The complexity of Medicare Advantage (MA) physician networks has been well-documented, but the payment regulations that underlie these plans remain opaque, even to experts. If an MA plan enrollee sees an out-of-network doctor, how much should she expect to pay?
The answer, like much of the American healthcare system, is complicated. We’ve consulted experts and scoured nearly inscrutable government documents to try to find it. In this post we try to explain what we’ve learned in a much more accessible way.
Medicare Advantage Basics
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third of the 60+ million Americans covered by Medicare are enrolled in MA plans. These plans, subsidized by the government, are governed by Medicare rules, but, within certain limits, are able to set their own premiums, deductibles, and service payment schedules each year.
Critically, they also determine their own network extent, choosing which physicians are in- or out-of-network. Apart from cost sharing or deductibles, the cost of care from providers that are in-network is covered by the plan. However, if an enrollee seeks care from a provider who is outside of their plan’s network, what the cost is and who bears it is much more complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers, which constitute about 97% of all physicians in the U.S., accept Medicare Fee-For-Service (FFS) rates for full payment of their services. These are the rates paid by TM. These doctors are subject to the fee schedules and regulations established by Medicare and MA plans.
Non-participating providers (about 2% of practicing physicians) can accept FFS Medicare rates for full payment if they wish (a.k.a., “take assignment”), but they generally don’t do so. When they don’t take assignment on a particular case, these providers are not limited to charging FFS rates.
Opt-out providersdon’t accept Medicare FFS payment under any circumstances. These providers, constituting only 1% of practicing physicians, can set their own charges for services and require payment directly from the patient. (Many psychiatrists fall into this category: they make up 42% of all opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So, if an MA beneficiary goes to see an out-of-network doctor, by whom does the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member willingly seeks care from an out-of-network provider, the member assumes full liability for payment.That is, neither the HMO plan nor TM will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies, and must be disclosed to the patient before any services are administered. If the provider is participating with Medicare (in the sense defined above), they charge the patient no more than the standard Medicare FFS rate for their services. Non-participating providers that do not take assignment on the claim are limited to charging the beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states further restrict this. In New York State, for instance, the maximum is 105% of Medicare FFS payment.) In these cases, the provider charges the patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare, there are no limits to what they can charge for their services. The provider and patient enter into a private contract; the patient agrees to pay the full amount, out of pocket, for all services.
Figure 1: MA HMO Out-of-Network Payments
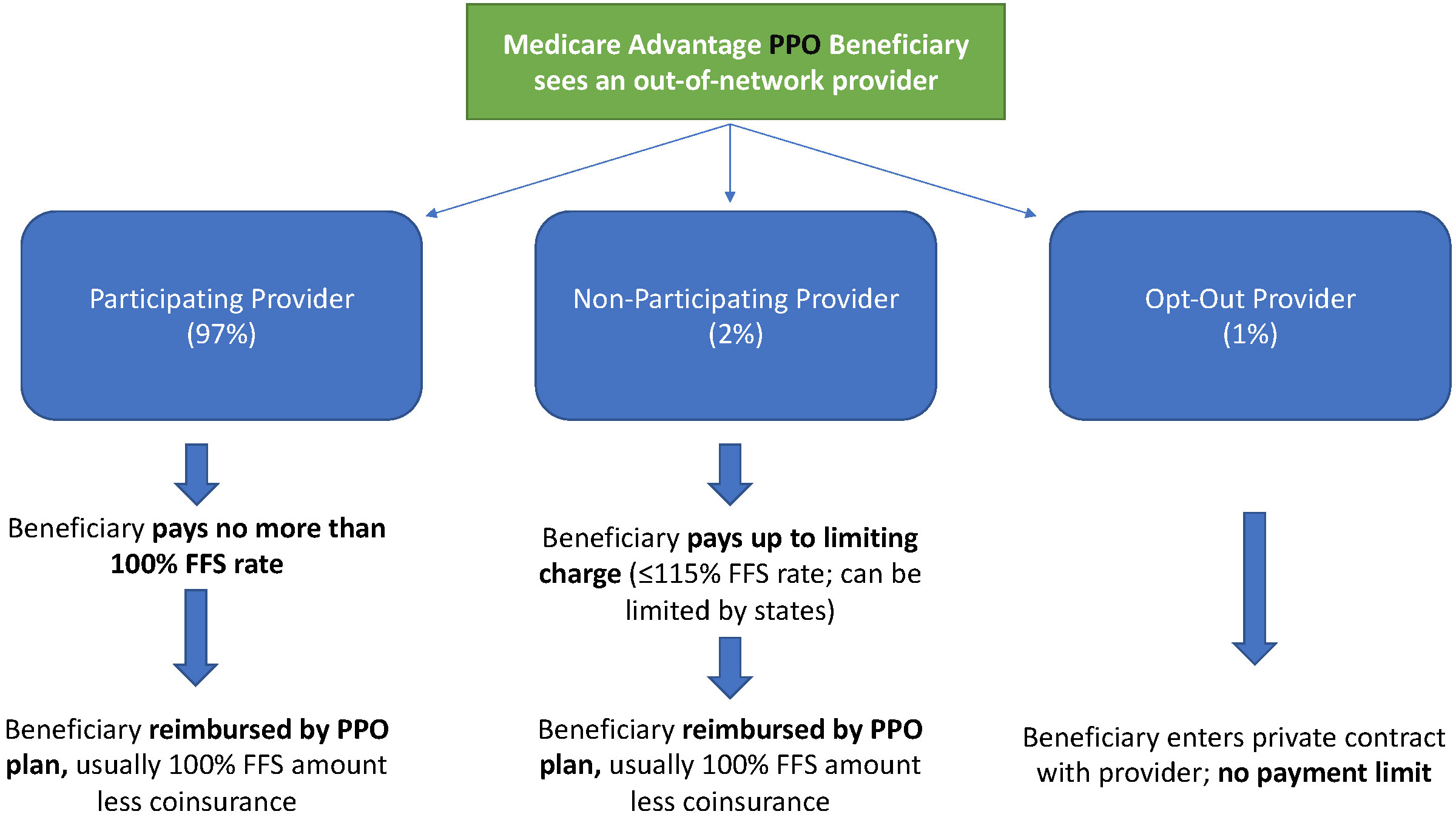
MA PPO plans operate slightly differently. By nature of the PPO plan, there are built-in benefits covering visits to out-of-network physicians (usually at the expense of higher annual deductibles and co-insurance compared to HMO plans). Like with HMO enrollees, an out-of-network Medicare-participating physician will charge the PPO enrollee no more than the standard FFS rate for their services. The PPO plan will then reimburse the enrollee 100% of this rate, less coinsurance. (See Figure 2.)
In contrast, a non-participating physician that does not take assignment is limited to charging a PPO enrollee 115% of the Medicare FFS amount, which can be further limited by state regulations. In this case, the PPO enrollee is also reimbursed by their plan up to 100% (less coinsurance) of the FFS amount for their visit. Again, opt-out physicians are exempt from these regulations and must enter private contracts with patients.
Figure 2: MA PPO Out-of-Network Payments
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare) and the provider happens to be out-of-network for the MA plan (regardless of HMO/PPO status), the plan must cover the services at their established in-network emergency services rates.
The second caveat is in regard to the declared public health emergency due to COVID-19 (set to expire in April 2021, but likely to be extended). MA plans are currently required to cover all out-of-network services from providers that contract with Medicare (i.e., all but opt-out providers) and charge beneficiaries no more than the plan-established in-network rates for these services. This is being mandated by CMS to compensate for practice closures and other difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside of the pandemic and emergency situations, knowing how much you’ll need to pay for out-of-network services as a MA enrollee depends on a multitude of factors. Though the vast majority of American physicians contract with Medicare, the intersection of insurer-engineered physician networks and the complex MA payment system could lead to significant unexpected costs to the patient.
Part one of our six-part series on vaccinations, supported by the National Institute for Health Care Management Foundation, dives into the history of variolation, exploring the beginning of the long road that led to vaccines as we know them today.
