Verity Health System announced Jan. 6 that it plans to close St. Vincent Medical Center, a 366-bed hospital in Los Angeles.
El Segundo, Calif.-based Verity entered Chapter 11 bankruptcy in August 2018 and is seeking bankruptcy court approval to close St. Vincent Medical Center. The nonprofit health system is shutting down St. Vincent after a deal to sell four of its hospitals fell through.
Corona, Calif.-based KPC Group bid $610 million in January 2019 to acquire four hospitals from Verity, and the bankruptcy court approved the asset purchase agreement three months later. In early December, KPC’s Strategic Global Management missed the court-appointed deadline to purchase the hospitals.
In December, SGM appealed the court’s order setting the closing deadline. About one month later, Verity filed a lawsuit against KPC Group and its affiliates, alleging “intentional and misleading conduct” and breach of the asset purchase agreement, according to the Los Angeles Times.
The bankruptcy court will consider Verity’s request to close St. Vincent later this week. The health system said arrangements have already been made to transfer patients and specialty services to nearby facilities.
“We are deeply saddened to announce the planned closure of St. Vincent Medical Center,” Verity Health CEO Rich Adcock said in a news release. “This decision has not been taken lightly and comes only after exhausting every option to keep this hospital open.”
The closure of St. Vincent will not affect Verity’s other three hospitals in California: St. Francis Medical Center in Lynwood, Seton Medical Center in Daly City, and Seton Coastside in Moss Beach.
Since 2005, 162 rural hospitals have shuttered, with 60% of the closures occurring in southern states that did not expand Medicaid enrollment.
KEY TAKEAWAYS
19 rural hospitals closed in 2019, up from 15 closures in 2018, and continuing a steady double-digit trend in closures since 2013.
Most hospitals closed because of financial problem, and 38% of rural hospitals are unprofitable.
Patients in communities affected by closure travel 12.5 miles on average for care. However, 43% of the closed hospitals are more than 15 miles to the nearest hospital, and 15% are more than 20 miles.
Despite a booming national economy, 2019 was the worst year for hospital closings since at least 2005.
The North Carolina Rural Health Research Program says that 19 rural hospitals closed this year, up from 15 closures in 2018, and continuing a steady double-digit trend in closures since 2013.
Since 2005, the North Carolina researchers tracked 162 hospital closings, with 60% of the closures occurring in southern states that did not expand Medicaid enrollment.
Texas led the way, with 23 hospital closures since 2005, followed by Tennessee with 13, and North Carolina with 11.
The closures have been blamed on a number of factors, including: the older, sicker, poorer, and less-concentrated rural demographic; bypassing by local residents seeking care at regional hospitals; hospital consolidation; value-based care; referral patterns of larger hospitals; the transition to outpatient services; and mismanagement.
Among the findings highlighted by the North Carolina Rural Health Research Program:
More than half of the rural hospitals that close cease to provide any type of health care, which were define as abandoned.
Most closures and “abandoned” rural hospitals are in South (60%), where poverty rates are higher, people are generally less healthy and less likely to have public or private health insurance.
Most hospitals closed because of financial problems. 38% of rural hospitals are unprofitable.
In 2016, 1,375 acute care hospitals out of 4,471 urban and rural acute care hospitals (31%) were unprofitable, including 847 rural hospitals (versus 528 unprofitable urban hospitals).
Patients in communities affected by closure travel 12.5 miles on average for care. However, 43% of the closed hospitals are more than 15 miles to the nearest hospital, and 15% are more than 20 miles.
The typical rural hospital employs about 300 people, serves a community of about 60,000. When the only hospital in a county closes, there is a decrease of about $1,400 in per capita income in the county.
University of Minnesota research shows that between 2004 and 2014, 179 rural counties lost all hospital-based OB services.
Over the last 15 years, the difference in mortality between rural and urban areas has tripled – from a 6% difference to an 18% difference in 2015.
The Rural Health Model, the first of its kind, creates an alternative payment model that transitions hospitals from fee-for-service to global budget payments.
KEY TAKEAWAYS
The Rural Health Model creates an alternative payment model that transitions hospitals from fee-for-service to global budget payments.
Instead of getting paid for admissions, hospitals in the model will get a preset amount of money to provide services in the community.
State officials say the new payment model allows hospitals time to transform care to better meet the health needs of the community.
Eight more hospitals and one payer have joined a Pennsylvania initiative to shore up the financial footing of the state’s rural hospitals.
“I am especially pleased to see more hospitals joining this important initiative to improve their financial viability so that every Pennsylvanian has access to quality health care within a reasonable distance from home,” Gov. Tom Wolf said in a media release.
State officials the program is needed because nearly half of all rural hospitals in Pennsylvania are operating with negative margins and are at risk of closure. Four rural hospitals in Pennsylvania have shuttered since 2006, according to the North Carolina Rural Health Research Program.
The Rural Health Model, the first of its kind, creates an alternative payment model that transitions hospitals from fee-for-service to global budget payments. Those global payments come from several payers, including private and public insurers.
