Following rumors of a potential merger reported last month by the Wall Street Journal, the paper shared this week that Bloomfield, CT-based Cigna is no longer pursuing an acquisition of Louisville, KY-based Humana.
According to insiders, the $140B merger was scuttled when the two health insurance giants couldn’t agree on price and other terms.
Instead, Cigna announced that it will be focusing on smaller, bolt-on acquisitions, and is reportedly still considering divesting its Medicare Advantage business.
Cigna also announced $10B of stock buybacks to assuage shareholders, who reacted negatively to the rumored deal, dropping the company’s stock price by nearly 10 percent since merger rumors surfaced.
The Gist: While there are several reasons why this deal may have been called off—Wall Street’s adverse reaction, antitrust concerns, leaking of the talks before the parties were ready—this likely isn’t the end of either payer’s pursuit of greater scale, as both stand in UnitedHealth Group’s giant shadow.
Given Cigna and Humana have each had potential mergers with other payers blocked by the courts, and federal antitrust scrutiny is only increasing, we’re wondering if each may be also looking at nontraditional partners (as Humana explored with Walmart in 2018), though the universe of companies with an interest in a vertically-integrated insurance and care business—and deep enough pockets—is small.
The nation’s largest for-profit hospital systems by revenue — HCA Healthcare, Community Health Systems, Tenet Healthcare and Universal Health Services —reported mixed results during the third quarter of 2023, despite announcing strong demand for patient services.
With the exception of HCA, each operator reported lower profits in the third quarter compared with the same period last year. Health systems CHS and HCA reported earnings that fell short of Wall Street expectations for revenue.
Major operators posted declining profits in the third quarter compared to the same period in 2022
Q3 net income in millions, by operator
Health System
Profit
Percent Change YOY
Community Health Systems
$−91
−117%
HCA Healthcare
$1,800
59%
Tenet Healthcare
$101
−23%
Universal Health Services
$167
−9%
Admissions rose across the board compared to the same period last year: Same facility equivalent admissions rose4.1% at HCA , 3.7% at CHS and 0.6% at Tenet,and adjusted admissions at acute hospitals rose 6.8% at UHS.
Although the for-profit operators began cost containment strategies earlier this year — recognizing that rising expenses, including costs of salary and wages, were pressuring hospital profitability post-pandemic — expenses also rose, with growth in salaries and benefit costs once again pressuring most operators’ revenue.
Hospital operators faced new challenges this quarter, executives said, including increased physician staffing fees and what hospital executives characterizedas aggressive behavior from payers.
Hospitals highlight rising physician fees
Rising physician fees were a topic of concern on earnings calls this quarter, with executives reporting fees that were 15% to 40% higher compared with the same period last year.
Third-party staffing firms charge hospitals physician fees, a percentage of physicians’ salaries, on top of the salaries themselves. Physician fees are separate but related to contract labor costs, which plagued hospitals during the COVID-19 pandemic as they attempted to stem staffing shortages.
Hospitals typically contract specialty hospitalist roles — like anesthesiologists, radiologists and emergency department physicians — and incur associated staffing costs.
Physician fees at HCA, the country’s largest hospital chain, grew 20% year over year in the third quarter, according to CFO Bill Rutherford.
Physician fees were up by as much as 40% at UHS — making up 7.6% of totaloperating expenses this quarter and surpassing the company’s initial projections for the year,CEOMarc Miller said during an earnings call. Historically, physician fees accounted for about 6% of UHS’ total expenses.
Likewise, Franklin, Tennessee-based CHS attributed some of its third-quarter losses to “increased rates for outsourced medical specialists,” according to a release on the operator’s earnings.
Tenet CEO Saum Sutaria noted that physician fee expenses were up 15% year over year, but said on an earnings call that the operator had spied rising physician fees during the pandemic, and had begun efforts to contain costs — including restructuring staffing contracts and in-sourcing critical physician services.
As a result, physician fee costs at Tenet had remained “relatively flat” from the second quarter to the third quarter this year, according to the Sutaria.
Physician fee increases may be a delayed consequence of the No Surprises Act, which went into effect in January of last year, experts say.
On an earnings call, UHS CFO Steve Filton said “the industry has largely had to reset itself” in wake of the law. Tenet and CHS executives echoed the sentiment, noting that the law had disrupted staffing firms’ business models and complicated payment processes.
