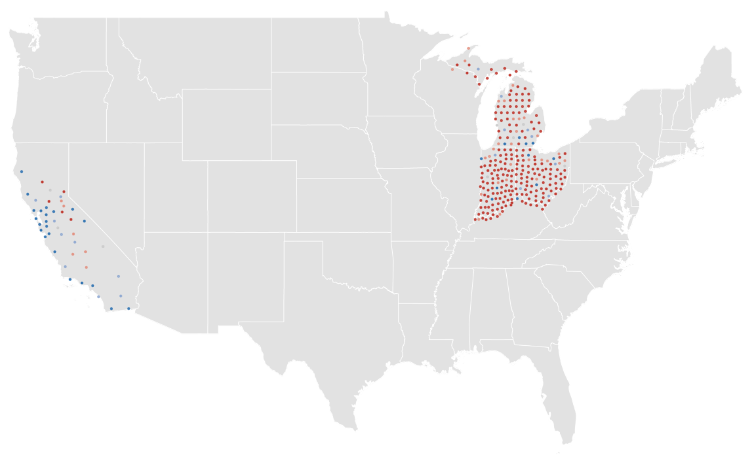
Consider, for example, the rate of completed vaccinations by county, according to data compiled by CovidActNow. You can see a slight correlation between how a county voted in 2020 — the horizontal axis — and the density of completed vaccinations, shown on the vertical. There’s a greater density of completed vaccinations on the left side of the graph than on the right.
If we shift to the percentage of the population that’s received even one dose of the vaccine, the effect is much more obvious.
This is a relatively recent development. At the beginning of the month, the density of the population that had received only one dose resulted in a graph that looked much like the current density of completed doses.
If we animate those two graphs, the effect is obvious. In the past few weeks, the density of first doses has increased much faster in more-Democratic counties.
If we group the results of the 2020 presidential contest into 20-point buckets, the pattern is again obvious.
It’s not a new observation that Republicans are less willing to get the vaccine; we’ve reported on it repeatedly. What’s relatively new is how that hesitance is showing up in the actual vaccination data.
A Post-ABC News poll released on Monday showed that this response to the vaccine holds even when considering age groups. We’ve known for a while that older Americans, who are more at risk from the virus, have been more likely to seek the vaccine. But even among seniors, Republicans are significantly more hesitant to receive the vaccine than are Democrats.
This is a particularly dangerous example of partisanship. People 65 or older have made up 14 percent of coronavirus infections, according to federal data, but 81 percent of deaths. That’s among those for whom ages are known, a subset (though a large majority) of overall cases. While about 1.8 percent of that overall group has died, the figure for those aged 65 and over is above 10 percent.
As vaccines have been rolled out across the country, you can see how more-heavily-blue counties have a higher density of vaccinations in many states.
This is not a universal truth, of course. Some heavily Republican counties have above-average vaccination rates. (About 40 percent of counties that preferred former president Donald Trump last year are above the average in the CovidActNow data. The rate among Democratic counties is closer to 80 percent.) But it is the case that there is a correlation between how a county voted and how many of its residents have been vaccinated. It is also the case that the gap between red and blue counties is widening.
Given all of that, it probably makes sense to point out that an argument against vaccines based on nothing more than “lol libs will hate this” is an embarrassing argument to make.
The pandemic won’t end for anyone until it ends for everyone. That sentiment has been repeated so many times, by so many people, it’s easy to forget it’s not just a cliche—particularly if you live in one of the wealthy countries, like the U.S. and Israel, that has made significant moves toward what feels like an end to the COVID-19 era.
Israel, for example, has fully vaccinated more than half of its population and about 90% of its adults 50 and older are now immune to the virus—enough that the country is “busting loose” and “partying like it’s 2019,” as the Washington Post put it last week. The U.S. is a bit further behind, with nearly 30% of its population fully vaccinated, but the possibility of a post-pandemic reality is already coming into focus. While daily case counts remain high, they are far lower than they were even a few months ago—about 32,000 diagnoses were reported on April 25, compared to daily tallies well above 250,000 in January. Deaths have also trended downward for most of 2021. The U.S. Centers for Disease Control and Prevention has relaxed its guidance on travel and indoor gatherings, and some states have repealed mask mandates and other disease precautions.
