Coronavirus cases reported in the United States passed 11 million on Sunday, as the nation shatters records for hospitalizations and daily new infections and as leaders turn to new, painful restrictions to stem the pandemic’s long-predicted surge.
The milestone came one week after the country hit 10 million cases, a testament to just how rapidly the virus is spreading — the first 1 million cases took more than three months. This new wave has increased covid-19 hospitalizations past the peaks seen in April and July, straining health-care systems and pushing some reluctant Republican governors to enact statewide mask mandates for the first time.
Other states are reenacting stay-at-home orders and store closures. Michigan Gov. Gretchen Whitmer (D) on Sunday announced sweeping new limits on gatherings for three-weeks — including a ban on indoor dining at restaurants and bars, and a halt to in-person classes at high schools and colleges. Washington Gov. Jay Inslee (D) also laid out a slew of new rules, which prohibit indoor social gatherings with people outside one’s household and indoor service at restaurants, bars and more.
“As hard as those first months were for our state, these next few are going to be even harder,” Whitmer said at a news conference, as health experts fear that winter weather driving people indoors will accelerate the crisis.
Inslee acknowledged that slowing the virus would come at a steep price for struggling businesses, even as the state works to distribute millions more in aid. He and Whitmer both appealed to the federal government to step in with more help. Congress remains deadlocked on a stimulus package, and President Trump — still denying his election loss — has largely tuned out the pandemic’s surge; his refusal to concede is also stalling the transition to a new administration, including the formal transfer of information on the nation’s pandemic response.
Whitmer said that Trump has “an opportunity to meet the needs of the people of this country” and emphasized the importance of his final months in office. Inslee was already looking ahead to the administration of President-elect Joe Biden.
“All of us who feel, as I do, the pain of the small-business people ought to be pounding the doors of the Congress and the new president, who I’m glad we’re going to have, to really get this job done,” Inslee said.
Washington’s restrictions are not as tough as its stay-at-home order issued in March but extend into nearly every aspect of daily life. Wedding and funeral receptions are forbidden. Religious services and in-store retail are forced to operate at reduced capacity. Even outdoor social gatherings must be kept to a maximum of five people from outside one’s household.
Inslee and other leaders in the state emphasized the need to intervene early amid spiraling statistics, even as Washington posts some of the lowest numbers for new coronavirus infections in the country. The number of hospital patients with covid-19 recently rose about 40 percent in a week, officials said, and Seattle’s mayor said that nearly a fifth of the city’s cases have come just in the past two weeks.
Clint Wallace, an ICU nurse in Spokane, joined Inslee at Sunday’s news conference to plead with residents for their help. He called the ICU “as busy as I’ve seen it.”
“We are exhausted,” Wallace said of health-care workers around the state.
State and local officials nationwide are reinstating restrictions to fight the virus. New Mexico and Oregon on Friday ordered extensive new statewide shutdowns, while the Navajo Nation — devastated early on by the virus — reissued its stay-at-home order for at least three weeks. The Navajo Nation said cases threaten to swamp the health system on the southwestern reservation without immediate action.
North Dakota Gov. Doug Burgum (R) on Friday issued a statewide mask mandate and new capacity limits on businesses, less than a week after Utah Gov. Gary R. Herbert (R) announced a similar mask order in the face of overwhelmed hospitals warning that they might have to ration care.
“Our situation has changed, and we must change with it,” Burgum said in a late-night video message.
But state rules are just one piece of the puzzle, and some leaders are looking to Congress and the incoming president to take stronger action.
Ron Klain, Joe Biden’s incoming chief of staff, said Sunday it’s critical for the president-elect’s transition team to start working with Trump administration officials to ensure “nothing drops in this change of power” that could imperil the distribution of a potential coronavirus vaccine.
“Joe Biden is going to become president of the United States in the midst of an ongoing crisis. That has to be a seamless transition,” Klain said on NBC News’s “Meet the Press.”
President Trump’s White House is blocking the administration from formally cooperating with Biden, forcing the president-elect’s transition team to continue preparations with recently departed government officials and other experts. That means Biden’s team has not heard from Trump’s about vaccine development and other work to combat the pandemic.
A health expert on Biden’s covid-19 advisory board said there’s “a lot of information that needs to be transmitted. It can’t wait until the last minute.”
It is in the nation’s interest that the transition team get the threat assessments that the team knows about, understand the vaccine distribution plans, need to know where the stockpiles are, what the status is of masks and gloves,” said Atul Gawande, a surgeon at Brigham and Women’s Hospital and a professor at Harvard Medical School, on ABC News’s “This Week.”
