Cartoon – Its Curiosity


Here are three insightful and thought-provoking facts that most
people aren’t aware of and the potential implications of these
statistics / trends on healthcare stakeholders.
Fact 1: The third leading cause of death in the U.S. is due to medical error
According to a study by Johns Hopkins, more than 250,000 people in the United States
die every year because of medical mistakes, making it the third leading cause of death
after heart disease and cancer. Some studies show the death rate as high as 440,000
deaths per year. To put that in perspective, approximately 350,000 people died from
COVID-19 in 2020, which, similar to medical error, was no fault of their own. A medical
error death “is caused by inadequately skilled staff, error in judgment or care, a system
defect, or a preventable adverse effect. This includes computer breakdowns, mix-ups
with the doses or types of medications administered to patients and surgical
complications that go undiagnosed.”
Fact 2: Medicare’s trustees report that the Part A trust fund will be insolvent by
2024
Medicare – Part A, which pays for hospital bills, is funded mainly through the payroll
taxes. According to the report, without changes to expected spending or trust fund
revenue, the fund will run dry in 2024 and have sufficient funds only to meet 90% of its
obligations. This is the second time insolvency has been predicted within five years.
Without any changes the shortfall would have to be covered by one or more of the
following potential options: (i) add new revenue, which equates to increasing the payroll
tax rate, (ii) raise the share of costs shouldered by enrollees, (iii) cut benefits, or (iv)
reduce payments to healthcare providers.
Fact 3: The last decade was the lowest population growth rate ever recorded
U.S. Population Growth for Decades
The U.S. population growth of 6.6% between 2010 and 2020 is lower than in any previous decade, including the Great
Depression years of the 1930s. It is also roughly half the growth rate of the 1990s, a time of rising immigration and
millennial-generation births.
The 2010s decade was one of fewer births, more deaths, and uneven immigration, but the primary cause of this dramatic decline is highly related to falling U.S. fertility rates.
The U.S. fertility rate has been falling steadily and as of recently stood at 1.7 births per woman (ratio of number of births in a year to total population of women between the ages of 15 and 50), the lowest level on record. Some experts hope that the decline is “temporary” and that Millennials are postponing family formation as they are burdened with debt and struggle with launching careers and establishing households. However, there is no clear sign of an any uptick, and, to make matters worse, net immigration has also declined since 2008.
The data is clear that the aging of America is inevitable, and the prospects for higher fertility rates look dim. Even if the
fertility rate were to surge today, it would not have an appreciable effect on the ratio of workers to retirees or the growth rate in employment for another twenty to twenty-five years (the time it takes to turn an infant into a fully productive adult).
Conclusion
What does the third leading cause of death in the U.S., Medicare Part A near-term insolvency projections, and declining population growth have in common? All of these alarming realities can be solved through value-based care. Value-based care is an alternative system for how providers are rewarded for care and incentivizes the quality of care they give to people, rather than the volume of services. Another way to put it, providers and health systems will not be paid for medical error deaths and instead be rewarded for quality of patient care and outcomes. Because of this alternative payment system, healthcare stakeholders will be forced to invest in technology, tools, and resources so that healthcare providers and workers can make better quality decisions. Technology will help alleviate staff shortages, improve medical treatment accuracies, increase productivity, and enable organizations to do more with less.
The alarming medical error rate is proof that our traditional healthcare system and payment models are flawed, and that the need to move into a value-based care world is a must. Imagine if the third leading cause of death in the U.S. were caused by commercial airline pilot errors. The industry would crumble overnight. The healthcare sector and our standards for care should be no different.
To add fuel to the fire, we have an impending insolvency issue with Medicare Part A funding combined with population growth trends that will result in a much wider gap between the working and an aging population in need of care. The working population decline will also have a downstream impact of less working providers / medical staff to take care of patients, as well as fewer contributing taxpayers. These trends, if left as is, will guarantee a very imbalanced, underfunded and extremely lopsided healthcare ecosystem.
Healthcare stakeholders need to think about reorienting provider compensation to encourage value over volume, invest in much needed tools, such as strong data analytics and reporting, so that the right decisions and diagnoses are made at the right time. Lastly, we need to shift care away from costly and error-prone hospitals and create innovative care models that deliver better care in a cost-effective manner. In essence, we need to do more with less. The aging and demographic shift of America is inevitable; however, the fiscal, economic, and potential healthcare catastrophe is not if we prepare, adapt, and transition to a value-based care world today

Dollar General hired its first CMO and plans to become a destination for affordable healthcare offerings.