But while people in certain affluent countries celebrate a return to vacations and parties, COVID-19 remains a dire threat in many nations around the world—nowhere more so than India. For five days in a row, the country has set and reset the global record for new cases in a single day, tallying about 353,000 on April 26.
By official counts, about 2,000 people in India are dying from COVID-19 every day as hospitals grow overtaxed and oxygen supplies run short. Experts say the true toll is likely even higher than that. People are dying as they desperately seek treatment, and crematoriums nationwide are overwhelmed.
It can be difficult to grapple with that devastating reality when people in countries like the U.S. are reuniting with loved ones and cautiously emerging from lockdown. How can both scenarios be happening at once? The answer, as it often has during the pandemic, lies in disparity. As of April 26, 83% of vaccinations worldwide had been given in high- and upper-middle-income countries, according to a New York Times data analysis. In the developing world, many countries are preparing for the reality that it could take until 2022 or even 2023 to reach vaccination levels already achieved by richer countries today. Even in India, one of the world’s leading vaccine manufacturers, fewer than 10% of people have gotten a vaccine—a cruel irony, as people in India die in the streets while those thousands of miles away celebrate receiving their second doses.
To truly defeat COVID-19, we must reckon with that cognitive dissonance, says Dr. Rahel Nardos, who is originally from Ethiopia and now works in the University of Minnesota’s Center for Global Health and Social Responsibility. As an immigrant and global health physician who lives in the U.S., Nardos says she inhabits two worlds: one in which the U.S. may feasibly vaccinate at least 70% of its population this year, and another in which many countries struggle to inoculate even 20% of their residents in the same time frame.
“It’s a huge disparity,” Nardos says. “We need to get out of our silos and start talking to each other and hearing each other.”
That’s imperative, first and foremost because it could save lives. More than 13,000 people around the world died from COVID-19 on April 24. Remaining vigilant about disease prevention and monitoring, and working to distribute vaccines in countries that desperately need them to fight back COVID-19 surges, could help prevent more deaths in the future. That’s especially critical for developing countries, many of which are so overwhelmed by COVID-19 that nearly all other aspects of health care have suffered. “We may be looking at five, 10 years before they can get back to their baseline, which wasn’t that great to begin with,” Nardos says.
There’s also a global health argument for distributing vaccines more equitably.Infectious diseases do not respect borders. If even one country remains vulnerable to COVID-19, that could allow the virus to keep spreading and mutating, potentially evolving to such a point that it could infect people who are vaccinated against original strains of the disease. Already, vaccine makers are exploring the possibility of booster shots to add extra protection against the more transmissible variants currently circulating in various parts of the world.
We aren’t at that point yet; currently authorized vaccines appear to hold up well against these variants. But if the virus keeps spreading for years in some areas, there’s no telling what will happen, says Jonna Mazet, an epidemiologist and emerging infectious disease expert at the University of California, Davis.
“Evolution of those new strains could go into multiple directions. They may evolve to cause more severe or less severe disease. Some of the variants [could be] more concerning for young people,” Mazet says. “The whole dynamics of the disease change.”
And if the virus is mutating somewhere, chances are good it will eventually keep spreading in multiple areas, Mazet says. “Unless or until we have a major shift, we are still going to have large parts of every country that have a susceptible population,” she says. “The virus is going to find a way.”
The only way to stop a virus from mutating is to stop giving it new hosts, and vaccines help provide that protection. COVAX—a joint initiative of the World Health Organization; Gavi, the Vaccine Alliance; the Coalition for Epidemic Preparedness Innovations; and UNICEF—was meant to ensure that people in low-income countries could get vaccinated at the same time as people in wealthier ones. COVAX is providing free vaccines to middle- and low-income countries, using funds gained through purchase agreements and donations from richer countries. But supply and funding shortages have made it difficult for the initiative to distribute vaccines as quickly as it intended to. Many of the doses it planned to disseminate were supposed to have come from the Serum Institute of India, which delayed exporting doses in March and April as India focused on domestic vaccine rollout to combat its COVID-19 surge at home.