Instead of getting paid for admissions, hospitals in the model will get a preset amount of money to provide services in the community.
State officials say the new payment model allows hospitals time to transform care to better meet the health needs of the community. This includes providing nontraditional roles, such as providing transportation and broadband internet access.
The eight hospitals are:
• Armstrong County Memorial Hospital in Kittanning.
• Chan Soon-Shiong Medical Center at Windber in Somerset County.
• Fulton County Medical Center in McConnellsburg.
• Greene Hospital in Waynesburg, Greene County.
• Monongahela Valley Hospital in Monongahela, Washington County.
• Punxsutawney Area Hospital in Punxsutawney, Jefferson County.
• Tyrone Hospital in Tyrone, Blair County.
• Washington Hospital in Washington, Washington County
A total of 67 hospitals are eligible for model based and nearly 20% of them will participate in in 2020, state officials said.
In addition, Aetna will join five other private payers – Gateway, Geisinger, Highmark, Medicare and UPMC – which combine make up nearly half of the individual and small group market insurance population in the state.
The program is funded and administered by the newly created Rural Health Redesign Center Authority and the Pennsylvania Rural Health Redesign Center Fund.
In addition to providing access to care for rural communities, state officials say the model will ensure that, by remaining open, rural hospitals continue to be a vital economic driver for their communities.
“The Rural Health Model is a transformative step that changes the financial model for hospitals in rural areas,” said Pennsylvania Secretary of Health Rachel Levine, MD. “This is a step that will help achieve financial stability for these facilities and aims to improve the overall health of the community.”
“THIS IS A STEP THAT WILL HELP ACHIEVE FINANCIAL STABILITY FOR THESE FACILITIES AND AIMS TO IMPROVE THE OVERALL HEALTH OF THE COMMUNITY.”
RACHEL LEVINE, MD, PENNSYLVANIA SECRETARY OF HEALTH
The Hospital and Healthsystem Association of Pennsylvania report found that hospitals also supported more than one in every 10 jobs.
Hospitals in Pennsylvania made a total economic impact of $136.1 billion in Fiscal Year (FY) 2018, according to a Hospital and Healthsystem Association of Pennsylvania (HAP) report released Tuesday.
Of the total economic impact, $60.5 billion were the result of “direct impact,” such as employee salaries, benefits, as well as goods and services for hospital operations. Another $75.6 billion were the result of “ripple impact,” such as additional economic effects of a hospital in a community.
HHAP also found that hospitals supported more than 650,000 jobs, accounting for more than one in every 10 jobs in the state and providing $32.3 billion in total wages. Nearly 300,000 jobs were directly associated with hospitals while 363,000 jobs were associated with “ripple effects” of health systems.
The study’s findings point to the significant economic impact provider organizations have in the Keystone State and the need to promote policies that foster continued growth, according to Sari Siegel, PhD, vice president of healthcare research at HAP.
“While overall growth projections are strong, some hospitals remain financially stressed. Our work illustrates that hospitals often are the backbones of their communities and closure could cause devastating economic ripples throughout a region,” Siegel said in a statement. “The findings of this report underscore the need for policies that bolster hospitals’ long-term sustainability.”
Pennsylvania hospitals have contributed significantly to the state’s economy in recent years and have also made headlines throughout 2019.
Hahnemann University Hospital, a Pennsylvania-based hospital, filed for bankruptcy and closed over the summer. A group of six Philadelphia-based health systems won the hospital at auction for $55 million in early August.
The report was also released days after two Pennsylvania-based health systems, Tower Health and Drexel University, finalized a $50 million acquisition of St. Christopher’s Hospital for Children, a 188-bed pediatric medical center in Philadelphia.
There are 253 hospitals in Pennsylvania, according to HAP, with more than 37,600 staffed beds. The report also found that hospitals are among the 10 largest employers in 85% of counties across the state.
The total economic impact of Pennsylvania hospitals in FY 2018 grew by nearly $50 billion over the past decade, according to a HAP analysis of data collected from the Department of Health and Human Services (HHS).
Additionally, Pennsylvania hospitals received nearly $2 billion in research allocations from HHS and Patient-Centered Outcomes Research Institute in FY 2018.
Corona Calif.-based KPC Group missed the court-appointed deadline to purchase four hospitals from El Segundo, Calif.-based Verity Health, which entered Chapter 11 bankruptcy in August 2018.
KPC Group bid $610 million in January to purchase the four hospitals from Verity. Three months later, U.S. Bankruptcy Judge Ernest M. Robles approved the asset purchase agreement for KPC’s Strategic Global Management to acquire the hospitals. In late November, the judge ordered SGM to close the deal by Dec. 5.
After SGM failed to complete the purchase by the court-appointed deadline, Verity asked the court to issue an order requiring SGM’s principals to testify as to why the deal did not close and whether SGM has the financial ability to close the sale. Verity also asked the court to issue an order finding SGM in breach of the asset purchase agreement and allowing it to keep SGM’s $30 million deposit and proceed with other plans to sell the hospitals.
On Dec. 9, the court denied Verity’s request to force SGM’s executives to appear and testify in court.
