
Cartoon – Do you work here…
https://apnews.com/article/kaiser-health-care-workers-strike-b8b40ce8c082c0b8c4f1c0fb7ec38741

Picketing began Wednesday at Kaiser Permanente hospitals as some 75,000 health care workers went on strike in Virginia, California and three other states over wages and staffing shortages, marking the latest major labor unrest in the United States.
Kaiser Permanente is one of the country’s larger insurers and health care system operators, with 39 hospitals nationwide. The nonprofit company, based in Oakland, California, provides health coverage for nearly 13 million people, sending customers to clinics and hospitals it runs or contracts with to provide care.
The Coalition of Kaiser Permanente Unions, representing about 85,000 of the health system’s employees nationally, approved a strike for three days in California, Colorado, Oregon and Washington, and for one day in Virginia and Washington, D.C.
A cheer went up from union members outside Kaiser Permanente Los Angeles Medical Center when the strike deadline arrived before dawn.
The strikers include licensed vocational nurses, home health aides and ultrasound sonographers, as well as technicians in radiology, X-ray, surgical, pharmacy and emergency departments.
Doctors are not participating, and Kaiser says its hospitals, including emergency rooms, will remain open during the picketing. The company said it was bringing in thousands of temporary workers to fill gaps during the strike. But the strike could lead to delays in getting appointments and non-urgent procedures being rescheduled.
It comes amid unprecedented worker organizing — from strike authorizations to work stoppages — within multiple industries this year, including, transportation, entertainment and hospitality.
Wednesday’s strike is the latest one for the health care industry this year as it continues to confront burnout with the heavy workloads — problems that were exacerbated greatly by the pandemic.
Unions representing Kaiser workers in August asked for a $25 hourly minimum wage, as well as increases of 7% each year in the first two years and 6.25% each year in the two years afterward.
They say understaffing is boosting the hospital system’s profits but hurting patients, and executives have been bargaining in bad faith during negotiations.
“They’re not listening to the frontline health care workers,” said Mikki Fletchall, a licensed vocational nurse based in a Kaiser medical office in Camarillo, California. “We’re striking because of our patients. We don’t want to have to do it, but we will do it.”
Kaiser has proposed minimum hourly wages of between $21 and $23 next year depending on the location.
Since 2022, the hospital system has hired 51,000 workers and has plans to add 10,000 more people by the end of the month.
Kaiser Permanente reported $2.1 billion in net income for this year’s second quarter on more than $25 billion in operating revenue. But the company said it still was dealing with cost headwinds and challenges from inflation and labor shortages.
Kaiser executive Michelle Gaskill-Hames defended the company and said its practices, compensation and retention are better than its competitors, even as the entire sector faces the same challenges.
“Our focus, for the dollars that we bring in, are to keep them invested in value-based care,” said Gaskill-Hames, president of Kaiser Foundation Health Plan and Hospitals of Southern California and Hawaii.
She added that Kaiser only faces 7% turnover compared to the industry standard of 21%, despite the effects of the pandemic.
“I think coming out of the pandemic, health care workers have been completely burned out,” she said. “The trauma that was felt caring for so many COVID patients, and patients that died, was just difficult.”
The workers’ last contract was negotiated in 2019, before the pandemic.
Hospitals generally have struggled in recent years with high labor costs, staffing shortages and rising levels of uncompensated care, according to Rick Gundling, a senior vice president with the Healthcare Financial Management Association, a nonprofit that works with health care finance executives.
Most of their revenue is fixed, coming from government-funded programs like Medicare and Medicaid, Gundling noted. He said that means revenue growth is “only possible by increasing volumes, which is difficult even under the best of circumstances.”
Workers calling for higher wages, better working conditions and job security, especially since the end of the pandemic, have been increasingly willing to walk out on the job as employers face a greater need for workers.
The California legislature has sent Democratic Gov. Gavin Newsom a bill that would increase the minimum wage for the state’s 455,000 health care workers to $25 per hour over the next decade. The governor has until Oct. 14 to decide whether to sign or veto it.

With Medicare’s Annual Election Period (also known as Open Enrollment) beginning on October 15th, over 65 million adults across the United States will have until December 7th to decide whether they plan to renew or change their Medicare coverage. Beneficiaries choose between Traditional Medicare (TM) and a variety of Medicare Advantage (MA) plans and prescription drug coverage.
