
Cartoon – Importance of Customer Service

I wrote an Industry Insights article last year about large health system mergers
on the heels of the announcement that behemoths Advocate Aurora and Atrium
Health were coming together. That transaction closed in December of 2022
and since then, we have witnessed numerous other “mega-mergers,” creating health systems with
well over $5 billion in revenue.
With the operating environment for hospitals becoming even more challenging, is getting bigger the solution?
Before we answer that though, let’s take a brief look at the large mergers that have occurred over the past few years.
In 2021, Spectrum and Beaumont in Michigan announced they were coming together to create a $15
billion revenue system now known as Corewell Health. Intermountain and SCL Health came together
to create a $15B system; Illinois systems NorthShore University Health and Edward-Elmhurst
Healthcare ($5B); in Pennsylvania, Jefferson Health closed on its merger with Einstein Healthcare
Network ($8B); Piedmont Healthcare + University Health Care + 4 HCA hospitals in Georgia ($5B);
and North Carolina-based Novant Health closed on its merger with New Hanover Regional ($6B).
In 2022, the keynote merger was Advocate Aurora and Atrium Health coming together to create a
$27 billion multi-state system. There were also other sizeable combinations such as the University of
Michigan Health and Sparrow Health ($7B), South Dakota-based Sanford Health and Minnesota-based Fairview Health ($14B), though that merger has since been called off, Wisconsin’s Marshfield
Clinic and Minnesota’s Essentia Health ($5B), and Wellstar Health and August University Health in
Georgia ($6B).
So far in 2023, the most notable is Kaiser Permanente’s acquisition of PA-based Geisinger Health,
which will take the combined system to over $100 billion in revenue. Other mega-mergers include
BJC Health and St. Luke’s Health System in Missouri ($10B), Froedert Health and ThedaCare in
Wisconsin ($5B), and most recently, Oregon Health & Science University and Legacy Health ($7B).
So why are these systems merging?
For starters, there is the benefit of geographic and revenue diversification. Some markets are more
challenging than others, with diversification across a larger footprint helping to balance the combined
systems. Plus, scale allows the systems to more effectively manage risk. With the need to compete
in a value-based care world, health systems must operate in markets that are large enough to be
effective.
Of critical importance, and another key driver behind these mergers, is the enhanced ability to invest
in technological capabilities. It is important to note technology investments cannot be funded through
traditional tax-exempt debt and as technology plays a more important role in the delivery of
healthcare, not-for-profit systems must make investments to remain competitive. AI, data security,
revenue cycle, innovation, information sharing, etc. are all necessary for the successful delivery of healthcare. Furthermore, not every health system can source, invest, or build the right technology on its own. By combining, systems improve upon their ability to lower their per unit cost of investment in technology.
There is also the people. Human talent is a sought-after resource for hospitals these days and the business of running hospitals has
only gotten tougher. Not every health system can attract the best leaders. By merging, health systems can leverage the capability set
from across the organization to more effectively manage the business.
Another reason is the enhanced capital access. As rates rise and lenders tighten standards, bigger is better; and larger balance sheets
with greater assets and security enhances borrowing capabilities. However, capital access does depend on financial performance, so it
requires earnings creation. The jury is still out on the back-office savings created by these mega-mergers, but over time, with effective
leadership, the right technology, and the necessary scale, achieving synergies must be a motivating factor.
But do mergers actually achieve these goals? I have not yet found an independent study to answer this question as many megamergers are recent and there are many variables that influence the analysis. While an n of 1 would not be acceptable to my actuarial
wife, there are examples that show promising signs. In my home state of NJ, the 2016 merger between Hackensack and Meridian is
notable. Leading up to the merger, Hackensack had $1.7 billion in revenue and was averaging 9% operating EBIDA margins, 150 days
cash on hand, and 1x cash to debt. Meridian had $1.6 billion in revenue and was averaging just over 11% operating EBIDA margins,
240 days cash, and 1.4x cash to debt. Post-merger, the combined system now has $6.6 billion of revenue and not taking into the
account the recent swings during and post-COVID, was averaging 11% EBIDA margins, 270 days cash, and 1.6x cash to debt. For the
combined Hackensack Meridian Health System, 1+1 > 2. They have grown faster, plugged weaknesses, improved their balance sheet,
all while continuing to make investments.
There are many reasons why large systems are pursuing mergers and why we expect to see more. And one of these mega-mergers
could create another competitor to the national for-profit operators like HCA or the large catholic systems like Ascension,
CommonSpirit, Providence, or Trinity.