“By failing to close, SGM risks the loss of its $30 million good-faith deposit as well as the possibility of damages for breach of contract in an amount of up to $60 million,” Judge Robles wrote in a Dec. 9 court filing. “Being compelled to offer testimony will not motivate SGM to close where the threat of the loss of up to $90 million has failed to accomplish that end.”
The judge assured Verity that it would have the chance to litigate the issues of whether SGM breached the asset purchase agreement and whether it’s entitled to keep the good-faith deposit.
Though neither party has terminated the sale process, the judge said Verity can “explore options for the alternative disposition of the hospitals” without violating the asset purchase agreement.
The next bankruptcy court hearing is slated for Dec. 30.
From reimbursement landscape challenges to dwindling patient volumes, many factors lead hospitals to close.
Here are 10 hospitals that have closed in the past four months, beginning with the most recent:
1. Dallas-based Steward Health Care closedSt. Luke’s Medical Center in Phoenix on Nov. 24. Officials said the hospital closed due to dwindling patient volumes. St. Luke’s Medical Center’s occupancy rate remained below 40 percent over the past two years, President James Flinn wrote in a letter to the local community in October.
2. Nix Medical Center, a 208-bed hospital in San Antonio, closed in November. A few months earlier, Los Angeles-based Prospect Medical Holdings said it was closing the hospital because community demand for acute care at Nix Medical Center has declined over the past year.
3. Southcross Hospital in San Antonio closed Oct. 11. The hospital and its operator, San Antonio-based Arete Healthcare, entered Chapter 11 bankruptcy in November.
4. Haskell County Community Hospital in Stigler, Okla., closed Oct. 2, according to the Cecil G. Sheps Center for Health Services Research. Haskell County Community Hospital is one of several hospitals previously owned by Kansas City, Mo.-based EmpowerHMS that filed for bankruptcy protection earlier this year.
5. Brentwood, Tenn.-based Quorum Health closedMetroSouth Medical Center in Blue Island, Ill., on Sept. 30. Quorum announced in June that it filed an application with the Illinois Health Facilities and Services Review Board to close the 314-bed hospital.
6. East Ohio Regional Hospital in Martins Ferry closed Sept. 27. The hospital’s president and CEO cited mounting financial losses as one of the factors that forced the hospital to shut down.
7. Ohio Valley Medical Center in Wheeling, W.Va., closed in September. Hospital officials said the “unwanted, yet unavoidable,” decision was made due to an unsuccessful search for a strategic partner, lack of interest from potential buyers and a more than $37 million operating loss over the last two years.
8. Hahnemann University Hospital in Philadelphia closed in early September. Hahnemann announced in June that it would close Sept. 6. The hospital pushed back the closure date after a bankruptcy judge approved the sale of its residency programs on Sept. 5.
9. Westlake Hospital in Melrose Park, Ill., closed in August, according to the Chicago Sun-Times. Los Angeles-based Pipeline Health revealed plans to close Westlake Hospital in February, a few weeks after acquiring the 230-bed hospital from Dallas-based Tenet Healthcare.
10. North Metro Medical Center in Jacksonville, Ark., closed Aug. 20, leaving local residents without an emergency room. No notice was given before the hospital shut down.
Philadelphia-based Hahnemann University Hospital’s license has been revoked, the Pennsylvania Department of Health told the judge overseeing the hospital’s bankruptcy case in a Nov. 1 letter, according to The Philadelphia Inquirer.
The license revocation comes roughly two months after the hospital closed and about four months after the hospital entered Chapter 11 bankruptcy.
Pennsylvania Secretary of Health Rachel L. Levine brought the license revocation to the judge’s attention and expressed concerns about security in the letter.
“I am bringing the current situation at Hahnemann to your attention because I am deeply concerned about the state and security of the building and the supplies and equipment it is housing,” she wrote, according to the report.
Ms. Levine said a small team has made some progress but more work needs to be done. “While I do not want to take away from the effort that they have put forth, the fact is it is just not enough.”
Among the work that needs to be done, the removal of laboratory equipment and highly flammable chemicals, the letter stated.
Healthcare costs in the U.S. are too high. Americans struggle to afford basic needs like prescription drugs and too often face crushing surprise bills after undergoing necessary medical procedures. Seniors in particular feel the weight of health expenses when they discover that the Medicare benefits they earned don’t always provide sufficient coverage.
While the Affordable Care Act instituted protections for Americans with pre-existing conditions, guaranteed essential health benefits and made some progress in lowering patients’ costs, those advancements are under attack in the courts and through regulatory actions. I chair the House Ways and Means Committee, which has jurisdiction over a great deal of our nation’s healthcare system, including Medicare. Under Democratic leadership, we are fighting to bring down healthcare costs and preserve critical existing health protections.
Our committee hit the ground running this year. The first hearing I convened as chairman focused on protecting Americans with pre-existing conditions. Nearly 130 million Americans have a pre-existing condition—anything from asthma to cancer to diabetes. Thanks to the ACA, insurance companies can no longer refuse to cover these individuals. The hearing shed light on the importance of this safeguard and the ways it provides Americans with greater peace of mind and financial security.