The retail giant will bring an increased assortment of medical, dental and health aids to its shelves as part of its first major jump into the healthcare industry, according to a July 7 news release.
Three things to know:
https://www.cbsnews.com/news/blood-donation-shortage-us-2021/

Blood centers in some U.S. cities are down to a one-day supply, forcing hospitals to postpone surgeries. The blood shortage is yet another fallout from the pandemic, experts say.
OneBlood, the Southeast’s largest blood center, is scrambling to manage the blood shortage crisis.
“It’s a 24/7 operation,” said OneBlood’s Susan Forbes. “The donors are not in the traditional locations anymore. We lost large corporations, religious organizations, movie theater drives, festivals that were taking place ended.”
Before COVID-19 shutdowns, schools accounted for 25% of collected blood. Now, demand for blood products is up 10% nationwide.
Some hospitals have had to delay scheduled surgeries. At NYU Langone Health in New York City, surgeon-in-chief Dr. Paresh Shah said they came close to doing the same.
“There’s this huge backlog of operations that really needed to get done,” Shah said. “We were down to such a low inventory of blood that if we had one major transfusion event, we would have been depleted completely.”
He said the lack of blood can mean life or death in trauma situations.
Eleven-year-old Iggy Friday was diagnosed with Leukemia this winter and has needed more than 30 transfusions during chemotherapy. His recent platelet transfusion was delayed because of the shortage — luckily for just a few hours.
“I did think about the people who needed it now and stuff. So that’s why I was fine with waiting,” he said. “It helps a lot of people and can save a lot of lives.”
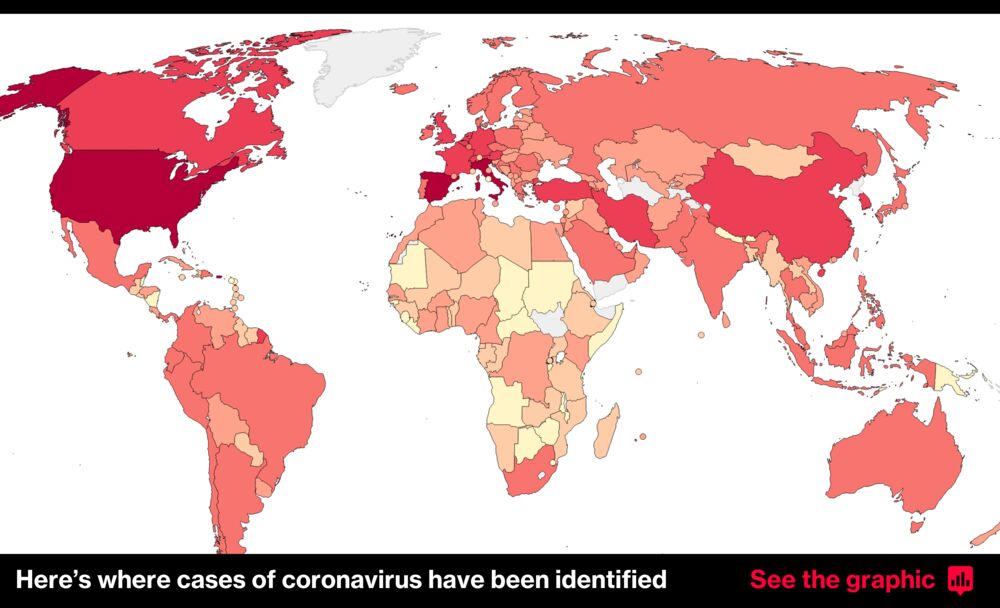
The coronavirus has killed nearly 4 million people since it first emerged in Wuhan, China, in 2019, according to data compiled by Johns Hopkins University.
New confirmed cases of covid-19, the disease caused by the virus, remain high, and the world struggles with unequal vaccine rollouts and new threats posed by fast-spreading variants.
“The pandemic is a long way far from over,” World Health Organization Director General Tedros Adhanom Ghebreyesus warned in May. “It will not be over anywhere until it’s over everywhere.”
Some countries have already found that the spread of the virus is outpacing their vaccination plans, especially in the face of proliferating variants. In India, new daily cases topped 400,000 in early May — a global record but probably an undercount.