The No Surprises Act prevents patients who unknowingly receive out-of-network care at an in-network facility from being stuck with unexpectedbills. However, the act has had unintended ripple effects, experts say.
Staffing firms and hospitals allege that the arbitration process created to resolve disputes between providers and insurers is unbalanced and incentivizes insurers to withhold reimbursement for care. In an August survey, over half of doctors reported insurers have either ignored decisions made by arbitrators or declined to pay claims in full.
In other cases, a backlog prevents claims from being adjudicated at all. Last year, the CMS found the federal arbitration process had only reached a payment determination in 15% of cases. Federal regulators have been forced to pause and restart the arbitration process multiple times in the wake of federal court decisions challenging arbitration methodology.
Although the act went into effect more than a year ago, many hospitals are just now feeling the strain, saidLoren Adler, associate director at the Brookings Institute’s Schaeffer Initiative on Health Policy.
That’s because most insurers, hospitals and medical groups operate on three-year contracts, according to Adler. Staffing firms, which have struggled since the No Surprises Act was enacted, have passed on costs to hospitals as contracts come up for negotiation and insurers charge firms higher rates.
In the face of rising costs, some hospitals may opt to follow Tenet and CHS and in-source physicians — either to retain contracts with physicians who worked with firms that have folded or because the passing of the No Surprises Act makes outsourcing less attractive.
CHS hired 500 physicians from staffing firm American Physician Partners after the company collapsed in July. CFO Kevin Hammons said on an earnings call that hiring the physicians had saved CHS “approximately $4 million sequentially compared to the subsidy payments previously paid” to the staffing firm.
However, in-sourcing may not be an effective cost containment strategy for all operators. HCA reported it was hemorrhaging money following its first-quarter majority stake purchase of staffing firm Valesco, which brought about 5,000 physicians onto its payroll. HCA CEO Sam Hazen said the system expects to lose $50 million per quarter on the venture through 2024, citing low payments as the primary issue.
Payer problems
Hospital executives also tied quarterly losses to aggressive behavior from insurers during third-quarter earnings calls.
UHS executives said payers were improperly denying high volumes of claims and disrupting payments to its hospitals, with UHS’ Miller characterizing insurers as “increasingly aggressive” during the third quarter. Though insurers had reduced their number of claims audits, denials and patient status changes during the early stages of the pandemic, payers were increasing denials and reviews, according to UHS’ Filton.
Tenet’s Sutaria said that claims denials were “excessive and inappropriate” during a third-quarter earnings call, adding that the hospital system was working to push back on the volume of claims denials.
Their number one strategy is to provide “excellent documentation” to refute denials quickly, Sutaria said.
Still, excessive claims denials can drive up administrative costs for hospitals, according to Matthew Bates, managing director at Kaufman Hall.
“That denial creates a lot more work, because now I have to deal with that bill two, three, four times to get through the denial process,” Bates said. “It starts to rapidly eat into the operating margins… [becoming] both a cashflow problem and an administrative costs burden.”
Executives across the four for-profit operators said they planned to negotiate with insurers to receive more favorable rates and limit the number of denials in subsequent quarters.
HCA’s Hazen said that it was important for HCA to maintain its in-network status with insurers “to avoid the surprise billing and that [independent dispute resolution] process,” but that it would work with its payers to get “reasonable rates” going forward.