Anthony S. Fauci, head of the National Institute of Allergy and Infectious Diseases, compared the process Sunday to “passing a baton in a race.”
“I’ve been through multiple transitions now, having served six presidents for 36 years, and it’s very clear that transition process that we go through … is really important in a smooth handing over of the information,” Fauci said on CNN’s “State of the Union.”
“Of course it would be better if we could start working with them,” he added when asked whether working with Biden’s team would serve the public interest.
On “Meet the Press,” Klain said there is “not that much Joe Biden can do right now to change things,” because he is not yet president.
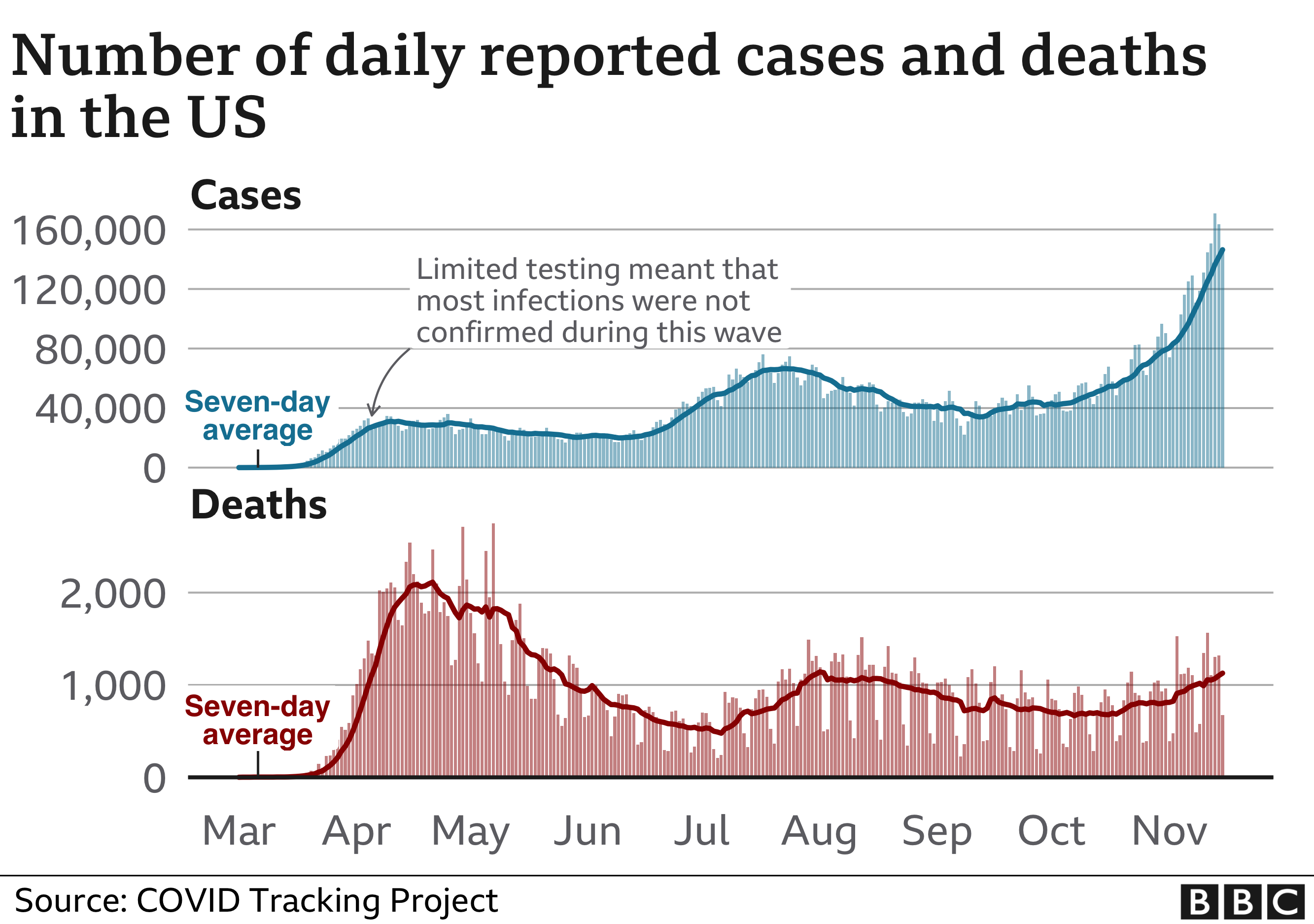
“Right now we have a crisis that’s getting worse,” Klain said. “We had never had a day with 100,000 cases in a single day until last week. By next week, we may see 200,000 cases in a single day.”