China now leads the world in the number of vaccine doses given out, though some other nations have vaccinated far more of their population. The vaccines were developed and rolled out at record speed, and studies show most have impressive efficacy.
More than a billion doses have been administered around the world, far more than the number of confirmed cases of the coronavirus since the start of the pandemic — though a large number of cases were likely never recorded, experts caution.
But the vaccine rollout has been persistently unequal, with problems with global supply and pockets of opposition in many nations. Covax, a program to distribute vaccines fairly backed by the World Health Organization, only belatedly began distributing doses to low-income nations.
“I can’t say it’s surprising,” said Thomas J. Bollyky, a senior fellow at the Council on Foreign Relations. “In every previous pandemic where we have our global health crisis, where there has been limited supplies of medical intervention, wealthy nations have hoarded.”
The United States, which continues to have the highest cumulative number of confirmed cases and deaths globally. More than 590,000 deaths from covid-19 have been recorded across the country.
Though cases dipped after January, a new wave began only a few months later, prompting President Biden to urge governors to reinstate mask mandates and other virus-related restrictions. “This is deadly serious,” Biden said in March.
Behind the United States, India, Brazil, France and Turkey have the largest number of cases.
India’s record-setting surge this spring meant the country accounted for about 1 in 3 of all new confirmed cases. The spike, which has been blamed on complacency and the lifting of restrictions, along with the spread of variants, has seen the country’s health-care system overwhelmed amid widespread oxygen shortages.
Even after the spike in new cases subsided in mid-May, India still set records for the number of new daily deaths with more than 4,500 deaths from covid-19 reported in a single 24-hour period.
In India, as in Britain and Brazil before it, some of the spread of the virus has been blamed on fast-spreading variants rampant in the country.
The variant widespread in India, known by the name B.1.617.2, has spread far beyond its borders. In May, British officials warned that it would likely become dominant across Britain unless more was done to control its spread.
Sharon Peacock, director of the U.K.’s Covid-19 Genomics Consortium, told reporters that a fast-spreading variant such as B.1.617.2 had “a biological passport for international travel and global spread” — making its spread difficult, if not impossible, to fully contain.
Some countries have seen success at controlling the virus.
In New Zealand, which closed its borders and ordered people to stay home as a first wave hit in the spring of 2020, confirmed infections went down to zero for a time. Taiwan and Singapore have kept their outbreaks far smaller than those in other parts of the world, which some experts attribute to their early responses and sophisticated tracking and tracing.
China, the early epicenter of the crisis, has seen much of daily life return to normal. In the early months of the outbreak, it reported more cases than any other country. Its tally of new infections peaked in mid-February of 2020 and approached zero by mid-March, although questions surround the accuracy of its data.
Wuhan, the virus’s initial epicenter, ground to a standstill in January 2020 as the coronavirus spiraled out of control. But after months without a confirmed case of domestic transmission, about 1.4 million children in the city returned to classrooms at the start of September, and crowded events have resumed.
Countries that have successfully rolled out vaccines are also seeing important gains. Britain, one of the hardest-hit countries in terms of cases and deaths, has excelled in the distribution of coronavirus vaccines. It was the first country to roll out a fully tested vaccine to the general public in December, when it began distributing the vaccine developed by Pfizer and Moderna.
Data released by Public Health England in March suggested that vaccinations had saved over 6,000 lives among people over 70, if not more.
Israel, which has seen several waves of the virus, had raced ahead of other nations and given the first doses of Pfizer’s two-dose vaccine to more than a third of its population by the end of January. Data from Israel indicated that the Pfizer vaccine was around 94 percent effective at stopping asymptomatic infection.
Early signs from the country suggest that the large scale of vaccinations has had an impact on the spread of the virus.
But global health experts have cautioned that despite the success of vaccines, the virus remains a potent threat and returning to normal life too early could ultimately extend the length of the pandemic and lead to fresh new cases.
Though wealthy countries have taken some steps to ensure vaccines are shared around the world, such as by donating through Covax or supporting waivers on intellectual property such as the Biden administration has done, experts say they are worried by the ongoing level of spread.
“Sadly, unless we act now, we face a situation in which rich countries vaccinate the majority of their people and open their economies, while the virus continues to cause deep suffering by circling and mutating in the poorest countries,” United Nations Secretary General António Guterres said at a meeting of the World Health Assembly on May 24.

