


The Trump administration finalized a hospital payment rule Friday that retains proposed cuts to off-campus clinics and the 340B drug discount program.
The changes outlined in the hospital Outpatient Prospective Payment System (OPPS) rule come despite both cuts being struck down in legal challenges and amid major pushback from providers.
The agency decided to move ahead with the two-year phase-in of the cuts to outpatient services for clinic visits furnished in an off-campus hospital outpatient setting. The goal is to bring payments to off-campus clinics in line with standalone physicians’ offices.
“With the completion of the two-year phase-in, the cost sharing will be reduced to $9, saving beneficiaries an average of $14 each time they visit an off-campus department for a clinic visit in [calendar year] 2020,” the Centers for Medicare & Medicaid Services (CMS) said in a fact sheet.
However, the two-year project that was supposed to start in 2019 has been halted because of a federal court ruling.
CMS decided to move forward with the cuts for off-campus clinics.
“The government has appeal rights, and is still evaluating the rulings and considering, at the time of this writing, whether to appeal the final judgment,” the agency said.
The American Hospital Association (AHA) said that the site-neutral payment rule was misguided and that CMS ignored the recent court ruling.
“There are many real and crucial differences between hospital outpatient departments and the patient populations they serve and other sites of care,” said Tom Nickels, executive vice president of the AHA, in a statement.
CMS also finalized a proposed cut for the 340B program that cuts payments by 22.5% in 2020.
CMS has installed prior cuts in 2018 and 2019 to the program that requires drug companies to provide discounts to safety-net hospitals in exchange for getting their products covered on Medicaid.
However, a court ruling has struck down the cuts, and CMS is currently appealing the decision.
CMS said that it hopes to conduct a 340B hospital survey to collect drug acquisition cost data for 2018 and 2019, and the survey will craft a remedy if the appeal doesn’t go their way.
“In the event the 340B hospital survey data are not used to devise a remedy, we intend to consider the public input to inform the steps we would take to propose a remedy for CYs 2018 and 2019 in the CY 2021 rulemaking,” the agency said.
Hospital groups commented that CMS should drop both the 340B and site-neutral cuts because of the legal challenges.
Several groups weren’t happy that the cuts were still there.
“The agency also prolongs confusion and uncertainty for hospitals by maintaining unlawful policies it has been told to abandon in clear judicial directives,” said Beth Feldpush, senior vice president of policy and advocacy for America’s Essential Hospitals, in a statement Friday.
The hospital-backed group 340B Health added that CMS needs to stop this “unfunny version of ‘Groundhog Day’ and restore Medicare payments for 340B hospitals to their legal, statutory level.”
Elizabeth Warren, who rose to the top with big liberal bets, is banking a big slice of her presidential run on full-throated support for Medicare for All.
Why it matters: Warren is taking a beating on social media after claiming middle class Americans won’t pay higher taxes to fund health care coverage fully paid for by taxpayers, according to data from NewsWhip provided exclusively to Axios. At the same time, her poll numbers nationally are slipping.
https://www.axios.com/public-health-crisis-trends-future-c24f9720-4657-45f2-ab73-05a8bb9a4d3e.html
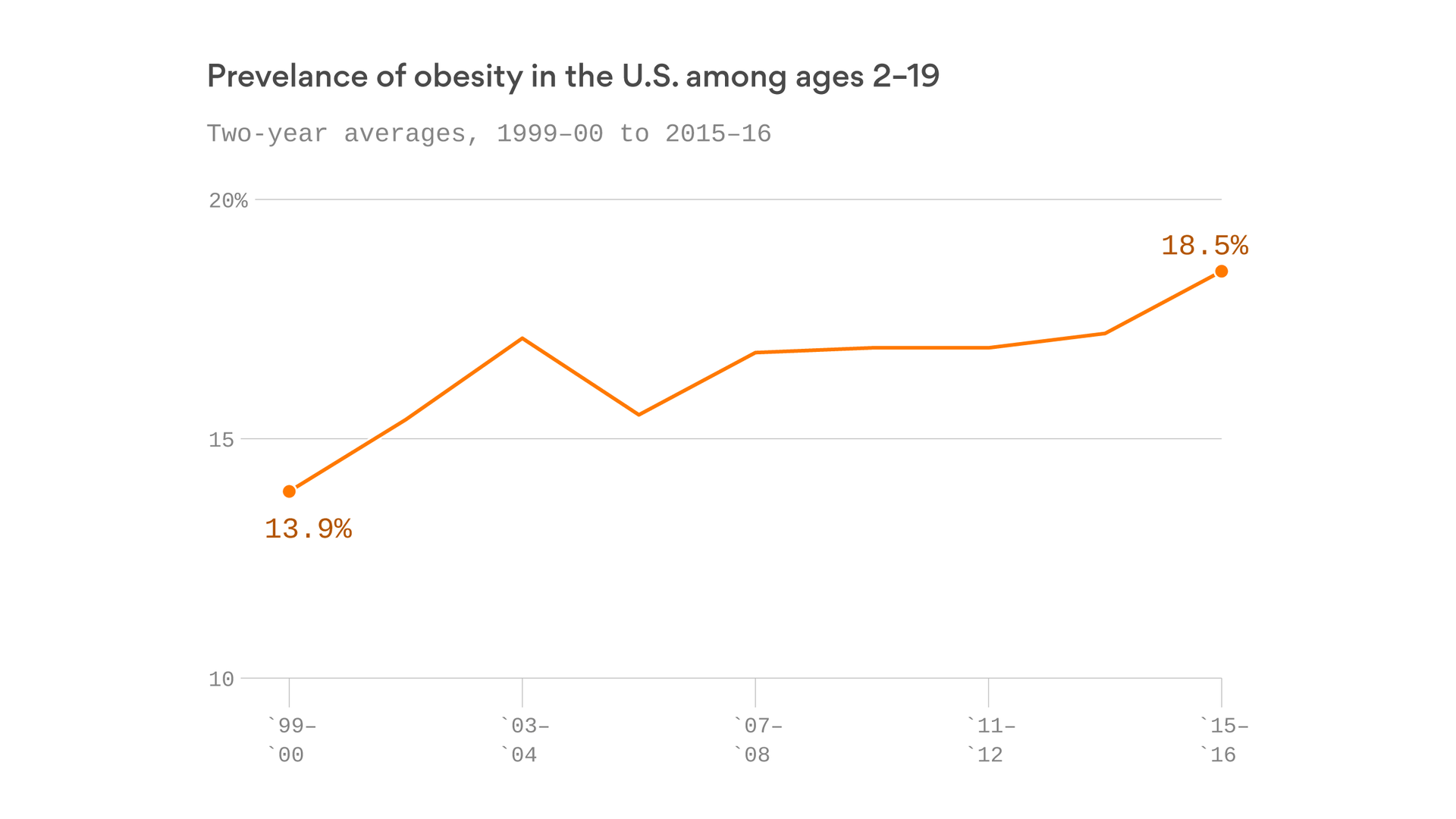
The health troubles we’re seeing now — especially among young people — will continue to strain the system for years and even decades to come.
The big picture: Rising obesity rates now will translate into rising rates of type 2 diabetes and heart disease. The costs of the opioid crisis will continue to mount even after the acute crisis ends. And all of this will strain what’s already the most expensive health care system in the world.
https://apnews.com/40211902a28946fe89f3f92b3c084e51