President Biden promised on the campaign trail to expand the Affordable Care Act to cover more of the roughly 29 million nonelderly Americans (about 11 percent of that population) who remain uninsured. He also said he’d strengthen the law by, for instance, providing an accessible and affordable public option and increasing tax credits to make it easier for people who buy insurance on their own to afford monthly premiums. Once in office, Biden immediately moved to reopen the period when people could enroll in the ACA marketplaces.
Unfortunately, the administration is paying little heed to a problem that is in many ways just as insidious as lack of insurance: underinsurance. That’s when people get too little from the insurance plans that they do have.
After passage of the ACA, the number of Americans lacking any insurance fell by 20 million, dropping to 26.7 million in 2016 — a historic low as a percentage of population. The figure began to creep up again during the Trump administration, reaching 28.9 million in 2019. That’s the problem that the current administration wants to address, and it certainly needs attention.
But according to research by the Commonwealth Fund, a foundation focused on health care, 21.3 percent of Americans have insurance so skimpy that they count as underinsured: Their out-of-pocket health-care expenses, excluding premiums, amount to at least 5 to 10 percent of household income. The limits in coverage mean their plans might provide little financial protection in a health-care crisis.
High-deductible plans offered by employers are one part of the problem. Among people covered by the companies they work for, enrollment in high-deductible health plans rose from 4 percent in 2006 to 30 percent in 2019, according to a report from the Kaiser Family Foundation. The average annual deductibles in such plans are $2,583 for an individual and $5,335 for families.
In theory, high-deductible plans, which make people spend lots of their own money before insurance kicks in, turn people into careful consumers. But research finds that people covered by such plans skip care, both unnecessary (elective cosmetic surgery, for instance) and necessary (cancer screenings and treatment, and prescriptions).Black Americans in these plans disproportionately avoid treatment, widening racial health inequities.
Health savings accountsare designed to blunt the harmful effects of high-deductible plans: Contributions by employers, and pretax contributions by individuals, help to cover costs until the deductible is reached. But not all high-deductible health plans offer such accounts, and many people in lower-wage jobs don’t have them. In the rare cases that they do, they often don’t have extra money to deposit in them.
In a November 2020 article in the journal Health Affairs, scholars affiliated with Brown University and Boston University found that enrollment in high-deductible plans had increased across all racial, ethnic and income groups from 2007 to 2018; they also found that low-income, Black and Hispanic enrollees were significantly less likely than other groups to have a health savings account — and the disparities had grown over time.
The short-term health-care plans — a.k.a. “junk” plans — that the Trump administration expanded also contribute to the problem of underinsurance. They often have low premiums but do not cover preexisting conditions or basic services like emergency health care.
Fortunately, proposals like Biden’s that make health care more accessible also tend to address the problem of underinsurance, at least in part. For example, to make individual-market insurance more affordable, Biden proposes expanding the tax credits established under the ACA. His plan calls for removing the cap on financial assistance, now set at 400 percent of the federal poverty level, in the insurance marketplaces and lowering the statutory limit on premiums to 8.5 percent of income (from nearly 10 percent).
The president also proposes to peg the size of the tax credits that subsidize premiums to the best plans on the marketplaces, the “gold” plans, rather than “silver” plans. This would increase the size of these credits, thereby making it easier for Americans to afford more-generous plans with lower deductibles.
The most ambitious Biden proposal is a public option, which would create a Medicare-like offering on marketplaces, available to anyone.Pairing this with allowing any American to opt out of their employer plan if they found a better deal on HealthCare.gov or their state marketplace — which they can’t now — would help some people escape high-deductible plans. The public option would also eliminate premiums and involve minimal to no cost-sharing for low-income enrollees — especially helpful for uninsured (and underinsured) people in states yet to expand Medicaid.
Given political realities, however, this policy may not see the light of day. So it would be best to target underinsurance directly. Most people with high-deductible plans get them through an employer. Yet unlike in the marketplace plans, the degree of cost sharing in these employer plans is the same for low-income as well as high-income employees. To deal with that problem, the government could offer incentives for employers to expand the scope of health services they cover — even in high-deductible plans. Already, many such plans exempt from the deductible some primary-care visits and generic-drug prescriptions. The list could grow to include follow-up visits and certain specialist care.