If you were anything like my family over the July 4 holiday, there were bowls of potato salad, casseroles of baked beans and platters of hotdogs, hamburgers and chicken all pulled from the grill and served family-style. For a lot of us, it was the first time seeing a wide net of our family in more than a year and we took advantage of ditching the masks, probably wrongly assuming our circles were vaccinated at higher levels than they were and maybe even handing kids lighters for sparklers they shouldn’t be wielding.
Our increasing return to normal makes it easy to believe the pandemic is almost over. Sure, we still had to wear masks on the flights, trains and buses. Grocery markets and big-box stores in some communities still asked that we wear them, too. The staff at Nationals Park here in D.C. and Progressive Field in Cleveland wore theirs as I visited both for MLB games. But the worst of the pandemic feels behind us here in the U.S., as vaccinations are climbing, deaths and new cases are sinking and headlines seem to be shifting to more run-of-the-mill topics like tropical storms.
A new and unusually long report from Congress’ independent think-tank is a stark warning to the U.S. government that even COVID-19 seems over, it actually isn’t, particularly when it comes to Americans’ well being. Released on Friday, the wonks at the Congressional Research Service (CRS) urged officials going into the long holiday weekend to remember amid the celebrations that we still don’t know the final toll of the pandemic, especially when it comes to long-term consequences for behavioral and mental health. Its notes about substance-abuse challenges are particularly worrying, given that lawmakers cannot ignore the already troubling fight against opioids.
Anecdotally, we know the last 18-or-so-months have taken a toll on our friends, colleagues and neighbors. Those of us lucky enough to have been allowed to work from home adapted in fits and starts. My colleagues with children or dependents were stretched to the points of breaking, but most have made it to the other side. Those in complete isolation actually came to look forward to Zoom meetings and telemedicine appointments. And tech-slow people like my grandmother probably wouldn’t have made it through without the good folks at the local public library loading her loans into the trunk through a touch-free lending system.
But you cannot make public policy on anecdotes alone, which is why the CRS report offers a roadmap for lawmakers. Noting upfront that the data is still coming in and comparisons so quickly after—and during, really—a so-recent period are imprecise, there are still warning signs that America has not healed the way we’d like to believe. The share of Americans suffering simultaneously from depression and anxiety grew five-fold, year-over-year, in just the first three-months of the pandemic-mandated lockdown, from April to June 2020, when the death toll still hovered around 120,000. Fatal overdoses grew 11% between March and May last year, and non-fatal overdoses rose 19% during that same short window. In the three months that followed, there were almost equal levels of depression or anxiety among households that had lost jobs and those that had not. No one was spared, but the hit came hardest for less-educated, essential and lower-paid workers.
Why is this Washington’s problem? An estimated 10% to 20% of Americans who needed mental-health services during the pandemic received no treatment. Another survey cited in the report estimates that up to a quarter of adults with depression or anxiety went untreated. As many as 27,000 Americans who survived COVID-19 may end up dead over the next decade as a result of behavioral health-related challenges, and that number may ultimately reach more than 154,000. At the moment, federal law does not require mental health services to be treated on par with treatments for physical health. Not Medicare. Not CHIP. Not even fancy private insurance plans.
There were, believe it or not, a few upsides to the COVID-19 pandemic that the CRS report notes. Under emergency powers granted in one of the relief bills, the Department of Health and Human Services waived the in-person requirement for some treatments, including mental health and substance abuse counseling. For now doctors can be paid for that phone call consultation rather than requiring patients to make a brick-and-mortar visit to qualify for Medicare and Medicaid money. The Department of Veterans Affairs allowed taxpayer dollars to help with mental health services via tech platforms, too. In all, billions of dollars were included in the raft of COVID-19 stimulus plans to shore up mental health and substance abuse programs.
But those were the bright spots. Not all of Washington’s urgent changes were for the better. The Drug Enforcement Agency allowed doctors to prescribe medicine without a physical appointment, Health and Human Services’ civil rights unit turned a lot of blind eyes to patients’ privacy rights as public health data seemed ubiquitous, and the Small Business Administration shoved piles of cash out the door to health clinics and larger rafts of money to hospitals with minimal upfront scrutiny.
So as Washington turns slowly toward the post-pandemic policies of this country, lawmakers have plenty to consider, especially if it wants to return America to its Before Times footing. As much as it may feel like the United States is rounding a corner—and it’s tough not to when you see big crowds gathering maskless for fireworks and parades—the reality is this: there’s still a lot of trauma under the surface that is all too easy to miss unless D.C. is looking for it.