For this enrollment cycle, it is estimated that the average beneficiary will have over 40 plans to choose from, leading to complexity. For those who are dually eligible for both Medicare and Medicaid benefits, there is an even greater number of options for them to consider, especially if they live in areas where integrated options such as dual-eligible special needs plans and Medicare-Medicaid plans are available.
As the US population continues to age and the number of Medicare enrollees grow, it is important to understand how beneficiaries make their coverage decisions and ensure they are protected from any misinformation in the process.
Though already complex, the plan selection process for older adults is further complicated by the deceptive marketing tactics that brokers, agents, and third-party marketing organizations (TPMOs) have employed in recent years. In a recent study, the Commonwealth Fund identified how some of these practices are driven by the financial incentives associated with enrolling beneficiaries in particular MA plans.
Between robocalls and misleading television advertisements, many beneficiaries across the country have found themselves enrolled in MA plans they did not intend to enroll in, or that did not cover services or in-network providers that they were initially marketed. In a sweeping review of Medicare Open Enrollment-related television ads, Kaiser Family Foundation found that the majority of Open Enrollment-related advertisements last year promoted the Medicare logo and privately-operated hotlines, misleading beneficiaries into believing these were government sponsored ads and helplines.
Acknowledging the growing concerns and complaints among beneficiaries, the Centers for Medicare and Medicaid Services (CMS) announced that starting in 2024, Medicare-related television ads must be approved in advance of airing and cannot contain plan names or Medicare logos and images that misrepresent their organization or agency. Additional consumer protections included in the 2024 MA and Part D Final Rule will hold brokers, agents, and other TPMOs to higher standards of providing transparent, quality information. These activities include monitoring TPMO behavior, regulating how and when they market to beneficiaries, ensuring brokers review the full list of options and choices available to a beneficiary, and going through a detailed, standardized set of pre-enrollment questions. There is also an increased effort in getting beneficiaries to use some of the federally funded tools and resources available to assist in their coverage decisions.
Some of these tools include the Medicare.gov website, the CMS Medicare Plan Compare tool, and a 1-800-MEDICARE hotline to help inform beneficiaries about their benefits. However, a study by Hernandez et al. revealed that very few Medicare beneficiaries utilized these tools and often felt more comfortable discussing their options in-person with brokers or family members and friends, even though these sources may be biased or potentially inaccurate. Additionally, it is important to recognize that navigating these tools requires some degree of health literacy and technological proficiency, which may disproportionately affect those who are low-income, have lower levels of education, or are non-native English speakers.
The State Health Insurance Assistance Program (SHIP), however, is a free and unbiased resource for Medicare counseling that few beneficiaries are aware of. In 1990, the federal government implemented SHIPs to help support Medicare beneficiaries with free, one-to-one health insurance counseling and education within their communities. It is currently run by the Administration for Community Living (ACL). The ACL administers grants to states, who in turn provide funding to community-level subgrantees to maintain various networks of full-time, part-time, and/or volunteer counselors. The latest available data suggests that SHIPs provided assistance to 2.7 million Medicare beneficiaries from April 2018 through March 2019—just 4.5% of the eligible Medicare population.
While some states had greater success, serving over 10% of their eligible population, others were only able to reach as few as 2%. A 2018 evaluation of California’s SHIP, called HICAP (Health Insurance Counseling & Advocacy Program), highlighted the strengths of this community-based counseling system. HICAP reported high rates of engagement, citing their ability to deliver uniquely tailored counseling to beneficiaries in their native languages and through in-person or hybrid settings depending on the beneficiary’s condition or preferences. Moreover, strong marketing efforts via Spanish radio shows and mailing postcards were particularly effective in reaching “hard-to-locate” populations. However, the program did experience challenges given the variation in operations across locations, citing concerns over the recruitment, training and retention of volunteers and paid staff.
In recognition of SHIP’s potential to provide an unbiased alternative to brokers and combat misinformation, CMS finalized a requirement in the 2024 MA and Part D rule that TPMOs are to provide a disclaimer citing SHIP as an option for beneficiaries to obtain additional help (42 CFR § 422.2267(e )(41)). But despite SHIP’s promise, some beneficiary advocates have worried that the multi-tiered, volunteer, and part-time driven delivery model that characterizes most SHIPs leads to access and quality gaps. This is especially a concern among vulnerable beneficiaries who may live in low-income neighborhoods, have disabilities, or limited English proficiency. Given their historically low utilization rates and limited visibility, others have expressed concern that SHIPs may be ill-equipped to handle an increased demand for services in the coming year, due to more Medicare beneficiaries being advised of their existence through TPMO disclaimers. With the limited evidence about SHIP’s performance and outreach nationally, given the diffuse nature of the program, it will be important to understand some of the barriers and facilitators they face to delivering timely and accurate Medicare counseling.