On the morning of November 7, major news networks starting with CNN called the presidential election for Joe Biden. Although the election has yet to be officially certified, Biden and Vice President-elect Kamala Harris have wasted no time preparing their response to the rapidly worsening coronavirus pandemic.
Over the past week, the US has averaged more than 150,000 new COVID-19 cases per day, an increase of 81% from the average on November 1. The US had a record 181,200 new reported cases on November 13. Over 11 million Americans have been infected, and the nation is nearing a grim milestone of 250,000 deaths. Experts warn that the worst is yet to come. As temperatures drop and family-centric holidays approach, people are likely to spend more time socializing indoors with non-household members, increasing the risk for COVID-19 transmission.
Mitigating the spread of the coronavirus and preventing more deaths are top priorities for the incoming Biden-Harris administration. Biden’s campaign team published a seven-point plan to beat COVID-19, and on November 9, the Biden-Harris transition team named a COVID-19 Advisory Council tasked with guiding the federal response to the pandemic immediately after the inauguration.
The council “will be consulting with state and local officials to gauge public-health steps needed to bring the virus under control,” Evan Halper and Noam Levey reported in the Los Angeles Times. “The board will also focus on racial and ethnic disparities in how, where, and how quickly the virus is spreading.”
Innovative Plan: Tell the Truth
The Biden-Harris plan sets a new tone for the nation’s coronavirus response, using federal powers and leadership to centralize the acquisition and distribution of personal protective equipment (PPE), along with the coordination of testing and contact tracing, instead of leaving those vital resources to be led in 50 different ways by state governors. It emphasizes evidence-based guidance and empowers public health officials and scientists to guide and revise the nation’s reopening strategy as the pandemic evolves.
“You’ll immediately see a change of tone, a change in communication,” Ezekiel Emanuel, MD, PhD, the vice provost for global initiatives at the University of Pennsylvania, told Politico.“This is the stuff of real leadership: telling the truth, modeling the right behaviors like wearing a mask, only having small crowds, putting the scientists out there.”
The first priority in the plan is to ensure that all Americans have access to regular, reliable, and free coronavirus testing. Rapid testing is vital for identifying, isolating, and treating new cases of COVID-19, but the US has been crippled by continuing test shortages and long lag times before results are reported. Biden plans to double the number of drive-through testing sites while scaling up next-generation solutions like home tests.
Contact tracing goes hand-in-hand with testing in the public health response to COVID-19, and the plan would establish a US Public Health Job Corps to train and mobilize 100,000 Americans to perform culturally competent contact tracing in communities most affected by COVID-19.
The second priority is to fix the nation’s PPE problems. N95 masks, gloves, gowns, and other PPE used by health care staff are still in short supply. AARP reported that one in four nursing homes ran short of PPE between August 24 and September 20. (Nursing homes continue to be a hot spot for coronavirus transmission.) Biden would use the Defense Production Act to increase production of PPE and distribute the supply to states instead of leaving states to fend for themselves.
For the third priority, Biden would tap the nation’s wealth of science experts to provide clear public guidance on how communities should navigate the pandemic. The US Centers for Disease Control and Prevention (CDC) would lead this effort, with an emphasis on helping communities determine when it is safe to reopen schools and various types of businesses.
Navigating Hurdles to Safe, Effective, Accepted Vaccine
Although the pharmaceutical company Pfizer announced on November 9 that its coronavirus vaccine trial showed positive early results, the road to vaccinating all Americans is tortuous. Pfizer still needs to seek emergency use authorization from the Food and Drug Administration (FDA) and ramp up vaccine production to meet the global need. In the meantime, Biden plans to invest $25 billion in a vaccine manufacturing and distribution plan that ensures every American can get vaccinated for free. This fourth priority would make the vaccine accessible to all people and communities regardless of income or any other factor.
The fifth priority is to protect Americans who are at high risk of getting seriously ill or dying from COVID-19. This includes people over 65, nursing home residents, and people living in neighborhoods with higher rates of COVID-19. Biden would establish a COVID-19 Racial and Ethnic Disparities Task Force (PDF) to report on disparities in COVID-19 infection, hospitalization, and death rates, as well as to provide recommendations to Congress and the Federal Emergency Management Agency on how best to distribute resources and relief funds to combat these disparities. The plan also calls for strengthening the Affordable Care Act to ensure that during the pandemic, Americans have health insurance coverage.