In the meanwhile, many poorer countries have been unable to vaccinate anywhere close to as many people as would be required to reach herd immunity. That will almost surely improve as new vaccines are authorized for use by regulators around the world, and as manufacturers scale up production, but those moves may be months away.
COVAX is also developing a mechanism through which developed countries could donate vaccine doses they don’t need. Some wealthy countries, including the U.S. and Canada, have contracts to purchase more than enough doses to vaccinate their entire populations, and have signaled their intent to eventually donate unneeded supplies—but timing is everything. That is, these countries will likely only donate once they are sure their own populations have been vaccinated at a level that ensures herd immunity.
On April 25, the Biden Administration said the U.S. would provide India with raw supplies for making AstraZeneca’s vaccine, as well as COVID-19 tests and treatments, ventilators, personal protective equipment, and funding. That’s a significant shift, since the export of raw vaccine materials was previously banned, but it still doesn’t provide India with ready-to-go vaccines. That step may be next, though. The U.S. will export as many as 60 million doses of AstraZeneca’s vaccine once the shot clears federal safety reviews, the Associated Press reports.
Gian Gandhi, UNICEF’s COVAX coordinator for supply, says he fears many wealthy countries’ vaccine donations may not come until late in 2021, just when global supply is expected to ramp up. That may cause a bottleneck effect: all doses may come in at once, rather than at a slow-but-steady pace that allows countries with smaller health care networks to distribute them. “We need doses now, when we’re not able to access them via other means,” Gandhi says.
The global situation is also critical now. Worldwide, more than 5.2 million cases and 83,000 deaths were reported during the week leading up to April 18. Indian hospitals are so overrun, crowds have formed outside their doors and desperate families are trying to source their own oxygen. Hospitals in Brazil are reportedly running out of sedatives. Iran last week broke daily case count records three days in a row. Countries across Europe remain under various forms of lockdown. Vaccines won’t change those realities immediately—but without them, the global community stands little chance of containing COVID-19 worldwide.
Now that we’ve entered a new phase of the vaccine rollout, with supply beginning to outstrip demand and all adults eligible to get vaccinated, we’re hearing from a number of health systems that their strategy is shifting from a centralized, scheduled approach to a more distributed, access-driven model. They’re recognizing that, in order to get the vaccine to harder-to-reach populations, and to convince reticent individuals to get vaccinated, they’ll need to lean more heavily on walk-in clinics, community settings, and yes—primary care physicians.
For some time, the primary care community has been complaining they’ve been overlooked in the national vaccination strategy, with health systems, pharmacy chains, and mass vaccination sites getting the lion’s share of doses. But now that we’re moving beyond the “if you build it, they will come” phase, and into the “please come get a shot” phase, we’ll need to lean much more heavily on primary care doctors, and the trusted relationships they have with their patients.
As one chief clinical officer told us this week, that means not just solving the logistical challenges of distributing vaccines to physician offices (which would be greatly aided by single-dose vials of vaccine, among other things), but planning for patient outreach. Simply advertising vaccine availability won’t suffice—now the playbook will have to include reaching out to patients to encourage them to sign up.
There will be workflow challenges as well, particularly while we await those single-dose shots—primary care clinics will likely need to schedule blocks of appointments, setting aside specific times of day or days of the week for vaccinations. The more distributed the vaccine rollout, the more operationally complex it will become. Health systems won’t be able to “get out of the vaccine business”, as one health system executive told us, because many have spent the past decade or more buying up primary care practices and rolling out urgent care locations. Now those assets must be enlisted in the service of vaccination rollout.
Health systems will have to orchestrate a “pull” strategy for vaccines, rather than the vaccination “push” they’ve been conducting for the past several months. To put it in military terms,the vaccination “air war” is over—now it’s time for what’s likely to be a protracted and difficult “ground campaign”.