The free and unbiased nature of the SHIP program presents a promising alternative to helping beneficiaries navigate complex plan choices for Open Enrollment. As MA enrollment increases and as plan choices become more complex, the SHIP program should be monitored for potential inequities in access to and quality of services based on area income.
For more information about your state’s SHIP program and to find a local Medicare counselor, please visit https://www.shiphelp.org/.
Medicare Advantage provides health coverage to more than half of the nation’s seniors, but a growing number of hospitals and health systems nationwide are pushing back and dropping the private plans altogether.
Among the most commonly cited reasons are excessive prior authorization denial rates and slow payments from insurers. Some systems have noted that most MA carriers have faced allegations of billing fraud from the federal government and are being probed by lawmakers over their high denial rates.
“It’s become a game of delay, deny and not pay,” Chris Van Gorder, president and CEO of San Diego-based Scripps Health, told Becker’s.
“Providers are going to have to get out of full-risk capitation because it just doesn’t work — we’re the bottom of the food chain, and the food chain is not being fed.”
In late September, Scripps began notifying patients that it is terminating Medicare Advantage contracts for its integrated medical groups, a move that will affect more than 30,000 seniors in the region. The medical groups, Scripps Clinic and Scripps Coastal, employ more than 1,000 physicians, including advanced practitioners.
Mr. Van Gorder said the health system is facing a loss of $75 million this year on the MA contracts, which will end Dec. 31 for patients covered by UnitedHealthcare, Anthem Blue Cross, Blue Shield of California, Centene’s Health Net and a few more smaller carriers. The system will remain in network for about 13,000 MA enrollees who receive care through Scripps’ individual physician associations.
“If other organizations are experiencing what we are, it’s going to be a short period of time before they start floundering or they get out of Medicare Advantage,” he said. “I think we will see this trend continue and accelerate unless something changes.”
Bend, Ore.-based St. Charles Health System has taken it a step further and is not only considering dropping all Medicare Advantage plans, but is also encouraging its older patients not to enroll in the private Medicare plans during the upcoming enrollment period in October.
The health system’s president and CEO, CFO and chief clinical officer cited high rates of denials, longer hospital stays and overall administrative burden for clinicians.
“We recognize changing insurance options may create a temporary burden for Central Oregonians who are currently on a Medicare Advantage plan, but we ultimately believe it is the right move for patients and for our health system to be sustainable into the future to encourage patients to move away from Medicare Advantage plans as they currently exist,” St. Charles Health CFO Matt Swafford said.
“I feel terrible for the patients in this situation; it’s the last thing we wanted to do, but it’s just not sustainable with these kinds of losses,” Mr. Van Gorder added. “Patients need to be aware of how this system works. Traditional Medicare is not an issue. With these other models, seniors need to be wary and savvy buyers.”
Here are six more recent examples of hospitals dropping Medicare Advantage contracts:
1. Adena Regional Medical Center is terminating its contract with Anthem BCBS’ Medicare Advantage and managed Medicaid plans in Ohio, effective Nov. 2. The flagship facility of Chillicothe, Ohio-based Adena Health System said rate negotiations between the organizations “have not been productive,” leading it to terminate its agreement with Anthem, whose parent company is Elevance Health.
2. Corvallis, Ore.-based Samaritan Health Services ended its commercial and Medicare Advantage contracts with UnitedHealthcare. The five-hospital, nonprofit health system cited slow “processing of requests and claims” that have made it difficult to provide appropriate care to UnitedHealth’s members, which will be out of network with Samaritan’s hospitals on Jan. 9. Samaritan’s physicians and provider services will be out of network on Nov. 1, 2024.
3. Cameron (Mo.) Regional Medical Center stopped accepting Cigna’s MA plans in 2023 and plans to drop Aetna and Humana in 2024. It plans to continue Medicare Advantage contracts with UnitedHealthcare and BCBS, the St. Joseph News-Press reported in May. Cameron Regional CEO Joe Abrutz previously told the newspaper the decision stemmed from delayed reimbursements.