During the presidential campaign, Biden called for a national mask mandate based on the growing body of evidence that mask-wearing can considerably reduce the transmission of respiratory viruses like the one that causes COVID-19. Biden plans to coordinate with governors and mayors to convince Americans to wear a mask when they are around people outside their household. Currently, 34 states and the District of Columbia mandate face masks in public, but there is no nationwide requirement.
Finally, the plan takes the long view on pandemic threats by rebuilding and reinvesting in defenses that will help the world predict and prevent future pandemics. The Biden administration has declared that the US will rejoin the World Health Organization, restore the White House National Security Council Directorate for Global Health Security and Biodefense, which was eliminated by the Trump administration in 2018, and shore up CDC’s global corps of disease detectives.
Public Health Experts at the Helm
The newly announced COVID-19 Advisory Council is a who’s who of public health experts, former government officials, and doctors, including several from California. The panel currently comprises 13 members, but Biden has said it may be expanded.
The three cochairs of the advisory board are former surgeon general Vivek Murthy, MD; former FDA commissioner David Kessler, MD, a UCSF professor of pediatrics, and of epidemiology and biostatistics; and Marcella Nunez-Smith, MD, MPH, an associate professor of internal medicine, public health, and management at Yale University whose research focuses on health disparities.
The other members appointed so far include:
Luciana Borio, MD, vice president at the venture capital firm In-Q-It. Borio served in multiple leadership roles in the Trump and Obama administrations in the National Security Council and FDA.
Rick Bright, PhD, director of the Biomedical Advanced Research and Development Authority under Trump and Obama. Bright resigned from the government in October after being removed from his vaccine development role by President Trump.
Ezekiel Emanuel, MD, PhD, the vice provost for global initiatives at the University of Pennsylvania. Emanuel served in the Obama administration as special advisor for health policy to Peter Orszag, PhD, the former director of the Office of Management and Budget.
Atul Gawande, MD, MPH, a professor at Harvard Medical School and the Harvard T.H. Chan School of Public Health. Gawande is a staff writer covering health and medicine at the New Yorker and served in the Clinton administration as senior adviser in the Department of Health and Human Services.
Eric Goosby, MD, a professor of medicine at UCSF. Goosby, an expert on HIV/AIDS, led policy work in this field under Clinton and Obama.
Celine Gounder, MD, a clinical assistant professor of internal medicine and infectious diseases at New York University.
Julie Morita, MD, executive vice president of the Robert Wood Johnson Foundation and former commissioner of the Chicago Department of Public Health.
Michael Osterholm, PhD, MPH, director of the Center for Infectious Disease Research and Policy at the University of Minnesota.
Loyce Pace, MPH, president and executive director of the Global Health Council.
Robert Rodriguez, MD, a professor of emergency medicine at UCSF.
If all goes according to plan, health care workers and individuals at high risk for severe illness from COVID-19 could be vaccinated as early as December.
Experts predict that the broader public could start being vaccinated in April.
The distribution of the vaccine could present some challenges for state and federal governments. That or any other unexpected events could delay the vaccine’s distribution.
When drugmaker Pfizer announced that its new vaccine was highly effective at preventing COVID-19, it raised hopes that the coronavirus pandemic could be nearing its end.
In a Nov. 9 press release, the company and its partner BioNTech claimed that an early analysis of clinical trial data found that inoculated individuals experienced 90% fewer cases of symptomatic COVID-19 than those who had received a placebo.
These results surpassed expectations. For months, experts have warned that a new vaccine might only be 60% effective. If Pfizer’s analysis is accurate — and it has yet to produce official scientific documentation — the new vaccine would offer a level of protection equal to that of highly effective vaccines for diseases such as measles.
Experts told us that Pfizer’s announcement is cause for optimism. However, the country, and the world, still have a way to go before coronavirus vaccines become available to ordinary Americans.
Here’s what we know about when the vaccine might be distributed and what that process could look like. What’s next for Pfizer’s vaccine?
If the information in the press release is accurate, Pfizer will likely be the first company to come up with a vaccine that meets the Food and Drug Administration’s requirements for distribution.
To get approval from the FDA, Pfizer has to gather two months of safety data on clinical trial participants to gauge whether the treatment has any negative side effects. The company will reach the two-month benchmark in the third week of November. Barring any unexpected developments, it will then submit its vaccine to the FDA for emergency use authorization, a special provision allowing the use of an unapproved product during a state of emergency.
After Pfizer submits its data to the FDA, the agency will analyze it to see if it’s sufficient to begin distribution. After approval from the FDA, the vaccine would be assessed by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices. The Advisory Committee will then issue a recommendation to the CDC, which will make the final ruling about whether to distribute the vaccine.