Instead of encouraging health savings accounts, the government could offer greater pretax incentives that encourage employers to absorb some of the costs that they have shifted onto their lower-income employees; that would help to prevent the insurance equity gap from widening further. The government could compensate employers that cover co-pays or other costs for their low-income employees. It could also subsidize employers that move away from high-deductible plans, at least for lower-income people.
Health insurance is complicated: More-affordable premiums are good only if they don’t bring stingy coverage. Greater investment in well-trained (and racially diverse) “navigators” — the people who help Americans enroll in plans on the federal marketplace, for example — would make it less likely that consumers would choose high-deductible plans without grasping their downsides. But it’s also important that people have options beyond risky high-deductible coverage.
The ACA expanded coverage dramatically — but the government needs to make sure that coverage amounts to more than an unused insurance card.
In this last episode of our six-part series on vaccinations, supported by the National Institute for Health Care Management Foundation, we cover vaccine development – particularly in the context of the current global pandemic. We discuss the timeline of Covid-19 vaccine development and the mRNA vaccine approach.
The following, which originally appeared on the Drivers of Health blog, is authored by Luke Testa, Program Assistant, The Harvard Global Health Institute.
In 2018, a short video circulated on WhatsApp claiming that the MMR vaccine was designed by Indian Prime Minister Narendra Modi to stop the population growth of Muslims. Subsequently, hundreds of madrassas across western Uttar Pradesh refused to allow health departments to vaccinate their constituents.
In 2020, a three-minute video claiming that the coronavirus vaccination campaign was secretly a plan by Bill Gates to implant trackable microchips in people wasone of the most widely shared pieces of misinformation online. Alongside a torrent of online COVID-19 vaccine falsehoods and conspiracy theories, sources of medical mis- and disinformation are fostering distrust in COVID-19 vaccines, undermining immunization efforts, and demonstrating how poor information is a determinant of health.
Medical misinformation, referring to inaccurate or unverified information that can drive misperceptions about medical practices or treatments, has flooded the infosphere (all types of information available online). Examples can vary from overrepresentations of anecdotes claiming that complications occurred following inoculation to misinterpretations of research findings by well-meaning individuals.
Considering the many ways in which medical misinformation can shape health behaviors, researchers at the Oxford Internet Institute recently suggested that the infosphere should be classified as a social determinant of health (SDOH) (designated alongside general socioeconomic, environmental, and cultural conditions). This classification, they argue, properly accounts for the correlation between exposure to poor quality information and poor health outcomes.
The connection between information quality and health has been especially pronounced during the COVID-19 pandemic. A 2021 study found that amongst those who indicated that they would definitely take a COVID-19 vaccine, exposure to misinformation induced a decline in intent of 6.2% in the U.K. and 6.4% in the U.S. Further, misinformation that appeared to be science-based was found to be especially damaging to vaccination intentions. These findings are particularly concerning considering the fact that during the pandemic, the 147 biggest anti-vaccine accounts on social media (which often purport to be science-based) gained 7.8 million followers in the first half of 2020, an increase of 19%.
During an unprecedented health crisis, medical misinformation within the infosphere is leaving both individuals and communities vulnerable to poor health outcomes.Those who are unvaccinated are at a higher risk of infection and increase the likelihood of community transmission. This places undue burden on those who cannot get vaccinated—due to inequities and/or preexisting conditions—and increases opportunities for variants to continue to mutate into more infectious and/or deadly forms of the virus. Poor quality information within the infosphere is undermining immunization efforts and threatens to prolong the ark of the pandemic.
Leveraging Healthcare Provider Influence in the Battle Against Poor Quality Information
Healthcare providers are uniquely suited to respond to this challenge. Throughout the pandemic, majorities of U.S. adults have identified their doctors and nurses as the most trustworthy sources of information about the coronavirus. In fact, 8 in 10 U.S. adults said that they are very or somewhat likely to turn to a doctor, nurse, or other healthcare provider when deciding whether or not to get a COVID-19 vaccine.