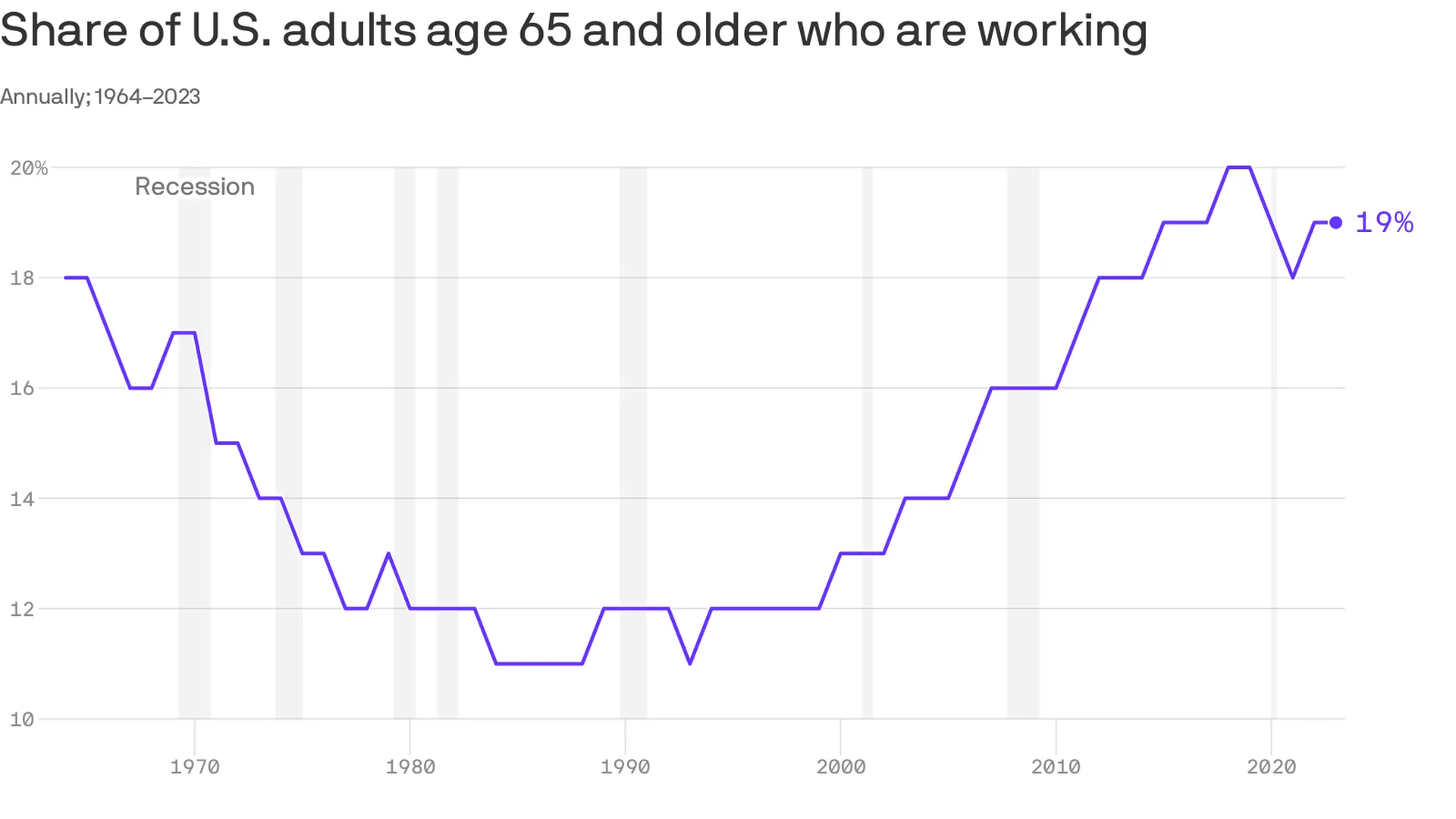
An increasing number of Americans age 65 and older are working — and earning higher wages, per a study from the Pew Research Center out Thursday.
Why it matters:
This is good for the economy, especially as the U.S. population ages — but whether or not it’s good for older Americans is a bit more subjective.
Zoom in:
The share of older adults working has been steadily increasing since the late 1980s, with a detour during the pandemic as older folks retired in greater numbers. Several forces are driving the shift:
Older workers are increasingly likely to have a four-year degree, and typically workers with more education are more likely to be employed.
Technology has made many jobs less physically taxing, so older workers are more likely to take them.
Meanwhile, changes in the Social Security law pushed many to continue working past 65 to get their full retirement benefits.
At the same time, there’s been a shift away from pension plans, which typically force people out of a job at a certain age, into 401(k) style plans that are less restrictive (and less generous, critics say).
By the numbers:
Last year, the typical 65+ worker earned $22 an hour, up from $13 (in 2022 dollars)in 1987. That’s about $3 less than the average for those age 25-64, and the number includes wages of full- and part-time workers.
Be smart:
Before Social Security existed, older people worked — a lot. In the 1880s, about three-fourths of older men were employed, said Richard Fry, senior researcher at Pew. They also didn’t live as long.