4. Stillwater (Okla.) Medical Center ended all in-network contracts with Medicare Advantage plans amid financial challenges at the 117-bed hospital. Humana and BCBS of Oklahoma were notified that their MA members would no longer receive in-network coverage after Jan. 1, 2023. The hospital said it made the decision after facing rising operating costs and a 22 percent prior authorization denial rate for Medicare Advantage plans, compared to a 1 percent denial rate for traditional Medicare.
5. Brookings (S.D.) Health System will no longer be in network with any Medicare Advantage plans in 2024, the Brookings Register reported. The 49-bed, municipally owned hospital said the decision was made to protect the financial sustainability of the organization.
6. Louisville, Ky.-based Baptist Health Medical Group went out of network with Humana’s Medicare Advantage and commercial plans on Sept. 22, Fox affiliate WDRB reported.

Something I have been writing about and speaking about recently is how difficult it is to operate a hospital in post-Covid America.
The line-up of management and governing obstacles includes both old and new healthcare issues:
It takes considerable hard thinking within executive suites to figure out the best way forward; to find the best roadmap through—at a minimum—the six obstacles outlined above. And as I have noted in my recent speaking engagements, a solution to one of these obstacles might actually make others of these obstacles more difficult to solve.
I have in recent weeks been looking for a “thought platform” that can assist hospital C-suite executives in resetting managerial expectations and operational initiatives—expectations and initiatives that can more effectively cope with the current and distressingly difficult environment.
Moving the hospital organizational thought platform from its 2019 managerial themes to a more relevant platform that better suits the challenges of 2023 is a managerial problem all of its own. Simply telling a large and very complex healthcare organization to stop thinking in pre-Covid terms is not likely to accomplish much. Before you can establish the organizational thought platform that best guides your hospital forward, you will need a leadership team that is committed to creating a “listening and learning” healthcare company.
A good tool for making your way to a listening and learning organization and eventually to a new and more relevant thought platform is the book The First 90 Days: Proven Strategies for Getting Up to Speed Faster and Smarter, by Michael D. Watkins.
Mr. Watkins is a co-founder of Genesis Advisers and a professor at the IMD Business School in Lausanne, Switzerland. The First 90 Days was originally published in 2003 as a guide to business executives moving into new senior positions of major responsibility. But the book also contains general management advice which is relevant not only to new jobs, but also to executives struggling with fast-changing and especially difficult market conditions.
One of the most compelling chapters in The First 90 Days is a chapter that focuses on the absolute importance of executive learning and the need to accelerate that learning.
While Professor Watkins was making a general business point, I would suggest that the need to accelerate executive learning and listening was never more important than in the “right now” post-Covid healthcare environment. Professor Watkins posed a series of critical leadership learning questions that I have modified to reflect the complex operating conditions of the 2023 hospital.
From that perspective, here are six critical learning questions for the hospital leadership team:
One of my last blogs focused on the importance of vision and strategy in the post-Covid hospital recovery process; the importance of reinventing the hospital of the future that best fits into a rapidly changing marketplace. This marketplace requires entirely new skillsets and functions on top of changing shared experiences and perceived social values. Finding the right going-forward strategy and vision is the first imperative.
But without executive learning and listening that leads directly to organizational-wide learning and listening, the chances of finding your way to that highest and best and most effective vision and strategy will be greatly diminished.
https://mailchi.mp/b7baaa789e52/the-weekly-gist-september-29-2023?e=d1e747d2d8

A number of health systems have recently noted increasing financial challenges for Medicare Advantage (MA) patient admissions.
One CFO shared, “our rates from MA plans are roughly on par with fee-for-service Medicare. Denials have always been a problem, making our [revenue] capture about 90 percent. But this year it’s dropped to 80 percent…it’s a crisis for us, given fast how MA volumes are growing.”
His team investigated the change and found the cause: mean length of stay for MA patients has jumped sharply. The rise was almost entirely due to difficulties in discharging patients to rehab and skilled nursing facilities.
Key insurers have narrowed their postacute networks, resulting in patients spending days waiting for a bed. “The payers told us they had focused the network on ‘high-performing’ providers. Our data and doctors’ experiences say otherwise. They chose a handful of facilities that are cheap, with questionable quality,” their CMO reported. Attempts to engage payers to solve the problem have gone nowhere:
“They have a disincentive to work with us on this. With case rates, they are saving money if patients are languishing in an expensive hospital bed rather than going to rehab.”