Medicare starts a long road to cutting prices for drugs, starting with 10 costing it $50.5 billion annually – a health policy analyst explains why negotiations are promising but will take years.
The Biden administration released on Aug. 29, 2023, a list of the first 10 drugs that will be up for negotiations with pharmaceutical companies over their Medicare prices.
The drugs are purchased through Medicare Part D, a prescription drug coverage program for Americans ages 65 and older. The 10 medications accounted for more than US$50.5 billion in gross costs between June 1, 2022, and May 31, 2023.
Provisions authorizing these negotiations were part of the Inflation Reduction Act which Congress passed in 2022, allowing Medicare to negotiate drug prices for the first time. Pending successful negotiations, these changes would amount to what researchers estimated to be net savings of about $1.8 billion in 2026. The Congressional Budget Office projected an even bigger savings of $3.7 billion.
The top 10 list includes such drugs as Johnson & Johnson’s Xarelto, which treats blood clots, and Amgen’s Enbrel, which treats rheumatoid arthritis and psoriasis.
Negotiations are expected to begin in October and continue until August 2024, with lower prices going into effect in 2026.
Democrats have hailed the new law’s drug pricing provisions as game-changing. They’re likely to make the issue a centerpiece of their 2024 election campaigns. Democrats are further emboldened as public opinion polls show overwhelming support for the policy among Americans.
As a scholar who researches the politics of health policy, I’m skeptical that Medicare drug price negotiations will end up making as big a difference as Democrats have promised, at least in the near future. While U.S. prescription drug prices are excessive, the true potential of the policy is unclear, as it remains muddled in lawsuits and industry opposition. However, if it can withstand the ongoing attacks and become settled law, Americans ages 65 and up could see real financial relief down the line.
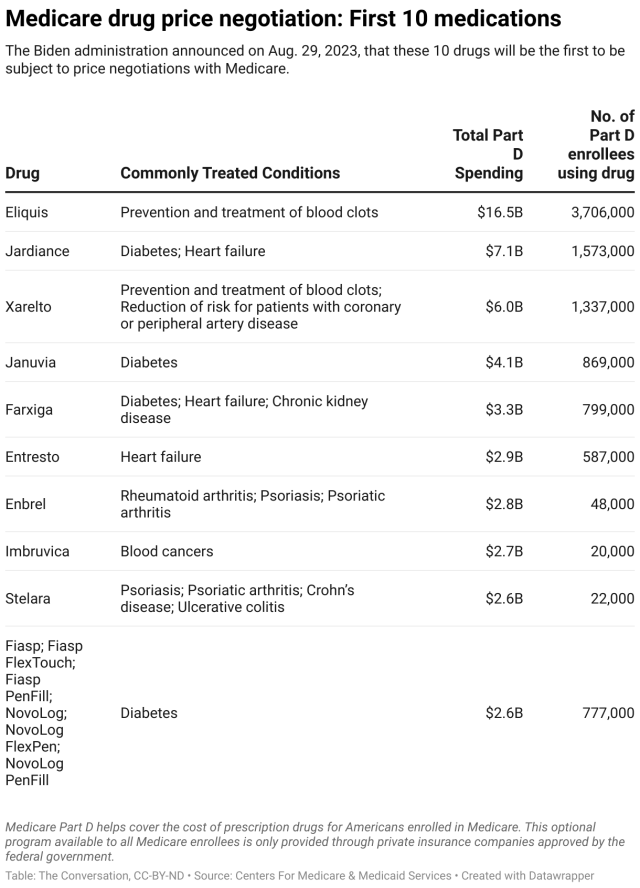
The Inflation Reduction Act allows the Centers for Medicare & Medicaid Services to negotiate prices with the companies that make some of the most expensive drugs in the Medicare program, including life-saving cancer and diabetes treatments like Imbruvica and Januvia.
If the negotiations proceed as planned, the drug-price-negotiation provision is expected to save the U.S. government about $98.5 billion by 2031 by allowing it to pay less on prescription drugs for Americans on Medicare – nearly 66 million people. The Biden administration hopes that these cost savings will be passed down to Americans 65 and older through reduced Medicare Part D premiums and lower out-of-pocket costs.
The Inflation Reduction Act provides additional benefits for older Americans, including limiting their out-of-pocket expenses for prescription drugs to no more than $2,000 annually, limiting the growth of Medicare Part D premiums, eliminating out-of-pocket costs for vaccines and providing premium subsidies to low-income people ages 65 and older.
The Inflation Reduction Act also includes a separate provision that requires drugmakers, under certain conditions, to provide the Medicare program with rebates if drug price increases outpace inflation, starting in January of 2023. That measure is expected to yield $71 billion in savings over a decade.