Meanwhile, the 65+ age group is a fast-growing one — by 2032 all the baby boomers will be in this category, per the BLS’s projections, and their increased workforce participation is good for an economy that is struggling with long-term labor shortages.
The big picture:
“If people are working longer because they find purpose in their jobs and want to stay engaged, that’s good for them individually,” said Nick Bunker, head of economic research at Indeed Hiring Lab.
It’s also good for the productive capacity of the economy, and the firms where they work. “Older folks have lots of experience and knowledge to pass down,” he said.
Yes, but: If there are people who want to retire, but can’t because of financial constraints, “that’s bad,” he added.
What to watch:
The share of older adults working peaked before the pandemic — will it surpass those levels?
The number hasn’t bounced back as much as anticipated partly because older Americans benefited hugely from the stock market surge and real estate gains of the past few years — and didn’t need to work anymore.
Starbucks is softening its stance toward unionization after years of pushing back.
Why it matters:
It’s a potentially huge shift for the chain and a signal of the staying power of the labor movement that surged in the wake of the pandemic.
“They know this isn’t going away,” said Nick Setyan, an equity analyst at Wedbush who covers Starbucks. He called the company’s new posture “capitulation.”
Setyan said recent worker walkouts were a turning point. Also, at least five more stores this month voted to unionize.
Zoom out:
Union organizing efforts have been a public relations headache for Starbucks since at least 2021 when a store in Buffalo became the first to vote for a union. Meanwhile, pressure from labor regulators isn’t slowing.
Zoom in:
Starbucks’ strategy shift began in March whenLaxman Narasimhan took the CEO reins from founder Howard Schultz, who had repeatedly clashed with workers over unionizing. The new CEO spoke of the need to care for customer-facing staff, per Reuters.
It’s accelerated over the past week — last Friday, Starbucks vice president Sara Kelly sent a letter to Workers United (the union that reps workers), saying the company wanted to restart bargaining.
The union has yet to bargain a contract. Starbucks now says it wants an agreement by next year.
On Wednesday, the company released an audit on its labor relations practices that was commissioned by Starbucks — after a shareholder vote forced its hand — and conducted by a former management-side lawyer.
Though the report asserted Starbucks didn’t have an “anti-union playbook,” it did find the company was unprepared to deal with its unionizing workforce and acknowledged that store managers made mistakes in how they handled the situation.
The report offers recommendations for improvement — including better training. Change starts with “tone from the top,” the audit says, suggesting that the company should reach agreements with the union “expeditiously.”
What happened:
Starbucks initially believed it could fend off unionization by messaging about best-in-class wages and benefits, Setyan said, noting that it’s true the chain offers better compensation than competitors.
“Internally, they felt kind of aggrieved,” he said, that workers who management perceived as well-compensated would want to organize.
For a while it seemed like the messaging campaign was working, but the Red Cup Rebellion walkout last month and a flurry of new union votes changed minds.
Starbucks has historically been very sensitive to public relations — and it became clear pushing back isn’t great for its image, Setyan said.
The other side:
Union representatives are skeptical of Starbucks’ new position.
“We are hopeful your letter is indeed the beginning of a sincere effort, and not a publicity move in the face of pressure from partners, Wall Street, shareholders, and others,” Workers United president Lynne Fox, said in a letter to Kelly last week.
What to watch:
If Starbucks’ change in tone is a sign that the company will finally come to terms with these workers, and agree to a contract, or just a shift in its public stance while it continues efforts to avoid a deal.