This system is exploring expedited placement and expanding their portfolio of home-based care and postacute offerings, while even considering guaranteeing payment themselves. If you’re having similar challenges or have found solutions to help with transitions of care, we’d love to hear from you and learn more.
https://mailchi.mp/b7baaa789e52/the-weekly-gist-september-29-2023?e=d1e747d2d8
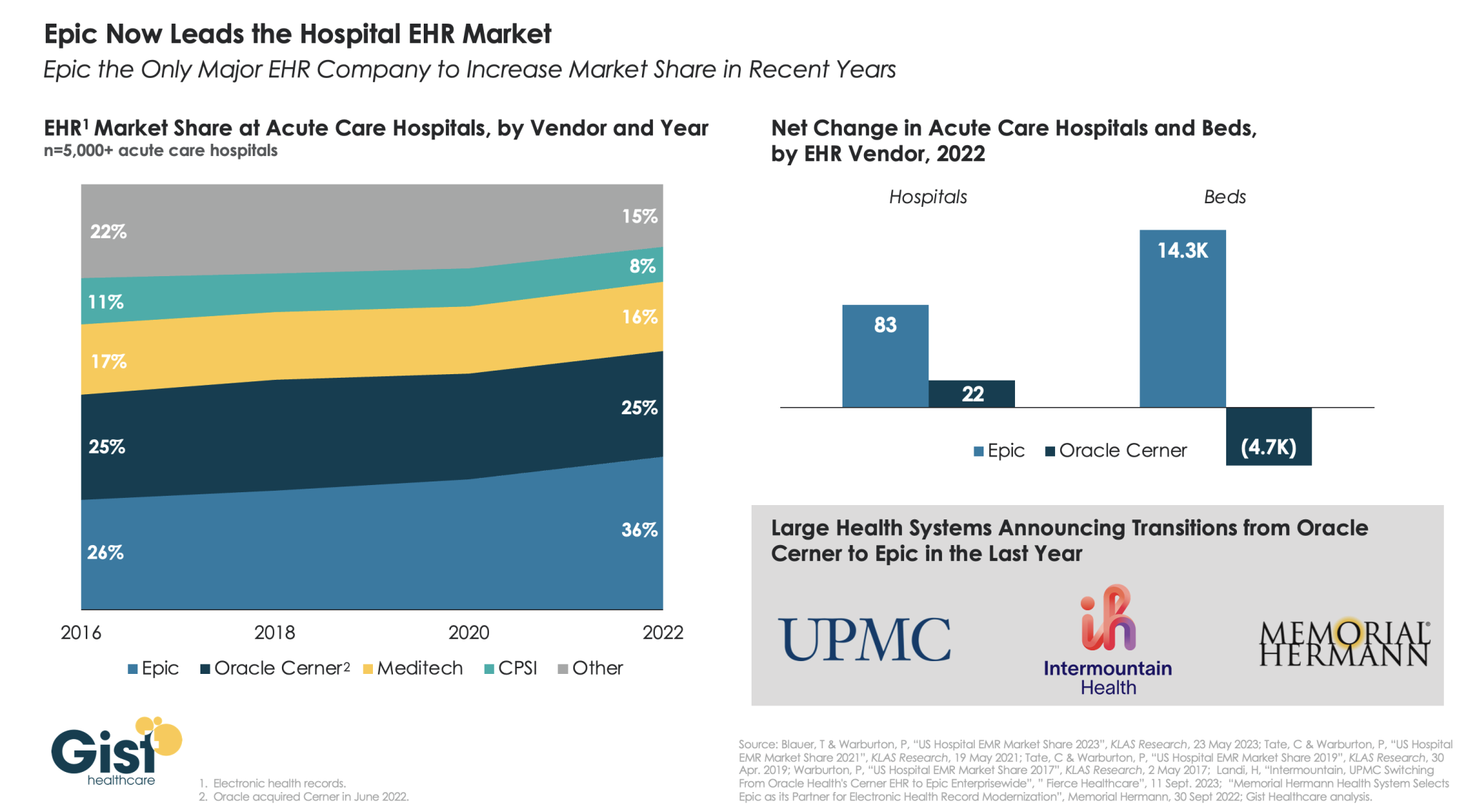
Two large nonprofit health systems made headlines earlier this month announcing that they plan to transition, enterprise-wide, from Oracle Cerner to Epic for their electronic health record (EHR) system.
Using data from KLAS Research, the graphic below shows how Epic has emerged in recent years as the leader in the hospital EHR market. From 2016 to 2022, Epic increased its acute care hospital market share from 26 percent to 36 percent, while its main rival, Oracle Cerner, held flat at 25 percent.