We also highlighted the immense pain families will endure if 18 Republican state attorneys general succeed in their case to repeal the law.
House Democrats, along with Democratic state attorneys general, jumped into this court battle and continue to defend the millions of Americans with health conditions from discrimination and financial ruin.
We also took concrete steps to increase transparency and lower drug prices. Ways and Means advanced legislation that sheds light across the healthcare supply chain—from pharmaceutical manufacturers to pharmacy benefit managers—to help reduce costs for families. More can be done. In the coming months, the committee will consider legislation to improve the Medicare Part D program, establishing an out-of-pocket cap on expenses for beneficiaries. This would lower costs for seniors and save taxpayers money.
Part D reform is just one way to improve Medicare for beneficiaries. Many seniors aren’t aware that Medicare does not cover routine vision, hearing or dental exams. I will work to change that. Helping seniors access the glasses, hearing aids or dental care they need will save them money on the front end. This coverage will also prevent the trauma and expense of falls or other related health problems that could arise down the road as a result of inadequate services.
Some of the most jarring and devastating medical costs Americans encounter are surprise medical bills. Ways and Means plans to tackle this problem too. We are crafting legislation now that will help patients avoid the huge expenses that follow inadvertently being treated by out-of-network providers.
Healthcare is a necessity and it’s a human right. Paying for it shouldn’t bankrupt families. We can lower patient costs without stifling medical innovation or throwing hospitals into turmoil. It’s possible to achieve commonsense solutions that strengthen our nation’s healthcare system while reducing the burden on consumers.
Officials at troubled drugmaker Purdue Pharma say “certain employees” should be paid more than $34 million in bonuses for meeting and exceeding goals over the last three years, even though the company is facing thousands of lawsuits over its role in the nation’s opioid crisis and earlier this week filed for bankruptcy.
In a legal filing, attorneys for Purdue Pharma asked a judge to authorize millions in payments to employees who have met “target performance goals.”
It is not clear from the company filings why employees would be eligible for bonuses, because, while the bonuses are supposed to be partly contingent on the company’s financial performance, the company has filed for bankruptcy.
At a bankruptcy court hearing in White Plains, N.Y., on Tuesday, Paul K. Schwartzberg, an attorney for the U.S. Trustee, raised objections to some of the bonuses. While it is typical for companies in bankruptcy to try to pay employees as a firm seeks to regain its financial footing, the Purdue Pharma bonuses go “way beyond” what is typical, he said.
The company is widely blamed for fueling the opioid epidemic because of allegedly misleading sales tactics it used to push physicians to prescribe millions of doses of its OxyContin painkiller. It faces thousands of lawsuits from cities, states and others affected by the opioid crisis, which claimed more than 200,000 lives in the past two decades.
“That $34 million is owed to the victims of the opioid epidemic, and every last cent should be spent on addiction science, treatment and recovery,” Connecticut Attorney General William Tong said in a statement to The Washington Post. “Purdue and the Sacklers still don’t seem to comprehend the pain and suffering they have caused. While I am sympathetic to the workers at Purdue, many of whom live in my hometown and state and had nothing to do with the egregious actions of their employer, this not business as usual.”
The attorneys for Purdue Pharma did not specify which of its 700 employees would be eligible for the bonuses, except that the incentives would not be available to “insiders” or any top executives involved in the company’s “strategic decision-making.” But other senior managers, who are often offered such incentive plans, could be eligible for the bonuses.
The number of employees eligible for the bonuses and the amounts of their rewards are unknown. But if the $34 million in bonuses were distributed equally to each of the 700 employees, each would receive about $50,000.
Company attorneys say the incentives are needed to retain key employees as it seeks to transform itself into a public trust aimed at delivering addiction remedies. Since 2018, about a quarter of the company’s “top tier” employees have left, they said.
“These employees have highly coveted skills in the industry and the company is not an easy place to work right now,” Eli J. Vonnegut, an attorney representing Purdue Pharma, said at the bankruptcy hearing. It “would be very difficult to attract new talent were the company to lose its current employees. With all the negative publicity, many employees are concerned about the economic risks that they are taking by staying at Purdue.”
The employee bonuses are part of the company’s long-standing incentive programs, according to the company. It is asking the bankruptcy court’s permission to pay out $26.5 million under its “Annual Incentive Plan,” which covers one year of company and employee performance, and another $7.9 million under its long-term rewards plan, which covers the last three years.
Under both programs, the size of the bonuses would depend on employees’ work and the company’s performance.
The company filing described the bonuses as something that employees “have come to rely on as a part of their annual compensation.”
The company is also seeking $1.5 million a month to cover anticipated legal expenses of employees. More than 270 former employees already have been witnesses or defendants in pending litigation, the company said.
U.S. Bankruptcy Judge Robert D. Drain is expected to consider the bonuses in October.
“These people are highly compensated,” Schwartzberg said. “They can wait” until then.