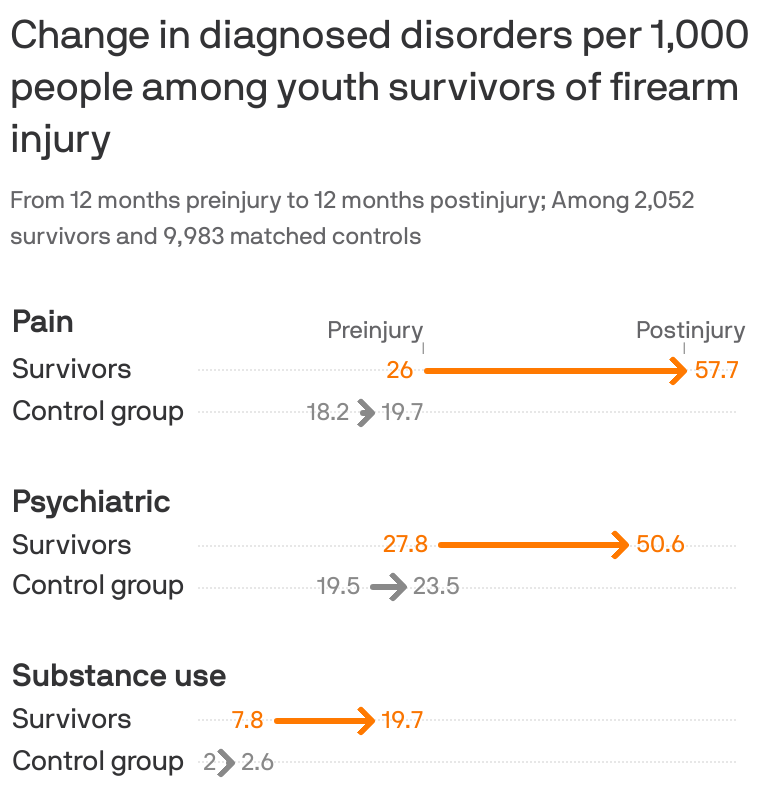
Young survivors of shootings face a litany of physical, psychiatric and substance abuse disorders that can combine to drive up their health costs almost 2,000%, according to new research.
The big picture:
Guns have become the leading cause of death among kids, but many more survive being shot. Their needs offer a rare and detailed look at the cumulative consequences of gun violence and the burden it places on survivors, their families and the health system.
By the numbers:
Using a trove of claims data for employer-sponsored insurance, researchers in Health Affairs compared over 2,000 child and adolescent shooting survivors and 6,000 family members with much larger control groups that did not suffer gun injury between 2007-2021.
In the year after being shot, survivors had a 117% increase in pain disorders including musculoskeletal pain and headaches compared with the control group, with a 293% increase for those more severely wounded.
There was a 68% increase in psychiatric disorders, such as PTSD and mood disorders, with a 321% increase among those with worse injuries.
Substance use disorders rose 144% percent — and cases rose regardless of the severity of the injury.
Emergency room visits for gun injuries among kids doubled during the pandemic, according to separate research published Monday in Pediatrics.
There is also an impact on families’ mental health and even the types of care they got in the aftermath of a child surviving a shooting, researchers found in the Health Affairs study.
Diagnosed psychiatric disorders among mothers and fathers increased by about 30% — and the increases were much larger among parents of children who died.
Mothers had a 75% increase in mental health visits, while other routine care like office visits and lab tests declined slightly for themselves and the siblings of survivors.
That was consistent with a “crowding out” effect when more acute health care needs arise, researchers said.
What they’re saying:
“Our study shines light on the substantial effects incurred not just directly by victims and survivors of gun violence, but indirectly by parents and siblings who, we found, often relinquish their own routine health care to the more acute health needs of the family,” senior study author Chana Sacks, co-director of the MGH Gun Violence Prevention Center, said in a statement.
Survivors’ health care costs also soared 17-fold to nearly $35,000 on average over the course of a year. Two-thirds of the cost was in the first month after being shot, while survivors used more health care across the board — including more visits to doctor’s offices, ER trips, imaging and mental health services.
Insurers covered the vast majority of the care, but families were on hook for about 5% of the cost.
Between the lines:
Researchers looked at claims data for workplace health insurance only, so the results don’t include kids without insurance or those enrolled in Medicaid — a major source of coverage, especially for children of color.