The first attempt in the United States to use a gene editing tool called CRISPR against cancer seems safe in the three patients who have had it so far, but it’s too soon to know if it will improve survival, doctors reported Wednesday.
The doctors were able to take immune system cells from the patients’ blood and alter them genetically to help them recognize and fight cancer, with minimal and manageable side effects.
The treatment deletes three genes that might have been hindering these cells’ ability to attack the disease, and adds a new, fourth feature to help them do the job.
“It’s the most complicated genetic, cellular engineering that’s been attempted so far,” said the study leader, Dr. Edward Stadtmauer of the University of Pennsylvania in Philadelphia. “This is proof that we can safely do gene editing of these cells.”
After two to three months, one patient’s cancer continued to worsen and another was stable. The third patient was treated too recently to know how she’ll fare. The plan is to treat 15 more patients and assess safety and how well it works.
“It’s very early, but I’m incredibly encouraged by this,” said one independent expert, Dr. Aaron Gerds, a Cleveland Clinic cancer specialist.
Other cell therapies for some blood cancers “have been a huge hit, taking diseases that are uncurable and curing them,” and the gene editing may give a way to improve on those, he said.
Gene editing is a way to permanently change DNA to attack the root causes of a disease. CRISPR is a tool to cut DNA at a specific spot. It’s long been used in the lab and is being tried for other diseases.
This study is not aimed at changing DNA within a person’s body. Instead it seeks to remove, alter and give back to the patient cells that are super-powered to fight their cancer — a form of immunotherapy.
Chinese scientists reportedly have tried this for cancer patients, but this is the first such study outside that country. It’s so novel that it took more than two years to get approval from U.S. government regulators to try it.
The early results were released by the American Society of Hematology; details will be given at its annual conference in December.
The study is sponsored by the University of Pennsylvania, the Parker Institute for Cancer Immunotherapy in San Francisco, and a biotech company, Tmunity Therapeutics. Several study leaders and the university have a financial stake in the company and may benefit from patents and licenses on the technology.
Two of the patients have multiple myeloma, a blood cancer, and the third has a sarcoma, cancer that forms in connective or soft tissue. All had failed multiple standard treatments and were out of good options.
Their blood was filtered to remove immune system soldiers called T cells, which were modified in the lab and then returned to the patients through an IV. It’s intended as a one-time treatment. The cells should multiply into an army within the body and act as a living drug.
So far, the cells have survived and have been multiplying as intended, Stadtmauer said.
“This is a brand new therapy” so not it’s not clear how soon any anti-cancer effects will be seen. Following these patients longer, and testing more of them, will tell, he said.

Almost all of the major health insurance companies are spending more on medical care this year than they have in the past, Axios’ Bob Herman reports.
The big picture: Rising prices and more services for some sicker patients are among the many reasons why this is happening. That uptick in spending has freaked out Wall Street, even though insurers are still quite profitable.
Driving the news: Almost all of the eight major publicly traded insurers have shown their medical loss ratio — the percentage of premium revenues they’re spending on medical claims — is rising this year.
Between the lines: Medical loss ratios are often higher for health plans that cover more older adults, the disabled and the poor, because those groups typically need more care or are in the hospital more frequently.
But costs have been climbing in some commercial markets, too.
The bottom line: Health insurance companies closely track their medical loss ratios and aim to hit those targets most often by charging higher premiums, denying care, forcing people to use lower-priced providers or declining to cover people they deem to be too expensive.