The number of rural hospital closures in the United States has increased over the past decade.1 Since 2010, 113 rural hospitals,2 predominantly in Southern states, have closed. This is a concerning trend, since hospital closures reduce rural communities’ access to inpatient services and emergency care.3 In addition, hospitals that are at risk financially are more likely to serve rural communities with higher proportions of vulnerable populations.4
Understanding the financial pressures facing rural hospitals is imperative to ensuring that America’s 60 million rural residents have access to emergency care.5 Rural hospitals are generally less profitable than urban ones, and those with the lowest operating margins maintain fewer beds and have lower occupancy rates. Low-margin rural hospitals are also more likely to be in states that have not expanded Medicaid under the Affordable Care Act (ACA). According to new analysis by the Center for American Progress, future hospital closures would reduce rural Americans’ proximity to emergency treatment. Among low-margin, rural hospitals—those most likely to close—the majority of those with emergency departments are at least 20 miles away from the next-closest emergency department.
This report first discusses the role that hospitals and emergency care play in rural health care as well as trends in hospital closures. It then uses federal data to examine differences in the financial viability of rural and urban hospitals and the availability of hospital-based emergency care in rural areas. The final section of this report offers policy recommendations to improve health care access and emergency care for rural residents.
Rural hospitals have been closing at an unprecedented rate
From 2013 to 2017, rural hospitals closed at a rate nearly double that of the previous five years.6 (See Figure 1) According to the Government Accountability Office (GAO), recent rural hospital closures have disproportionately occurred among for-profit and Southern hospitals. Southern states accounted for 77 percent of rural hospital closures over that time period but only 38 percent of all rural hospitals in 20137
Hospital closures may deepen existing disparities in access to emergency care. Closures are more likely to affect communities that are rural, low income, and home to more racial/ethnic minority residents.8 Although about half of acute care hospitals are located in rural communities and the other half are located in urban areas,9 rural residents live 10.5 miles from the nearest acute care hospital on average, compared with 4.4 miles for those in urban areas.10 According to a poll by the Pew Research Center, about one-quarter (23 percent) of rural residents said that “access to good doctors and hospitals” is a problem in their community, while only 18 percent of urban residents and 9 percent of suburban residents said it was a problem.11
A variety of factors influence hospitals’ sustainability. Thanks to medical and technological advances, conditions that once required hospitalization can now be treated in an ambulatory care center or a physician’s office. University of Pennsylvania professor and CAP nonresident senior fellow Ezekiel Emanuel has argued that one reason hospitals are closing is that “more complex care can safely and effectively be provided elsewhere, and that’s good news.”12 As a whole, the hospital industry remains highly profitable, and hospital margins are at their highest in decades.13
Evidence on the relationship between hospital closures and health outcomes is mixed. A 2015 study of nearly 200 hospital closures in Health Affairs found no significant changes in hospitalization rates or mortality in the affected communities, whether rural or urban.14 More recent studies have found an association between rural hospital closures and increased mortality. Harvard researcher Caitlin Carroll showed that rural hospital closures led to an overall increase in mortality rates for time-sensitive health conditions,15 and Kritee Gujral and Anirban Basu of the University of Washington found that rural hospital closures in California were followed by increases in mortality for inpatient stays.16
In rural areas, hospitals face additional challenges to their viability, including lower patient volumes; higher rates of uncompensated care; and physician shortages.17 In addition, rural patients tend to be older and lower income.18 Rural hospitals tend to be smaller, serve a higher share of Medicare patients, and have lower occupancy rates than urban hospitals.19 Rural hospitals commonly offer obstetrics, imaging and diagnostic services, emergency departments, as well as hospice and home care,20 but patients needing more complicated treatment are often referred to tertiary or specialized hospitals. In fact, rural patients are more likely to be transferred to another hospital than patients at urban hospitals.21
Most urban hospitals are reimbursed under the prospective payment systems (PPS) for Parts A and B of Medicare. Through both the inpatient and outpatient PPS, the Centers for Medicare and Medicaid Services (CMS) reimburse hospitals at a predetermined amount based on diagnoses, with adjustments—including those for local input costs and patient characteristics.22However, rural hospitals often face higher costs due to lower occupancy rates and provide care to a higher percentage of patients covered by Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). Such hospitals may be eligible to receive higher payments from Medicare if they qualify as a Sole Community Hospital (SCH) or Medicare-Dependent Hospital (MDH).23