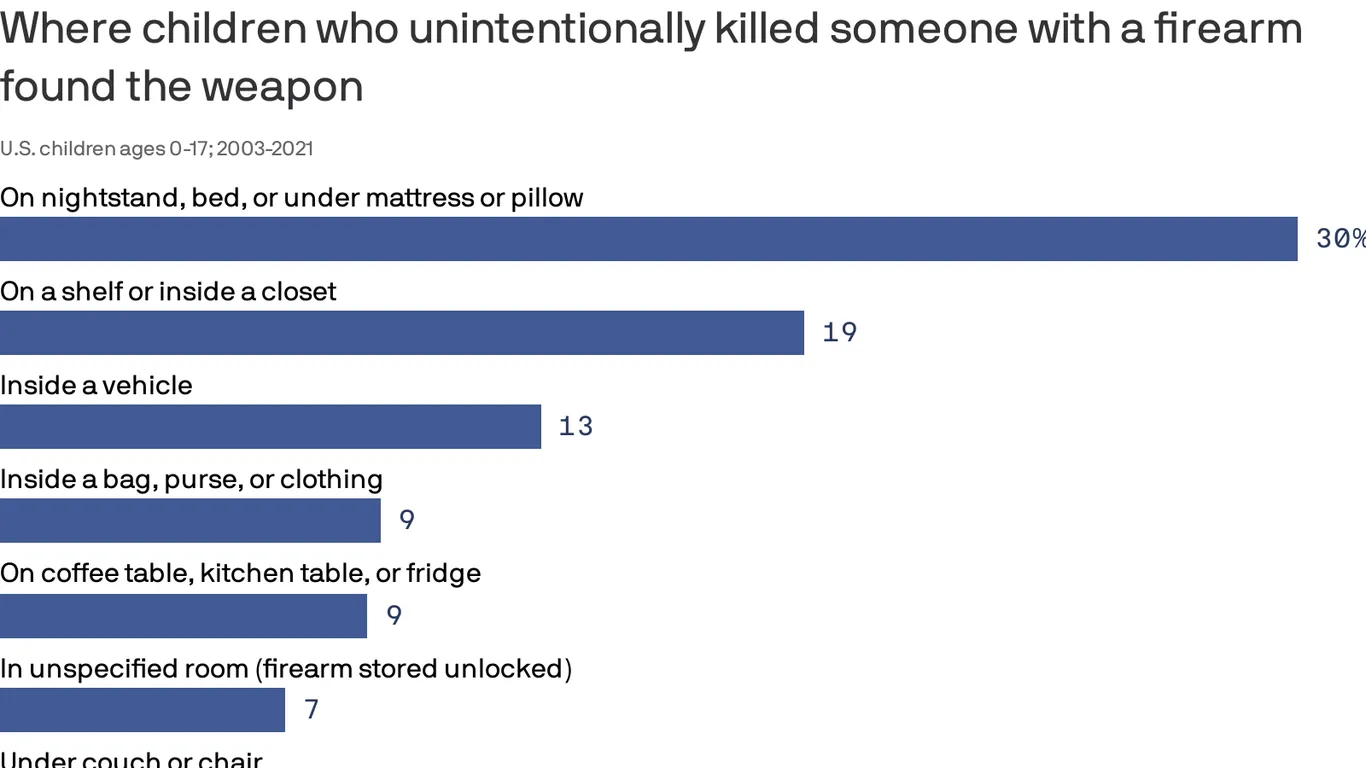
Children and teens involved in unintentional fatal shootings most commonly found the gun inside or on top of a nightstand, under a mattress or pillow, or on top of a bed, according to a new federal study.
Why it matters:
The data from the Centers for Disease Control and Prevention, which covers nearly 20 years of deadly firearm accidents among America’s youth, demonstrates why putting a gun out of sight or out of reach is not “safe storage,” federal researchers said.
It underscores the need for policymakers, health experts and parents to promote safe gun storage, they said.
Using data recorded between 2003 and 2021 by the National Violent Death Reporting System, researchers identified more than 1,250 unintentional gun deaths among kids.
The vast majority involved guns that were unlocked (76%), and most of those unlocked firearms were also loaded (91%).
Two-thirds (67%) of unintentional gun injury deaths among kids occurred when the shooter was playing with the gun or showing it to others.
In 30% of deaths, guns were found around nightstands and other sleeping areas.
Guns were also most commonly found on top of a shelf or inside a closet (18.6%) or inside a vehicle (12.5%).
A Los Angeles jury awarded $41.49 million to a former nurse who said Kaiser Permanente’s hospitals and health plan retaliated against and eventually terminated her for raising issues with patient safety and care quality, MyNewsLA reported Dec. 12.
The former nurse, Maria Gatchalian, was awarded $11.49 million in compensatory damages, including $9 million for emotional distress, and $30 million in punitive damages.
“We stand by her termination and are surprised and disappointed in the verdict,” Murtaza Sanwari, senior vice president and area manager for Kaiser Permanente Woodland Hills/West Ventura County, told Becker’s in a statement. “Kaiser Permanente plans to appeal this decision and will maintain our high standards in protecting the health and safety of all our patients.”