Moreover, Epic is gaining popularity among larger health systems, while Oracle Cerner lost almost 5K beds in 2022, despite gaining 22 hospitals, as it trades large systems for smaller hospitals.
Epic’s ability to consolidate multiple archives into a single, more functional platform has made it popular with physicians, whose feedback was cited by Intermountain as a key reason behind the system’s decision to switch.
With three quarters of Americans having an Epic record, the company is leveraging its pole position in aggregating healthcare data as healthcare approaches the cusp of a generative AI boom, recently announcing an expanded partnership with Microsoft focused on integrating AI tools into its EHR system.

While hospital operating margins remain below historical levels, overall conditions have stabilized in 2023. The median Kaufman Hall Calendar Year-To-Date Operating Margin Index reflecting actual margins was 1.1% in August.
The September issue of the National Hospital Flash Report covers these and other key performance metrics.
DOWNLOAD REPORT
https://mailchi.mp/b7baaa789e52/the-weekly-gist-september-29-2023?e=d1e747d2d8

Published this week in the Harvard Business Review, this intriguing case study tells the story of how Hawaii Pacific Health, a four-hospital system based in Honolulu, worked with its providers to reduce the deluge of needless or low-value administrative tasks required each day by the system’s electronic health record (EHR) platform.
The system’s “Get Rid of Stupid Stuff” (GROSS) initiative created a simple, accessible submission form that allowed providers to flag EHR prompts and workflows ranging from inefficient (printing and scanning discharge papers patients had already signed electronically) to nonsensical (affirming adolescent patients had received proper care for their non-existent umbilical cords). Around 10 percent of suggestions submitted were for prompts that could be immediately eliminated, 15 percent caught gaps in communication and workflow, and the remaining 75 percent identified more complex opportunities for redesign. The GROSS initiative not only freed thousands of labor hours, but also boosted morale by engaging clinicians in the system’s efforts to improve operations.
The Gist: While Hawaii Pacific Health is far from the only system to have successfully engaged its providers in the mission of reducing administrative busywork, this case study provides an example of how sometimes the simplest approaches can be the most effective.
As systems now look to generative AI as the next frontier of bureaucratic efficiency, they will need to optimize workflow processes before automating them in order to avoid ingraining today’s inefficiencies.
https://mailchi.mp/b7baaa789e52/the-weekly-gist-september-29-2023?e=d1e747d2d8
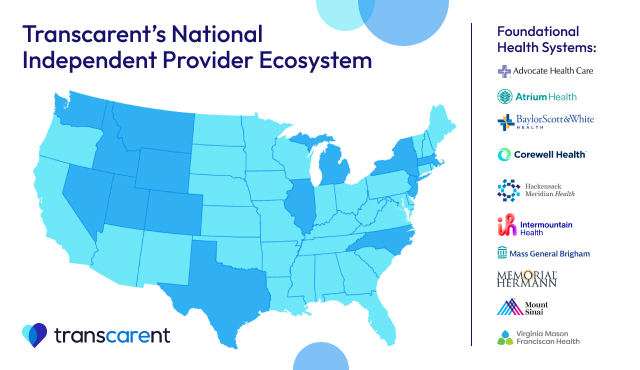
On Tuesday, San Francisco, CA-based healthcare navigation company Transcarent announced ten health systems that will form the initial network for its new direct contracting offering for self-insured employers. The participating health systems include prominent systems like Advocate Health, Intermountain Healthcare, Baylor Scott & White Health, and Mass General Brigham, among others.
Transcarent plans to supplement these care delivery networks with virtual care offerings and digital wraparound services, supported by its recent acquisition of virtual care provider 98point6’s physician portfolio. Transcarent CEO Glen Tullman, who launched the company after selling Livongo to Teladoc in 2020, says the new network’s direct contracting package will guarantee same-day payments to providers and also include value-based incentives.
The Gist: Transcarent was founded with the stated goal of lowering healthcare costs for employers, so it’s notable that the company is launching this direct contracting network with a group of big-name systems that aren’t all known for being value-oriented or low-cost.
But these highly sought-after systems may end up forming an appealing “string of pearls” that attracts large employers and consumers to the product. More employers may be enticed to take a look at Transcarent’s direct contracting model, given employer healthcare costs are projected to rise another 7 percent in 2024, after a similar hike in 2023, and competition for talent has begun to soften
—but the ability of the product to deliver value will depend on the incentives and structure of the offering, about which public details are scarce.