The 10 drugs that the Centers for Medicare & Medicaid Services have selected accounted for $3.4 billion in out-of-pocket spending in 2022 for Americans ages 65 and older and $50.5 billion, or about 20%, of total Part D gross prescription drug costs from June 1, 2022, to May 31, 2023.
Pharmaceutical companies have to sign agreements to participate in the upcoming negotiations by October 2023. Based on criteria such as public feedback and consultation, as well as the clinical value of the drug, the Centers for Medicare & Medicaid Services will make an initial price offer in early 2024, with the potential to further negotiate the price until August 2024. Going forward, additional drugs will be subject to negotiations.
If drugmakers don’t negotiate, they will face stiff penalties in the form of a tax, reaching as high as 95% of U.S. pharmaceutical product sales. Alternatively, the companies may pull their drugs from the Medicare and Medicaid markets, meaning that seniors on Medicare would lose access to them.
Americans pay substantially more for prescription drugs compared with people who live in countries with similar economies, like Germany, the U.K. and Australia. While Americans spent more than $1,100 a year in 2019, Germans paid $825, the British paid $285 and Australians paid $434 per person.
The reasons for this disparity are multilayered and include the overall complexity of the U.S. health care system and the lack of transparency in the drug supply chain. Of course, many other countries also directly set prices for drugs or use their monopoly on health services to drive down costs.
For example, Dulera, an asthma drug, costs 50 times more in the U.S. than the international average. Januvia, a diabetes drug that is among the first 10 drugs up for price negotiation, and Combigan, a glaucoma drug, cost about 10 times more.
These costs impose a big burden on Americans – 1 in 5 of whom skip at least some of their prescribed medications due to the expense. Those 65 and older are particularly affected by these problems.
It’s too soon to say how big the impact of the drug pricing provisions will be and whether this policy will be sustained.
Drugmakers have opposed any governmental regulation of drug prices for decades. They are fighting the measure in court and running a public relations campaign that warns of reduced investments in life-saving cures because their financial incentives are reduced.
Even if the drug price negotiations survive the industry’s legal challenges, it’s possible that future Republican administrations won’t embrace or enforce this policy. This is because potential Republican wins in the 2024 presidential and congressional elections could unravel or severely curtail the new drug negotiation policy. Indeed, Republicans have been working feverishly on designing a strategy to use the negotiations against Democrats in the upcoming elections.
In my view, the government’s efforts to cut prices for prescription drugs that Part D enrollees obtain are a step in the right direction. For now, the effect will likely be small because patients already receive discounts on the listed drugs, bringing the net savings down substantially. However, the potential for real savings for Americans ages 65 and older will undoubtedly grow as more drugs become subject to negotiation.
At the same time, drug manufacturers have indicated that they are willing to take their legal battles against the Medicare drug pricing reform all the way to the Supreme Court. If that happens, there’s a good chance they will prevail because the arguments made in their lawsuits are likely to appeal to the Supreme Court’s conservative majority, which has been favorable to many of the arguments made by drugmakers in their lawsuits.
Moreover, drugmakers could also simply pull their drugs from Medicare and Medicaid to force the government’s hand. The Centers for Medicare & Medicaid Services seems to have deliberately chosen drugs that make up a high percentage of manufacturers’ drug sales to counter this possibility. The industry has a history of skillfully exploiting loopholes and possesses a vast lobbying apparatus.
It’s also too soon to know if this is going to be a win for American patients overall. It’s possible that Americans who aren’t covered by Medicare may actually see prices go up. That’s because if drugmakers do make less money on drugs for people enrolled in Part D, they might make up for those lost profits by charging more for drugs that other people depend on.
And lastly, it’s possible that there will be fewer new prescription drugs – as an indirect result of this policy that’s supposed to improve access to health care – because it may reduce drugmakers incentives. While the number of cases is likely small, it would potentially take a toll on patients who might have seen a cure to their disease – or some relief from their symptoms.
Influential conservative policy groups are sketching out health care plans for a potential Republican administration over a year before the election.
Why it matters:
Republicans have moved on from the “repeal and replace” — the Affordable Care Act didn’t even get a mention in the first GOP presidential debate last week — but still haven’t settled on new health care agenda.
Context:
The early push to define the next GOP health agenda partly stems from Republicans’ inability to agree on an ACA alternative after former President Trump was elected, despite years of promises to overhaul the 2010 health care law. The GOP policy experts also said they want to avoid repeating the Trump administration’s failure to plan health care executive actions and key staffing decisions before taking office.