This might sound intricate, but James Blumenstock, the chief program officer for health security at the Association of State and Territorial Health Officials, said that the vaccine could probably be approved by the FDA and the CDC in a matter of days rather than weeks.
“Both agencies are standing ready and will give these requests and this assessment the highest level of priority just for expediency’s sake,” he said.
What this means is that high-priority Americans, such as health care workers, could be vaccinated as early as December. What a vaccine rollout might look like.
Pfizer predicts that it will be able to manufacture only 50 million doses for global consumption by the end of the year, enough to vaccinate 25 million people. (The world’s population is about 7.8 billion.)
With a limited number of doses available, the eventual rollout of a vaccine would likely consist of two phases. During the first phase, U.S. health care workers, emergency responders and individuals at higher risk of severe illness would be eligible for vaccination. If all goes according to plan, the first phase will commence sometime in December.
During the second phase, the vaccine would become available to the broader public. Most experts told us that they expect the second phase to start sometime in April, although the date would vary depending on Pfizer’s vaccine production rates and whether other companies get their vaccines greenlit by the FDA and CDC. The state of other vaccines
As of early July, there were roughly 160 vaccine projects under way worldwide, according to the World Health Organization.
Pfizer’s announcement bodes well for other vaccine candidates, said Matthew B. Laurens, an associate professor of pediatrics at the University of Maryland School of Medicine’s Center for Vaccine Development and Global Health.
Pfizer’s vaccine uses genetic material, known as mRNA, that provides the instructions for a body to produce coronavirus proteins, known as antigens, in the hope that these could prime the human immune system to fight the virus. The biotechnology company Moderna is also manufacturing a vaccine that uses mRNA and is set to receive trial data by the end of November.
Other companies in the United States and Europe producing a vaccine include Novavax, which plans to start clinical trials in the U.S. and Mexico by the end of November; Johnson & Johnson, which recently resumed testing its vaccine candidate after a brief pause; and AstraZeneca, which expects to have clinical trial data by the end of the year.
The more companies there are that are able to produce a vaccine, the quicker the vaccine will become widely available, experts say.
Vaccine presents potential distribution hurdles
The CDC will be in charge of the distribution process, with involvement from the U.S. Defense Department, said Dr. Litjen Tan, chief strategy officer for the Immunization Action Coalition, which distributes information about vaccines to try to increase vaccination rates.
Vaccines would be manufactured and then transported to states, which will then pass the vaccine on to providers, such as hospitals. The McKesson Corp., which has received a federal contract to distribute the treatment, will assist pharmaceutical companies and the government with the shipping process.
Shipping the doses will present some challenges. Pfizer’s vaccine has complex and ultra-cold storage requirements that many hospitals, particularly those in hard-to-reach areas, won’t be able to meet.
The cold chain requirement “is an issue for Pfizer, but manufacturing and distribution are issues for all vaccines,” said Robert Finberg, a physician and infectious disease specialist at the University of Massachusetts Medical Center.
To surmount this hurdle, Pfizer plans to transport the vaccine in thermal shippers that can keep the vaccine at the necessary temperature of minus 70 degrees Celsius for about two weeks. However, the shippers themselves present additional problems for distribution, Tan said. Each shipment consists of five trays containing 975 doses of vaccine, and reducing the size of the shipment could dramatically raise the cost of distribution.
As a result, the states might initially prioritize shipping the vaccine to major hospitals rather than rural hospitals that service fewer patients in order to avoid waste.
Blumenstock told us that state and federal governments are working hard to make sure that all regions of the U.S. receive proportionate amounts of vaccine. However, he acknowledged that hospitals in remote areas that don’t service many patients could initially take longer to get the vaccine than a well-trafficked hospital in a heavily populated area.
“Outskirt hospitals won’t be ignored or marginalized, even if it takes more time and effort to get them the vaccine,” he said. “One of the primary principles will be equitable distribution, even when that means you need to take extraordinary measures for logistics, transportation, and handling.”
Overall, experts said that Pfizer’s announcement is a significant step forward. “I’m optimistic that we have a vaccine that’s safe and effective,” said Tan. “And I’m glad that what we’re dealing with now is the problem of how to get it to the public.”






![builders quote [2] - Quotes links](https://lh5.ggpht.com/-eOW-RtPlZ8A/TbgYd_yZVmI/AAAAAAAAABk/2we6uyrhqmU/s1600/btw102-teamwork.jpg)