Another form of financial relief for rural hospitals is obtaining designation as a Critical Access Hospital (CAH), which Medicare reimburses based on cost rather than on the PPS.24 To qualify as a CAH, a hospital must provide 24/7 emergency services; maintain no more than 25 beds; and serve a rural area that is 35 miles from another hospital.25 Medicare reimburses CAHs at 101 percent of reasonable costs, rather than through the inpatient and outpatient PPS structures.26 As of 2018, there were 1,380 CAHs nationwide,27 accounting for about two-thirds of all rural hospitals.28
Even with cost-based reimbursement, however, some CAHs are unable to sustain the costs required to maintain inpatient beds.29 The 25-bed limit for CAHs prevent participating hospitals from eliminating inpatient services and restrict their ability to expand in response to fluctuations in community populations or care volumes. Other challenges facing rural hospitals include lacking sufficient patient volume to maintain high-quality performance for certain procedures and pressure to drop high-value but poorly reimbursed services such as obstetrics while maintaining low-volume, high profit services such as joint replacement procedures. 30
A key way that states can support struggling rural hospitals is by expanding Medicaid under the ACA. Expanding Medicaid increases coverage among low-income adults, 31 which in turn reduces uncompensated care costs for hospitals32 and allows financially vulnerable hospitals to improve their viability.33 Consistent with other recent studies,34 the GAO concluded in a 2018 report on rural hospitals that those “located in states that increased Medicaid eligibility and enrollment experienced fewer closures.”35
Rural hospitals are cutting back on services
Rural hospitals in different states have responded to financial pressures in a variety of ways, trying to balance community needs with financial viability. For many hospitals this has meant cutting inpatient obstetric services, leaving more than half of rural counties without hospital obstetric services.36 For instance, in Wisconsin, falling birth rates led to 12 hospitals in the state closing their obstetric services in the past decade.37 In Grantsburg, Wisconsin, lower birth rates and an older community population led Burnett Medical Center to shut down its obstetrics services.38 In order to offer these services, Burnett Medical Center would have needed to keep a general surgeon on call to perform caesarean sections, and with just 40 deliveries in 2017, the hospital could not justify the expense.39 While the hospital will continue providing prenatal and postnatal care, it will refer patients to a facility in Minnesota for deliveries—a facility is almost 40 minutes away.40
In other communities, hospitals have been replaced by other types of health care facilities. For example, Appalachian Regional Healthcare System closed Blowing Rock Hospital in North Carolina in 2013. Three years later, it opened a 112-bed post-acute care center in Blowing Rock in response to demand for rehabilitation services and the aging population in the surrounding area.41
Financial data shows that rural hospitals are more likely to struggle
To compare the financial situations of rural and urban hospitals and examine how future rural hospital closures could affect the availability of emergency care, CAP analyzed data from the CMS Healthcare Cost Report Information System (HCRIS). The CMS requires all Medicare-certified hospitals to report their financial information annually. CAP used the HCRIS to examine the financial margins and other characteristics of 4,147 acute care hospitals for fiscal year 2017. Of these, 1,954 hospitals (47 percent) were in rural areas, while the remaining were in urban areas. Hospitals self-report their status in the HCRIS as either urban or rural, which the CMS defines as either inside or outside of a metropolitan statistical area, respectively.42 Further information about CAP’s hospital sample can be found in the Methodological appendix.
Hospital operating margins, which measure excess patient-related revenues relative to patient-related expenses, are often used as an indicator of financial health.43 A 2011 study by Harvard researchers Dan Ly, Ashish Jha, and Arnold Epstein found that the lowest 10 percent of hospitals by operating margin were 9.5 times more likely to close within two years compared to all others. 44 The same study concluded that hospitals with low operating margins were also more likely to be acquired or merge.45
In CAP’s hospital sample, the median operating margin was negative 2.6 percent among all hospitals, negative 0.1 percent for urban hospitals, and negative 4.9 percent for rural hospitals.46 Public hospitals and MDHs in the sample were more likely to have negative operating margins, consistent with what other studies have found.47 To analyze hospitals’ relative financial health across geographic areas, CAP ranked hospitals in the HCRIS sample based on operating margin, splitting them into three groups: the lowest 10 percent, the middle 80 percent, and the highest 10 percent. The range of operating margins for each group is shown in Table 1.
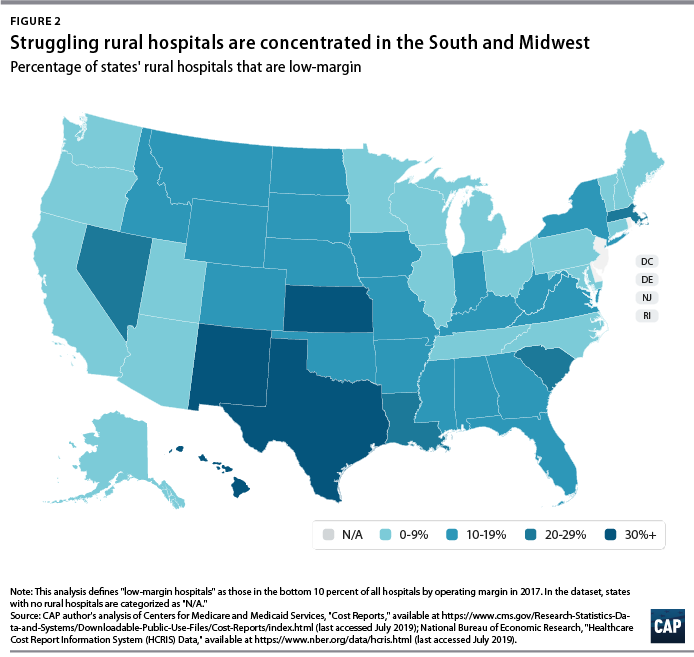
Rural hospitals are less likely to be financially healthy than urban hospitals. In 2017, rural hospitals comprised only 27.9 percent of the hospitals with operating margins in the highest decile but comprised 59.7 percent of the hospitals in the lowest decile. Southern and Midwestern states had the greatest proportion of rural hospitals with low operating margins, mimicking the geographic patterns in hospital closures that the GAO report identified. CAP finds that from 2015 through 2017, rural hospitals were consistently more likely than urban hospitals to fall in the bottom 10 percent of operating margins. CAP’s analysis also confirms that rural hospitals in states that expanded Medicaid had a higher median operating margin (negative 3.4 percent) than those in states that have not expanded Medicaid (negative 5.7 percent).