Details:
Conservative think tanks are looking to advance some long-held conservative goals like transforming Medicaid’s open-ended entitlement into block grants, but there’s also a new generation of Trump alumni who hope to revive some of his administration’s policies.
Zoom in:
Paragon Health, as well as the Heritage Foundation and America First Policy Institute, are the primary conservative think tanks now drafting health regulations, policy plans and recruiting personnel who could serve in a Republican administration.
Meanwhile, the America First Policy Institute, founded by Trump administration alumni in 2021, has put forward a 12-part health policy agenda it describes as “radical incrementalism.”
The Heritage Foundation has also detailed policy proposals and recently joined more than 70 other conservative groups to launch an initiative called Project 2025 to develop a governing agenda.
What we’re watching: The GOP presidential candidates themselves have said relatively little so far about their plans for the health care system. That could eventually change, given Americans’ concern over health care costs.

Over the past 20 years, we’ve seen an evolution in payor contracts from fee-for-service to value-based care (VBC). This evolution is occurring across payor types: Commercial, Medicare, and Medicaid. In recent years, many providers have signed VBC contracts, which often provide better reimbursement rates as a reward for improvements in care delivery and care outcomes.
Specifically, a significant number of providers signed incentive-laden 5-10-year VBC contracts in 2020 moving away from traditional fee-for-service models, which helped improve their financial positioning throughout the pandemic. However, recent economic shifts have changed the landscape in which these contracts exist. Current contracts fail to take into account the rate of inflation and heightened financial distress we are seeing in the industry today. They also do not take into consideration the fact that many COVID-19-era government relief options — such as the CARES Act, Provider Relief Fund, and American Rescue Plan of 2021 — are sunsetting.
Simply stated, VBC contracts negotiated pre-pandemic are not only obsolete but likely contain pricing provisions that do not consider either unprecedented cost increases or difficulty in meeting performance incentives due to changes in patient behaviors. The result is an urgent need to reassess payor contracts of all types across all payor types.
However, before you renegotiate your contracts, you need to carefully consider your organization’s structure and business model so that you can ensure you’re working toward the best possible outcome.
To begin, take some time to examine the following considerations:
· Market Position: Having greater market share often leads to better-negotiated rates. Your organization should understand its market position before renegotiating its VBC contracts to understand what advantages you may have.
· Total Reimbursement & Total Value: Assess your total reimbursement rates, base reimbursement, and incentive reimbursement opportunity.
· Current Yield: Determine the percentage of total cost and the value of your denials and write-offs.
· Fee-for-service vs. Risk-based Models: Fee-for-service-based models should assess their steerage. Risk-based models should identify actuarily sound allocations, percentage of premium reconciliations, and risk adjustments/risk scores.
· IT Infrastructure: Evaluate your IT infrastructure. For example, is your EHR system set up for data analysis and able to benchmark KPIs? It’s important that your systems are designed to provide this information for negotiations and to ensure you have a complete picture of your patient population.
· Business Structure: Some provider organizations benefit from VBC models more than others. For example, a primary care provider (PCP) is more likely to coordinate along the continuum of care than a specialist. This enables the PCP to potentially have more control over the cost of care and revenue streams than specialists, making them a better candidate for a risk-based contract.
Carefully considering these six factors is a crucial first step to renegotiating your value-based contracts. Once you’ve made these considerations, you’re ready to move forward.
Ready to get started renegotiating your value-based contracts? Read our insight to get five tips for negotiation success.
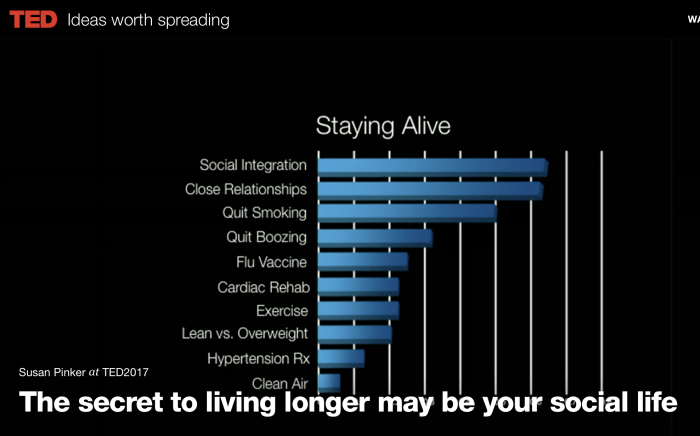
What does it take to live 100 years?
These predictors of a long health life may surprise you!
Watch the full TED Talk here: http://t.ted.com/jyX2zKP