This influence is especially pertinent considering the state of vaccine resistance across the globe. In March 2021, a Kaiser Family Foundation poll found that 37% of U.S. respondents indicated some degree of resistance to vaccination. If that percentage of Americans remain unvaccinated, the country will be short of what is needed to achieve herd immunity (likely 70% or more vaccinated). Similar levels of resistance to vaccination remain high in countries across the globe, such as Lebanon, Serbia, Paraguay, and France.
Although medical misinformation is contributing to high rates of refusal, it is important to note that drivers of vaccine resistance are complex and intersectional. Vaccine distrust or refusal may be rooted in exposure to anti-vaccine rhetoric, racial injustice or medical exploitation in healthcare, fears that vaccine development was rushed, and/or other drivers. For this reason, responses must be tailored to unique individual or communal motivations. For example, experts have pressed the critical need for vaccine distrust within Black communities to be approached not as a shortcoming of community members, but as a failure of health systems to prove themselves as trustworthy.
With regard to resistance rooted in anti-COVID-19 vaccine misinformation, healthcare providers are leveraging their unique influence through novel, grassroots approaches to encourage vaccine uptake. In North Dakota, providers are recording videos and sending out messages to their patients communicating that they have been vaccinated and explaining why it is safe to do the same. On social media, a network of female doctors and scientists across various social media pages, such as Dear Pandemic (82,000 followers) and Your Local Epidemiologist (181,000 followers), are collaborating to answer medical questions, clear up misperceptions about COVID-19 vaccines, and provide communities with accurate information about the virus. Similarly, the #BetweenUsAboutUs online campaign is elevating conversations about vaccines with Black doctors, nurses, and researchers in an effort to increase vaccine confidence in BIPOC communities.This campaign is especially critical considering the fact that BIPOC communities are often the target of anti-vaccine groups in an effort to exploit existing, rational distrust in health systems.
In addition to these timely responses, evidence-based interventions offer promising opportunities for healthcare providers to improve vaccine uptake amongst their patients.For example, there is a growing consensus around the practice of motivational interviewing (MI).
MI is a set of patient-centered communication techniques that aim to enhance a patient’s intrinsic motivation to change health behaviors by tapping into their own arguments for change. The approach is based on empathetic, nonjudgmental patient-provider dialogue. In other words, as opposed to simply telling a patient why they should get vaccinated, a provider will include the patient in a problem-solving process that accounts for their unique motivations and helps them discover their own reasons for getting vaccinated.
When applying MI techniques to a conversation with a patient who is unsure if they should receive a vaccine, providers will use an “evoke-provide-evoke” approach where they will ask patients: 1) what they already know about the vaccine; 2) if the patient would like additional information about the vaccine (if yes, then provide the most up to date information); and 3) how the new information changes how they are thinking or feeling about vaccination. During these conversations, the MI framework encourages providers to ask open-ended questions, practice reflective listening, offer affirmations, elicit pros and cons of change, and summarize conversations, amongst other tools.
Numerous studies show motivational interviewing to be effective in increasing vaccine uptake. For example, one randomized controlled trial found that with parents in maternity wards, vaccine hesitancy fell by 40% after participation in an educational intervention based on MI. Given its demonstrated effectiveness, MI is likely to help reduce vaccine hesitancy during the COVID-19 pandemic.
With infectious disease outbreaks becoming more likely and resistance to various vaccines increasing across the globe, continuing to leverage healthcare providers’ unique influence through grassroots campaigns while honing motivational interviewing skills as a way to combat mis- and disinformation in the infosphere may prove critical to advancing public health now and in the future.
Part five of our six-part series on vaccinations, supported by the National Institute for Health Care Management Foundation, continues to explore the history of societal backlash against vaccination, with particular attention to vaccine-adjacent incidents and misinformation.
Part four of our six-part series on vaccinations, supported by the National Institute for Health Care Management Foundation. It turns out, people have been resistant to the idea of vaccines pretty much since vaccines were invented. This video explores the history of anti-vaccine sentiments, vaccine legislation, and societal backlash.