Before her termination in 2019, Ms. Gatchalian had worked at the Kaiser Permanente Woodland Hills Medical Center since 1989, first as a registered nurse in the neonatal intensive care unit and later as a charge nurse in that unit.
According to MyNewsLA, Ms. Gatchalian said she had repeatedly raised concerns with Kaiser management about patient safety and care quality related to alleged understaffing and was discouraged from submitting formal complaints. Oakland, Calif.-based Kaiser argued in court that Ms. Gatchalian admitted she had placed her bare feet on equipment in the NICU, and the organization made the decision to terminate her following her conduct.
“We work hard to make Kaiser Permanente a great place to work and a great place to receive care,” Mr. Sanwari said. “The allegations in this lawsuit are at odds with the facts we showed in the courtroom.”
“To be clear, this charge nurse’s job was to be a leader for other nurses, ensure the standards of care were followed and to protect the neonatal babies entrusted to our care. She was terminated in 2019 following an incident where she was found sitting in a recliner in the neonatal intensive care unit, on her personal phone and resting her bare feet on an isolette with a neonatal infant inside. Neonatal intensive care units are critical care units designed for critically ill babies most often born prematurely and very susceptible to infections.
The isolette, where this nurse placed her bare feet, is a protective environment designed to shield the infant from infection causing germs. Placing her bare feet on the isolette may have created risk to the infant which could have been life threatening. Her actions were egregious and in violation of our infection control policies and standards.”
Board members are a professional group less often linked to the chronic exhaustion and emotional fatigue of burnout. But governing bodies are now increasingly feeling the strain, Fortune reports.
Board members are noting longer meetings, more rigorous prep work, and more frequent calls between meetings, according to Fortune, which spoke with a Korn Ferry partner who is hearing talk of board-level exhaustion “everywhere.”
One contributing factor to boards’ burnout is C-level turnover. As CEOs and C-suite leaders exit organizations, boards are forced to step up and take on a wider range of issues, Fortune reports. In healthcare, CEO changes have ticked upward. U.S. hospitals saw 126 CEO exits through the first 10 months of the year, a 62 percent increase from the same time period in 2022.
Increased rigor that board members now face in their responsibilities could also signal a change is due in how professionals think about board service.
The founder and CEO of a membership organization for executive women told Fortune that the traditional model of boards being a “last hurrah” before an executive’s retirement is not fit for the current demands and changes, such as the addition of more board members or limiting the number of board seats that someone can hold, may be needed.
Experts told Fortune that board leaders ought to check in with individual members to clarify the workload of serving on the body and acknowledge how the job has changed. This may be particularly crucial in healthcare, where fewer than 15% of board members overseeing the nation’s top hospitals have a professional background in the industry.
Before the growing issue of burnout, boards have long grappled with passive and disengaged members. Here are 10 signs of a board member who is effectively governing and adding value.
Great systems are usually governed by great boards, who are made up of people who match the following 10 descriptions.
Great board members do more than comply with corporate governance structure and rules. Too often, board members have loose ties to one another, are passive to the wants and views of the CEO or are not as informed about the specifics of healthcare as they ought to be. We view all of these traits, and more, as signs that a board has lost its charge and is no longer effectively governing.
We consider the following 10 items as descriptors of a board member who has a strong pulse and adds value to a governing body.
1. The board member is active, engaged and passionate about being a board member. No board can afford to have disengaged members. Bylaws and attendance requirements are important, but simply complying with them does not necessarily equate to being an active, contributing and passionate trustee. Engaged board members show up to meetings, and they show up prepared. While members typically refrain from meddling in day-to-day operations, boards with high levels of trust and candor make a point to communicate with the CEO outside of scheduled board meetings. Quality of board engagement is an important contributing factor to board performance, and there is a correlation between board engagement and the ability to attract board members. Everything that follows is dependent on board engagement.
2. The board member has a point of view on what the organization must be great at, and the board member is vehement about it. Health systems cannot be all things to all people, although the opportunities to attempt this are ample. The best organizations are not static, but disciplined. Well-governed systems know the specialties they are great in, and they continue to double down on their strengths. Their boards are cognizant of where revenues come from and ensure resources are allocated accordingly.