To examine commonalities among the hospitals most vulnerable to closure, CAP analyzed characteristics of the hospitals with low margins, defined as having an operating margin in the lowest 10 percent among all hospitals. Smaller, low-occupancy rural hospitals were most likely to struggle financially: nearly 1 in 6 (15 percent) of hospitals with 25 or fewer beds had low margins, and nearly one-fifth (17 percent) of hospitals with low-occupancy rates had low margins. (See Figure 3)
Emergency departments are on the front lines for rural health
In some emergency situations, hospital closures can be life-threatening, increasing the time and distance patients travel to receive care. Studies show that the probability of dying from a heart attack increases with distance from emergency care,48 and traumatic injuries are more likely to be fatal for rural residents than for urban ones.49
Rural residents are more likely than urban residents to visit the emergency department.50 A shortage of primary care providers; lack of public transportation infrastructure; shortages in preventive care; higher rates of smoking and obesity; and greater prevalence of chronic disease in rural areas all contribute to the greater utilization of emergency room care.51 As a result, emergency departments often stand in as the main source of care for vulnerable and low-income populations, especially for communities that face a shortage of primary care. 52 Among the dozens of rural hospitals that have closed in recent years, some served as the only emergency department in a community, according to MedPAC53
While freestanding emergency departments have proliferated,54 they are not filling the gap for rural emergency care. MedPAC found that, as of 2016, nearly all the country’s 566 stand-alone emergency departments were in urban areas and tended to be located in more affluent communities.55 Researchers at the North Carolina Rural Health Research Program found that the freestanding emergency department model was generally not viable in rural areas of the state due to low patient volumes, high rates of uninsured patients, and provider shortages.56 One limit on the growth of independent freestanding emergency centers is that they are not recognized in Medicare law and are therefore unable to bill the program, unlike hospital-affiliated off-campus emergency departments. 57
Future rural hospital closures would increase the distances that patients travel for emergencies
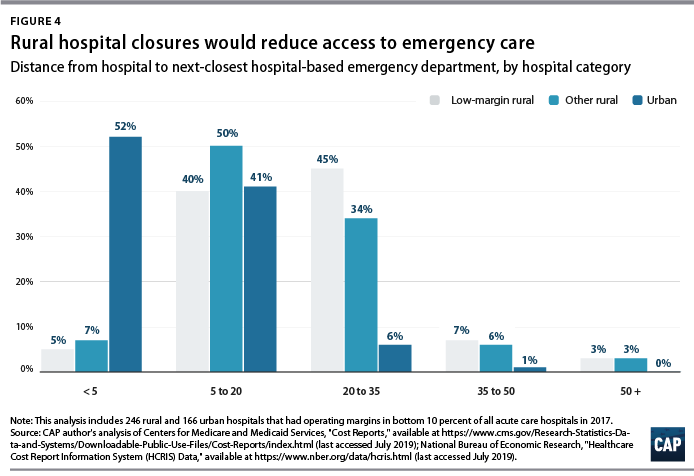
To better understand how future rural hospital closures could affect access to emergency care, CAP calculated hospitals’ distance to the next-closest hospital-based emergency department. CAP restricted its 2017 HCRIS data sample to the 3,616 acute care hospitals that provide 24-hour emergency services.58 Using addresses or coordinates provided in the HCRIS, CAP mapped each low-margin rural hospital to the next-closest hospital emergency department. Mapping strategies are detailed in the Methodological appendix.
Among the 222 low-margin rural hospitals, more than half (55 percent) were more than 20 miles away from the next-closest hospital-based emergency department, and one-tenth were more than 35 miles away. (See Figure 4). The average distance to the next-closest emergency department was 22 miles.
The disappearance of rural, low-margin hospitals would greatly increase patients’ travel distances for emergency care. Without other resources to fill the gap, some patients might forgo care they need and others would be forced to undertake an even longer journey to receive medical attention.
Policies to improve rural emergency and nonemergency care
As rural hospitals continue to close, it is crucial to preserve access to emergency care for rural Americans. The following section details a series of policy recommendations to support adequate emergency care and address care shortages in rural communities.