3. The board member realizes that her top job is to ensure the system has great leadership in place. Leaders can fall short in all sorts of ways, some more visible and easily detectable than others. The active, engaged and vehement board does not easily accept disappointment. Boards have many steps at their disposal to manage a problem before firing a CEO or senior leader, but they should never function in a way where termination is unthinkable. Boards cause great damage when they tolerate mediocre performance or compromised values among people at the top of the organization.
4. The board member understands accountability for patient safety and quality of care rests firmly in the boardroom. It rests on board members to insist that they receive sufficient, timely information about patient safety and care quality from the CEO. It rests on board leadership to ensure members have access to expertise and resources to properly obtain, process and interpret this information. It is not a bad idea for quality expertise to be included in board members’ competency profiles and for boards to undergo training and continued education in quality and safety. This is especially relevant for board members who come from industries outside of healthcare. It rests on the board when care quality declines or when lapses in patient safety are unaddressed: It is unacceptable for a board to say it missed the memo on care outcomes or that it did not understand the information in front of it.
5. The board member is a watchdog on societal, governance and audit issues. Informed citizens make for strong board members. It is important to not only be plugged in and aware of the issues and challenges confronting the organization today, but to be aware of broader societal issues that could affect system strategy and performance tomorrow. This is not hypothetical thinking. The past year was a master class in how broader issues affected healthcare in acute and direct ways: systemic racism, a global supply chain and a churning labor market are just three. Good boards are made up of members who stay informed and are biased toward anticipatory thinking, in which they are eager to explore the ways in which issues larger than or outside of their industry may come to affect the organization they help govern.
6. The board member supports the leadership team, but also questions it and holds it accountable. Board members cannot be pushovers for leadership. Directors are nominated by existing board directors on the nominating committee, which often includes the CEO. As a result, trustees can empathize with the CEO of the organization on whose board they sit. Empathy does not equate to blind acceptance, but this is nonetheless a dynamic trustees should be aware of and work to keep in check. It is not unusual for board members to struggle when giving candid feedback to the CEO, for example. As a result, chief executives carry on and live in a bigger and bigger bubble.
It’s worth noting that the reverse can occur within boardrooms as well, in which board members disagree about strategy and seek a CEO they can easily influence. At the end of the day, being a pushover is not associated with strong leadership and should be avoided by both trustees and senior executives. Instead, trustees need to embrace constructive tension in the boardroom. Questions, challenges and disagreements that reach resolution can drive valuable dialogue and stronger outcomes.
7. The board member allows others to voice their thoughts. In many boardrooms, a small number of the participants do most of the talking while the majority stays relatively quiet. A powerful or well-connected member may dominate discussions. Ideally, boards embrace the middle in interpersonal communication, with trustees contributing not too much nor too little. Either goes against the board’s very reason for being.
8. The board member helps ensure the board as a whole reflects the racial, ethnic, gender, religious and socioeconomic diversity of the community served by the organization. This is important for a number of reasons, with health equity being principal. Trustees are stewards for the communities they serve. For hospitals and health systems to increase opportunities for everyone to be healthier — including those who face the greatest obstacles — they need visions, strategies and goals that begin at the top from individuals who have viewpoints from the community. Without these insights, the board simply can’t govern effectively. Additionally, research has consistently found that teams of people who have diversity in knowledge and perspectives — as well as in age, gender and race — can be more creative and better avoid groupthink.
9. The board member is accessible. Just as no board wants its CEO in a bubble, governing bodies must actively resist this risk. For a stretch of time, boards were less visible groups of people who would meet four to six times a year in a mahogany-paneled room to decide the future of an organization that employs tens of thousands and serves even more. This dynamic cannot hold in healthcare. Community members and employees should know — or be able to easily learn — who serves on their health system’s board. If stakeholders bring issues or concerns to a board member, the trustee should be prepared to respond and follow up. In 2021’s healthcare, board members cannot breathe rarified air.
10. The board member emulates the values of the health system. So often when people talk about the tone being set at the top, they have the CEO in mind. The board is just as responsible, if not more responsible, for this charge. What a board permits, it promotes. Board members that emulate system values are better positioned to collaborate with mutual respect, candor and trust. Board members whose values are mismatched or personal agendas are at cross-purposes with the good of the organization should be replaced.