Expand Medicaid
Experience to date suggests that rural hospitals in those states that have not yet expanded their Medicaid programs under the ACA would benefit from Medicaid expansion through lower levels of uncompensated care and increased financial sustainability. Medicaid expansion is associated with improvements in health and a wide variety of other outcomes, including lower mortality, less uncompensated care, and lower rates of medical debt.59 According to the Kaiser Family Foundation, about 4.4 million adults would gain Medicaid eligibility if the remaining 14 nonexpansion states expanded their programs.60
Policymakers can also support rural communities and their hospitals by opposing efforts to repeal the ACA. If the Trump administration-backed lawsuit against the ACA were to succeed, 20 million Americans would lose health insurance coverage, and uncompensated care would rise by $50 billion, according to the Urban Institute.61
Create a greater number of rural emergency centers
To preserve access to emergency care, Congress could allow rural hospitals like CAHs to downsize to an emergency department and eliminate inpatient beds without giving up special Medicare reimbursement arrangements. Qualifying hospitals could transfer patients requiring inpatient admission to other hospitals, while continuing to offer some diagnostic imaging and other outpatient services.
One such proposal is the Rural Emergency Acute Care Hospital Act (REACH Act), bipartisan legislation proposed by Sen. Amy Klobuchar (D-MN) and Sen. Chuck Grassley (R-IA) that would create rural emergency centers.62 This designation would allow hospitals to provide only emergency care in rural communities and receive Medicare reimbursement at 110 percent of operating costs. Separately, MedPAC has recommended that rural hospitals located more than 35 miles from the nearest emergency department be allowed to convert to freestanding emergency departments while still being reimbursed at hospital rates.63
Institute global budgeting for rural hospitals
Under global budgeting, hospitals are paid a fixed amount rather than having their reimbursements based on the volume and types of services they provide.64 Global budgeting can reduce small, rural hospitals’ financial risk by providing them with a more predictable stream of revenue. In addition, payment reforms that include both hospital and nonhospital care can encourage communities to invest in services that are typically less generously reimbursed, such as preventive care.65
For example, in 2014, Maryland transitioned its acute hospitals from fee-for-service payments to a global budget.66 An evaluation of the global budget program showed that it reduced hospital expenditures relative to trend without transferring costs to other parts of the health care system.67 Future global budgets should emphasize improvements in population health and primary care,68 including ensuring that patients receive care in appropriate settings and reducing the number of avoidable hospital visits.
The Pennsylvania Rural Health Model is the first Medicare demonstration project to test the financial viability and community effects of a global budget for strictly rural hospitals.69 This six-year program aims to smooth out cash flow for 30 rural Pennsylvania hospitals on a monthly basis with the goal of enabling hospitals to meet community needs, especially for substance-use disorder and mental health services.70 With global budgets based on the previous year’s revenues, participating hospitals will have a more predicable stream of revenue. Importantly, the program allows hospitals to share in the savings that result from avoidable utilization.71
Improve transportation for rural residents
The lack of transportation infrastructure can lead rural residents to rely on ambulances and emergency rooms for nonemergency care. In nonemergency situations, patients often cite the lack of affordable transportation as a major barrier to care access.72 In order to fill the gap, payers and policymakers should consider efforts to utilize existing community transit resources for medical transportation or reimburse patients who use ride-sharing services in areas that lack public transit or taxi services. 73 Another option would be to formalize volunteer services for medical transit. Oregon offers a tax credit for volunteer rural emergency medical services (EMS) providers, who provide medical and transportation services analogous to those of volunteer firefighter programs.74 The CMS should also consider policies to better reimburse and expand the use of telehealth in remote areas to reduce patients’ burden of transportation.75Finally, the CMS should stop approving states’ requests to waive coverage of nonemergency medical transportation (NEMT) requirements under Medicaid.76 NEMT is vital to eligible beneficiaries’ access to care, including appointments for preventive care, chronic disease management, and substance-use disorder treatment.
Strengthen the rural health care workforce
Rural health care provider shortages contribute to poorer access to care and poorer quality of care in rural communities. While 20 percent of the U.S. population lives in rural areas, only 9 percent of primary care physicians practice in rural areas.77 Greater access to primary care providers in rural areas would improve quality of care and health outcomes while also reducing unnecessary emergency department visits.78
One way to assist rural areas would be to encourage health professionals to train and work in underserved communities. Federal funding for physician training should include reimbursements for community-based sites so that medical residents can rotate through nonhospital settings.79 Expanding the National Health Service Corps—which provides scholarships and student loan repayment for professionals who work in federally designated health professional shortage areas—could also help bolster the rural workforce. In addition, changes to immigration policy—such as expanding the Conrad 30 program that funnels immigrant doctors into rural and underserved communities, reforming H-1B visas to benefit high-need communities—could help alleviate rural areas’ shortage of medical professionals.80
Conclusion
Mounting closures of rural hospitals across the country are exacerbating the disparity in health care access between rural and urban areas. The financial vulnerability of the remaining rural hospitals suggests that the trend may continue, leaving shortages in emergency care and other hospital services.
Policymakers should support initiatives that allow remaining rural hospitals the flexibility to tailor their services to meet community needs and improve access to care for rural Americans.